1.jpg)

Although tales and myths of ocular surgery and organ transplantation appear in numerous ancient texts, the earliest accounts of ophthalmic diseases were written as a treatise by Sushruta, in the 6th century BC. Sushruta described 76 eye diseases, out of which 51 required surgical treatment. In the western world, the concepts of corneal surgery date back to Greek physician Galen (130-200AD).
The concepts to improve corneal clarity by surgery were developed over the next centuries and especially in the 17th and 18th centuries. But the major scientific progress and experimentation in the field of corneal surgeries happened in the 19th century. The progress in corneal surgery was hindered by a lack of understanding of immunology, asepsis, surgical procedures, and of course, the lack of proper instrumentation.
Emmert Wolf wrote over a century ago, “A man is only as good as his tools.” Early surgeons were hampered by a lack of proper surgical instruments. Over the centuries, innumerable ophthalmologists have contributed to the development and refinement of corneal surgical instruments, resulting in keratoplasty being the most commonly performed organ transplant, as well as the most successful.
One such contributor was Ramon Castroviejo (1904-1987). Castroviejo performed over 3000 grafts during his long and creative career. His contribution was largely in the design of new instrumentation, the advancement of surgical technique, and new experimental work. All the years of his practice, Castroviejo used Loupes to perform surgeries. However, he saw the emergence of microsurgery, and, recognizing that keratoplasty would be revolutionized by the advent of the operating microscope, he began to miniaturize his instruments. He worked with Ethicon (a suture manufacturer), towards the development of fine, atraumatic corneal sutures. Castroviejo also contributed to other areas of ocular surgery besides keratoplasty and also to the development of eye banking. In 1980 and 1981, Castroviejo was busy organizing the Eye Bank of Madrid and the research department of the Mediterranean Foundation. He was true to his beliefs and he made sure that his corneas were donated after his death.
With the advancement in microsurgical techniques and instruments, modern-day surgeons are transplanting layers of the cornea which are just a few microns thick like, the Bowmans layer transplant for keratoconus and DMEK and PDEK for endothelial dystrophies.
In this article, we are going to learn about how to identify an instrument, what are its uses, and its advantages and disadvantages if any. Also covered are the basics of sterilization, metals used in making instruments, and surgical steps as ready reckoners.
Which metals are used for making corneal surgical instruments?
Metals used in making corneal instruments should have the following properties-
Malleable: can be shaped without flaws
Ductile: as the instruments are thin and delicate
Satin finish: easy to clean and shouldn’t harbor microbes
Inert: shouldn’t cause toxicity
The most commonly used metals are stainless steel and titanium. Platinum is also used in some instruments.
What method is used for sterilization of corneal instruments?
Sterilization is defined as the complete absence of any viable microorganisms including spores.
The objective of sterilization is to get rid of microorganisms since they cause contamination, infection, and decay. The sterilisation procedure should be chosen according to the type of item to be sterilized.
Cleaning and decontamination, with thorough rinsing and flushing, should precede sterilization. During decontamination, all debris should be removed from the instruments. Instruments with lumens should be flushed off all debris and OVDs.
