
Introduction:
Seasonal Hyperacute Panuveitis (SHAPU) is a mysterious eye disease with grave prognosis, reported only from Nepal. Though it was reported for the first time in 1975,1-3 no definite etiopathogenesis has been established to date. It occurs as an outbreak in certain regions of Nepal in a cyclical pattern during the autumn season and peaks during the winter season (August–December) only in odd years. Thus, after the first outbreak of 1975, the next outbreaks occurred in 1977,1979, 1981, and so on and the last outbreak was reported in 2019. SHAPU predominately occurs among children4 and the youngest reported case is a 38- day-male baby.5 No gender predilection has been identified in SHAPU.4 All cases are mainly immunocompetent with no prior history of systemic or ocular illness/trauma.4, 6
SHAPU is very devastating and generally leads to the loss of sight within a week, followed by cosmetic disfigurement due to phthisis bulbi, which can have a significant emotional impact on the patient. The disease is so rare and less explored that there are only 12 articles upon it in the PUBMED to date. According to the SHAPU factsheet, >15,000 cases have been affected over the last 45 years.7
SHAPU Outbreak Period:
SHAPU occurs cyclically during the autumn season soon after the monsoon (August-November) and usually ends with the peaking of winter in December or January of the odd years.4
Presenting Visual Acuity:
Sudden onset of profound loss or drastic diminution of vision is a common presenting symptom of this disease. Usually, they present with vision of 3/60 or less but as the affected cases are predominately children, the accurate visual acuity assessment is often difficult.4
Ocular Manifestations In SHAPU:
SHAPU has characteristics symptoms and signs which makes it peculiar from the other uveitic condition. The clinical features are listed below-
Symptoms:
Unilateral eye
Sudden onset of red-eye with no/minimal pain but no discharge
Profound loss of vision in a week
The whitish glow from the center of the eye
Affected eye getting smaller in a few weeks
No prior history of surgery or trauma
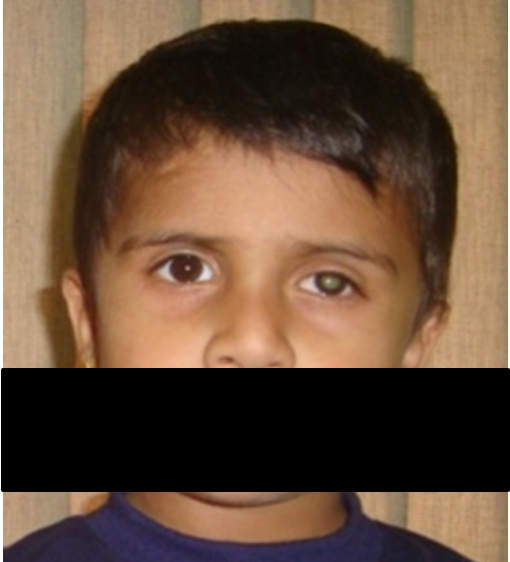
Figure 1: Unilateral red-eye with whitish pupillary light reflex
Signs:
Severe decrease in the visual acuity
Marked conjunctival congestion (circumcorneal and diffuse)
Dense fibrinous reaction/exudates in the anterior chamber