Below are the relevant details of the most commonly used methods of sterilization in a tabular form:
|
Method |
Time |
Advantage |
Disadvantage |
Suitable for |
|
Autoclave |
45min |
Kills spores |
Items must be heat and moisture resistance |
Gowns, dressing, drapes, metal instruments |
|
Hot air oven |
1.5-2hours |
Not much pressure builds up |
Prions not killed |
Metal instrument and sharps |
|
Ethylene oxide |
5psi-12hours 10psi-6 hours |
Low temperature |
Explosive, long duration |
Heat liable tubing, cyro, laser probe |
|
Plasma system |
Short cycle 74mins |
Low temperature |
Specific packing needed |
Same as ETO |
|
Glutaraldehyde |
Vegetative pathogens -15min Spores-3 hours |
For heat liable equipment |
Irritant |
Metal instrument, plastic, glass |
In this article, for the ease of perusal, we have divided the corneal instruments in the following categories:
| Instruments used in OPD |
|
Surgical instruments
|
| Instruments used in Eye Bank |
Instruments used in Cornea OPD:
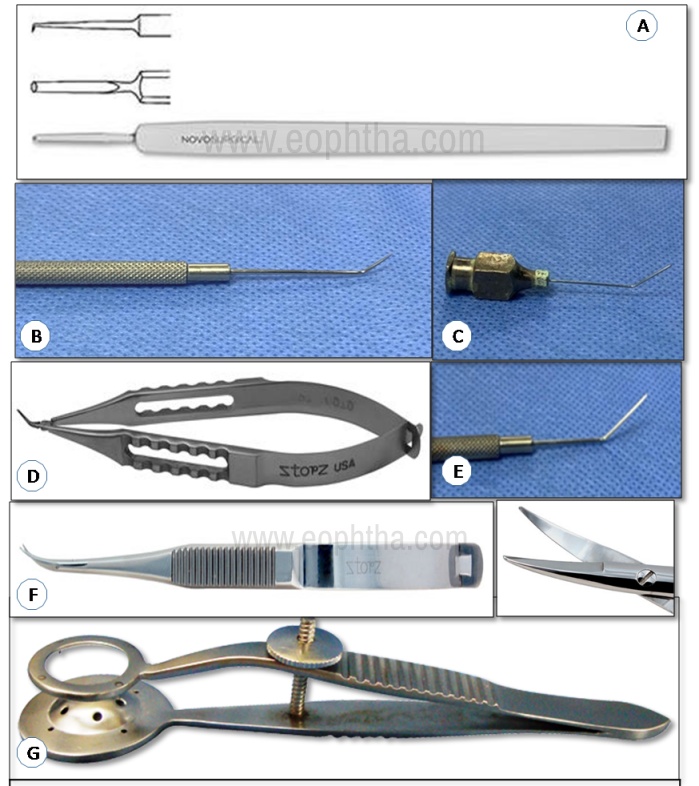
1. Ellis Foreign body spud:
Identification - Straight shaft, curved tip, 1mm rounded blade, flat handle
Uses
- To remove foreign body from the ocular surface
- To remove remaining rust ring from the cornea
Advantages –
- Atraumatic scraper
- The curvature of blade accommodates to the natural shape of the cornea
- Precise control
2. Barraquer wire speculum: (Description later in the text)
3. Suture set: (Description later in the text)
- Lim’s corneoscleral forceps
- Castroviejo’s scissors
- Westcott tenotomy scissors
- Kelmann McPherson forceps
- Jaffe tying forceps
4. Desmarre’s lid retractor
Identification - Solid plate design, with smooth C-shaped blades with blunt edges
The horizontal width of the blade decides the retractor size:
Size 0 = 11mm, size 1 = 13mm, size 2 = 15mm, size 3 = 17mm
Uses
- Double eyelid eversion for inspection and removal of any foreign body in the superior fornix
- Washing of chemical deposits in ocular chemical injury
- To open eyelids in the uncooperative patient for ocular examination
Advantages Concavity at the front end provide space for inspection and surgical manipulation
5. Nettleship punctum dilator
Identification - Long and slender with tapering pointed tips available in different sizes of 0.2, 0.3, 0.4mm tip diameter
Uses
- Mechanical punctum dilatation before sac syringing
- To diagnose punctal stenosis
- To dilate puncta before insertion of punctal plugs in dry eye cases
Advantages Facilitates the torsion force leading to rotatory movement
6. Castroviejo Punctum Dilator
Identification – It is a long and slender double-ended instrument with one medium and other fine ends.
Uses – Same as Nettleship punctal dilator
7. Lacrimal cannula
Identification - Short 23G cannula which can be straight or curved, with a hub at one end, the hub of the cannula is attached to a disposable syringe.