Mobile hypopyon in the anterior chamber
Significant posterior synechia with difficult to dilate the pupil
Leukocoria
Dense vitreous exudation with difficulty to visualize the fundus
IOP generally low to normal
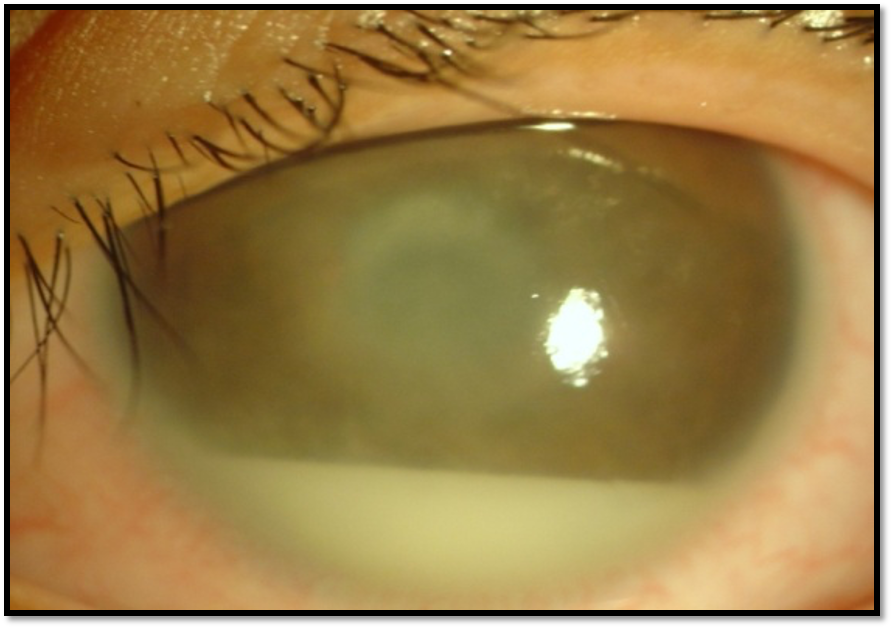
Figure 2: Dense fibrinous reaction with hypopyon in the anterior chamber of a SHAPU case
Uncommon Manifestations:
Iris muddy
Greenish pupillary reflex
Loss of corneal sensation
Greenish pupillary reflex
Hair like particles in ocular tissue
Laboratory Investigations:
Since the etiology of SHAPU is not well understood, there are no definite investigations to establish SHAPU rather clinical pattern recognition is more important.
Laboratory tests performed at the treating hospitals have identified a variable and confusing array of bacteria and viruses isolated from the aqueous and vitreous fluid samples from the eyes of affected patients.4 In some cases, Streptococcus pneumoniae and Acinetobacter, have been grown.8 However, viruses such as human Anelloviruses and Varicella zoster have also been reported in the vitreous fluid, but with no clear clinical significance,9, 10 while in many cases no organisms could be identified. Thus, various organisms have been reported by different workers,6, 9, 10 but lack of consistency in organisms reported makes it difficult for final attribution.
Newer molecular techniques including genomic sequencing to confirm or rule out microbes in the ocular fluid samples is underway to identify the definite microbes. Similarly, identification of immunological biomarkers and HLA typing from the blood and ocular specimen are also being planned to confirm its immunological association.
There are two arms of investigations for SHAPU as it could have an infective etiology or immunological etiology or a mixture of both. Thus, to establish it, there is a need for both microbial tests and immunological tests.
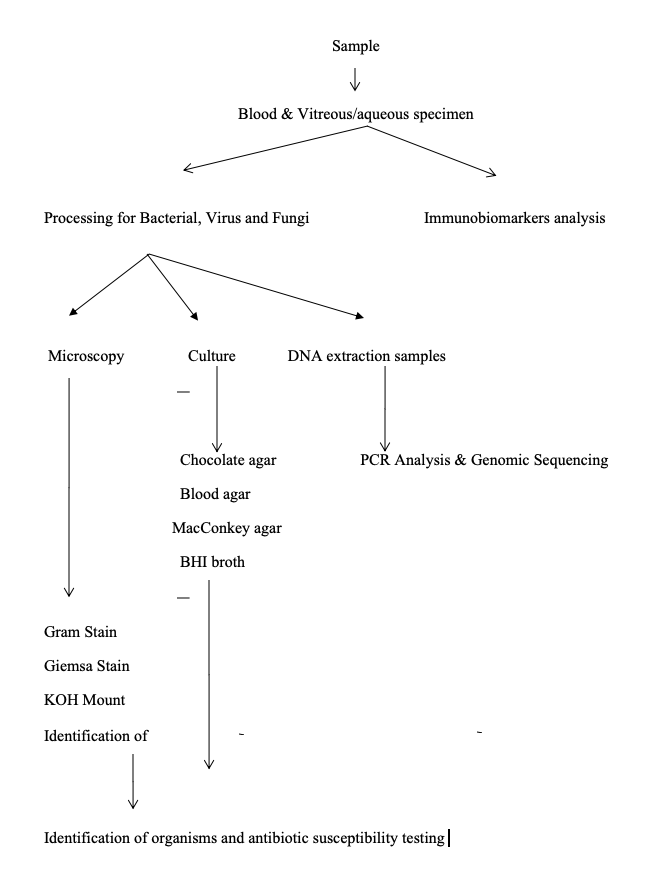
Figure 4: Flowchart for the microbiological processing and immunological analysis in SHAPU
Ocular Imaging Tests:
Ocular ultrasound (USG) is a very useful investigation tool in SHAPU because the fundus in such patients is difficult to visualize due to dense vitritis. USG shows hyperechoic shadows in the vitreous and retina, thickening of the ciliary body, and retinochoriodal complex with or without retinal detachment depending upon the stage of presentation.