Uses – Syringing of lacrimal duct to check for patency
Advantages – End opening port for direct irrigation and a tip for ease of entry into the undilated punctum
13mm length makes it ideal to probe and irrigate the proximal lacrimal system
8. Epilation forceps:
Identification Stout stainless steel instrument with flat plane tips and a spring action handle
Uses Removal of eyelashes in cases of distichiasis, entropion, etc.
Advantages
- Spring tension handle for greater control
- Secures eyelashes at the root to avoid breakage
- Smooth edges to reduce the risk of trauma
9. Eyeshield:
Identification Made of plastic or acrylic, can be translucent or opaque, ventilated or non-ventilated, sterile or non-sterile, and shaped specifically to cover either eye
Uses Protection of the eye after surgery or trauma
Advantages
- Universal eye shield i.e. it accommodates either eye
- Provides impact resistance
- Protects the eye after surgery or trauma

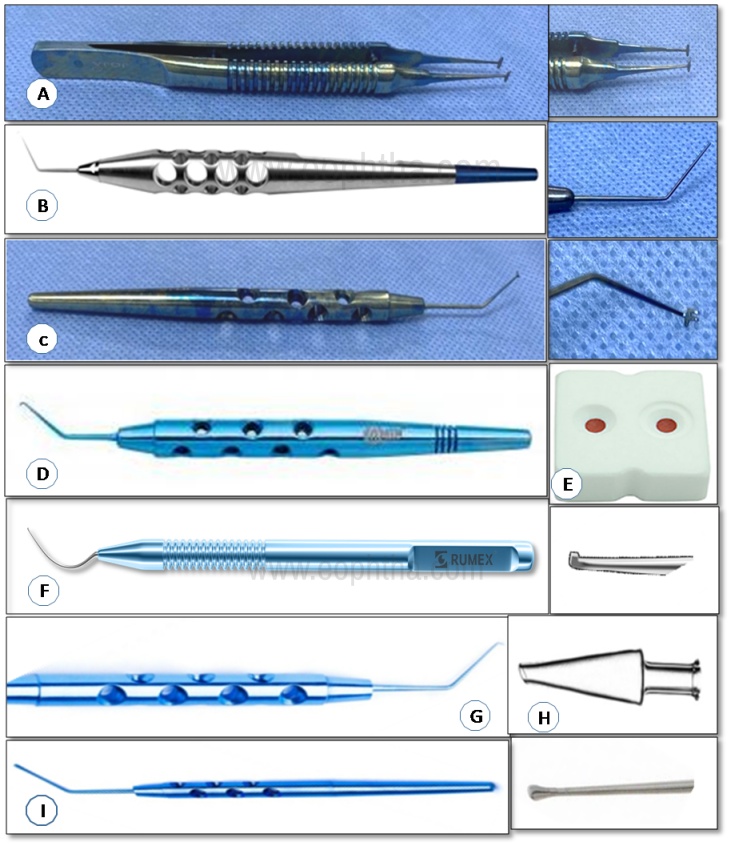
A. Ellis foreign body spud B. Barraquer wire speculum C. Desmarre’s lid retractor D. Lacrimal cannula E. Epilation forceps F. Eyeshield G. Nettleship and Castroviejo punctum dilator
Basic instruments used in all corneal surgeries:
Speculums:
A speculum consists of two limbs with adjustable or non-adjustable mechanism, joined at one end and open/closed/wired/solid blades at the open ends.
The adjustable variety contains a guard or a locking mechanism with a screw, by which the width of the open end of the speculum can be adjusted. The non-adjustable variety usually has a spring mechanism.
Adjustable: Lieberman, Knapp, Lancaster, Williams, Castroviejo, etc.
Non-adjustable: Wire-speculum - Barraquer, Kratz-Barraquer, Alfonso etc.
10. Barraquer wire speculum:
It is the most commonly used eye speculum. Available in pediatric (14mm) and adult sizes (16-18mm)
IdentificationStainless steel wire speculum with open blades without a lock or a screw
Uses To separate the eyelids for:
- Examination in uncooperative, very old or very young patients in OPD
- Corneal foreign body removal
- Examination in cases of chemical injury, thermal injury etc.