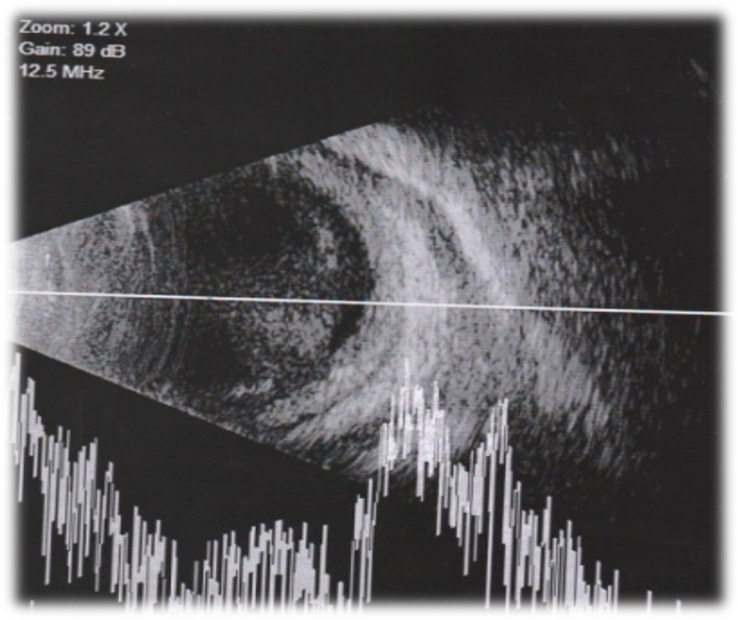
Figure 5: USG (A+B) scan showing dense hyperechoic shadows in the vitreous with thickened choroid
Optical Coherence tomography (OCT) is also an important tool to early detect the change in choroid and macula of SHAPU cases. But usually, it is difficult to perform in an early stage in the presence of hazy ocular media. The anterior segment OCT has been able to detect the hair particle in the cornea of a SHAPU case.11
Treatment:
Swinging between noninfective to infective etiology, there is no established protocol for the management of SHAPU cases.
In early reports, cases were treated with either singly or a combination of antibiotics, antiviral, immunosuppressive with uniformly poor results.4
Report from 200312 had shown better outcomes in 50% of the cases with early vitrectomy and then a report of 201013 reported regain of vision in 33.3% patients with topical, subconjunctival, oral, or intravitreal antibiotics and/or steroids but no surgical intervention.
With our experiences in various SHAPU outbreaks, we have developed a recent treatment protocol of immediate/urgent treatment with intravitreal antibiotics (Vancomycin (1 mg/0.1 ml) + Ceftazidime (2.25mg/0.1ml) ± steroid (Dexamethasone injection (0.4mg/0.1ml). Along with subconjunctival Vancomycin and Dexamethasone. If there is no sign of improvement by the 3rd day, pars plana vitrectomy ± lensectomy for diagnostic and therapeutic purposes is performed.
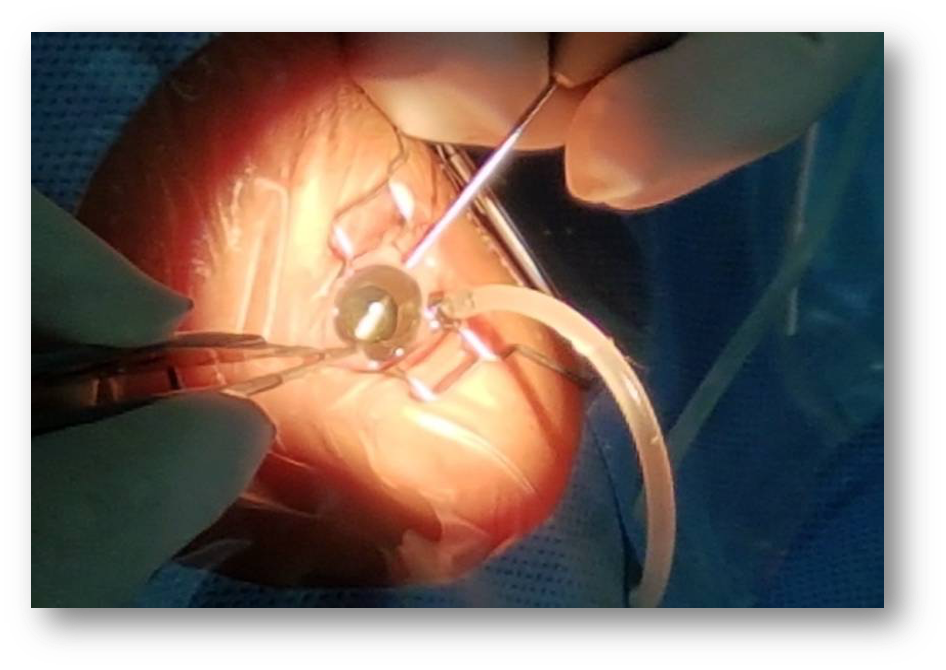
Figure 6: Undergoing Pars plana vitrectomy in a SHAPU case
Risk Factors of SHAPU:
In the 1980s, exposure to Tussock moths was reported as the primary risk factor for the disease.14 But later, other studies reported Gazalina moths as the suspect.8, 15 Tiny hairs of the moths have been identified in ocular structures in few patients including the cornea and anterior chamber. 6, 11
A multi-center, national case-control Epidemiological study conducted in SHAPU 2017 Outbreak has confirmed the white moths are the potential risk factors of SHAPU.16 SHAPU cases were 6.89 times more likely to report the history of direct contact with these white moths, making it the most important factor found in this study.
The moths might serve as vectors, carrying plant material acquired during their feeding time and this material may be the responsible agent that can induce infective and or immunological reactions within hours of contact with eye leading to hyperacute uveitis. Similarly, the spines and hairs of female moths bear toxic materials (histamine, acetylcholine, venom, pro-inflammatory products of cyclo-oxygenase, vaso-degenerative and fibrinolytic effects, serine proteases and pro-coagulant toxins) for natural protection of their eggs.17 These toxic materials may be capable of causing immediate hypersensitivity reactions in susceptible individuals. Additional research needed in this area, including the need for toxins & immune biomarkers analysis of the moth particles and its comparison with the ocular fluid samples of SHAPU.
Future studies also need to identify the genus of white moth, its lifecycle, and toxicology.

Figure 8: The female white moth with black striation and brownish spines and setae at the end to protect the eggs
Differential Diagnosis:
Conjunctivitis: It is often underlooked as unilateral viral conjunctivitis. But SHAPU is discharge less with circumcorneal congestion, intraocular reaction, and decreased vision, unlike conjunctivitis.
Endogenous Endophthalmitis: SHAPU cases are immunocompetent with no systemic foci of infection. All the blood parameters are normal.
Exogenous Endophthalmitis: SHAPU cases give no prior history of intraocular surgery or trauma to the eye.
HLA B 27 Uveitis: SHAPU is always unilateral with no recurrence in a ping pong manner.
Behcet’s disease: The hypopyon in SHAPU is fibrinous and not associated with the mouth/genital ulcer. SHAPU is always unilateral with no recurrence
Complication:
The serious gravity of SHAPU is associated with various complications if not treated on time.
Retinal detachment
Retinal necrosis
Hypotony
Cataract
Phthisis bulbi
Conclusion:
SHAPU continues to be a mysterious blinding disease in the absence of its known etiology. A multi-disciplinary, multi-centric team (national +international) consisting of epidemiologists, ophthalmologists, microbiologists, entomologists, health educationist should be constituted to undertake a comprehensive investigation and intervention so as to prevent the future outbreaks and timely management of the outbreaks with the standard treatment protocol.
NUGGETS
SHAPU Definition"Unilateral dischargeless red eye with severe intraocular reaction associated with significant vision impairment (in verbal children and adults) occurring soon after monsoon in the odd years, with contact history of white moths but no prior history of surgery or trauma”
Peculiarities:
- Odd years since 1975
- Seasonality (Post Monsoon season Aug-Dec)
- Predominantly children with no gender predilection
- Unilateral eye involved, No recurrences
- Sudden onset of Redness without discharge
- A dramatic loss of vision within 48 hours
- White Pupil with Red Eye
- No history of trauma or surgery
- Exact cause not known till date