- To facilitate wash with normal saline in cases of chemical injury, foreign body entry etc.
- Intraocular surgery like cataract, glaucoma etc
- Extraocular surgery like squint surgery, pterygium surgery, ocular surface procedures etc.
Advantages
- Universal, can be used in both eyes
- Self-retaining
- Lightweight – Doesn’t cause an increase in IOP in intraocular procedures
11. Liebermann self-retaining speculum:
Identification Adjustable speculum with 17mm open blades and straight shaft. Also available in pediatric size. Lid tension is adjustable with thumb-screw control.
UsesMainly used in corneal surgeries like pterygium excision, DALK, ALTK
Advantages
- Can be used for both the eyes
- Screw adjustment holds the speculum opens
- Controlled retraction
Disadvantages Greater rise in IOP, as exerts more pressure on the lids
12. Williams self-retaining eye speculum:
Identification Adjustable speculum with 14mm blades. Blades are spring controlled with screw-type locking mechanism.
Uses
- Ocular surface procedures which needs maximum exposure of palpebral aperture
- Intraocular procedures with closed AC like DALK, ALK etc.
Advantages
- Self-retaining
- Fenestrated blades ensure enhanced visibility
- Curved to follow the eye contour
- Self-locking
- Can be used for both the eyes
- Controlled retraction
DisadvantagesGreater rise in IOP, as exerts more pressure on the lids
13. Kratz-Barraquer eye speculum:
Identification - Wire speculum, with spring tension open K-wire blades
Uses – Similar to Barraquer wire speculum
Advantages –
- Spring tension for easy use
- Smooth polished edge to minimise patient trauma
- Open blades provide easy access to instruments and phaco probe
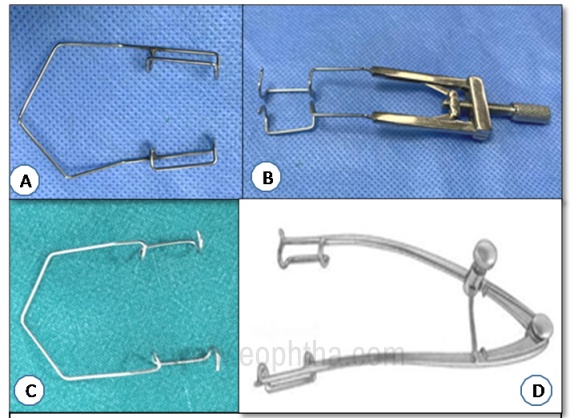
A. Barraquer wire speculum B. Liebermann self-retaining speculum C. Kratz-Barraquer speculum D. William self-retaining speculum
Needle holders:
Consist of four principal parts
- Handle – Generally cross serrated for a firm grip
- Hinge – Can be with or without lock
- Jaws–Can be delicate or stout
- Tips – With a groove to accommodate the body of the needle
14. Castroviejo’s needle holder:
Identification –Slender, spring action-based, needle holder with smooth jaws, and flat cross serrated handles
Uses
- Suturing delicate tissues like cornea, sclera, conjunctiva, etc
- Suturing AMG
- To make needle cystitome
Advantages
- Fine serrations for better grip
- Locking mechanism available in some models
- Fine, delicate jaws don’t cause damage to fine needles- ideal for suturing with finer sutures (10-0 nylon, 8-0 vicryl, etc)
15. Barraquer’s needle holder:
Identification- Spring action based needle holder with a non-locking, cross serrated grip handle, and curved delicate jaws, and a blunt tip
Uses
- Suturing delicate tissues like cornea, sclera, conjunctiva, etc
- Suturing AMG
- To make needle cystitome
Advantages
- Fine serrations for better grip
- Fine, delicate jaws don’t cause damage to fine needles- ideal for suturing with finer sutures (10-0 nylon, 8-0 vicryl etc)
16. Arruga needle holder:
Identification - Flat handle with a triangular design with a lock with thumb release, and serrated jaws
Uses
- For passing stay sutures in surface procedures
- For passing superior rectus and inferior rectus sutures in keratoplasty
Advantages
- Sturdy lock mechanism to hold the needle firmly
- Stout serrated jaws for thicker needles (4-0 silk etc)
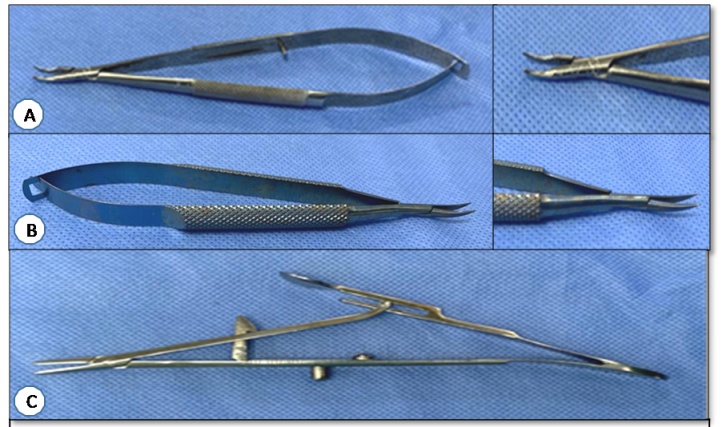
A. Castroviejo needle holder and tip B. Barraquer needle holder and tip C. Arruga needle holder
Scissors:
The scissors consists of four principal parts-
Handle – Part, where the instrument is gripped by the surgeon, can be hinge based/ spring-based or ribbon-shaped.
Pivot – Central point or axis
Blades - Can be either straight, angled, or curved
Tip – Working end of the scissors, can be pointed or rounded or blunt
17. Westcott tenotomy scissors: (aka conjunctival scissors)
Identification– Stout handles with a spring mechanism, with straight or curved blades and sharp or blunt tips
Uses– Delicate dissection, cutting and undermining conjunctiva in various surgeries
Advantages - Lightweight, blunt tips help in fine dissection during peritomy and protects the underlying structures.
18. Castroviejo’s corneoscleral scissors:
Identification – Delicate scissors with curved and angled blades kept apart by a spring action and a flat squeeze handle. Lighter than Westcott’s scissors with smaller blades.
Available in straight, left, and right variants.
In the left and right variants, the lower blade is 0.5mm longer than the upper blade, to match the curve of the limbus.
Uses- Wound enlargement in ECCE, penetrating keratoplasty, DALK, etc
Advantages - Curved blades help in the cutting of the cornea along its curvature
19. Vanna’s scissors:
Identification– Small, delicate scissors with flat or curved blades, serrated grip handles with a spring mechanism and a sharp tip
Uses– Procedures requiring delicate cutting like-
- Iris abscission, iridectomy, sphincterotomy, capsulotomy (envelope technique), etc.
- Prolapsed vitreous (manual vitrectomy)
- Cutting of pupillary membranes
Advantages –
- Small blades minimize trauma to adjacent structures
- Sharp tips to quickly and precisely cut the delicate tissues
20. Stevens tenotomy scissors:
Identification - Ring type, long handles with straight and curved blades with a blunt tip
Uses - Dissection and separation of tissue, used to create tissue plane in ocular surface procedures, symblephera release, for implantation of device like scleral bands, glaucoma drainage device etc.
Advantages – Blunt tip protects the underlying and surrounding structures
21. De Wecker’s iris scissors:
Identification- Fine scissors with right-angled blades, blades kept in V- shape due to spring action. Slightly larger than Vanna’s scissors.
Uses
- To perform iridectomy, iridotomy, iris abscission
- To cut the prolapsed form of the vitreous and pupillary membrane
Advantages
- Blades are directed at the right angle to arms so minimize the trauma to surrounding tissue
- The right-angled pattern of the blades provides a better field of vision
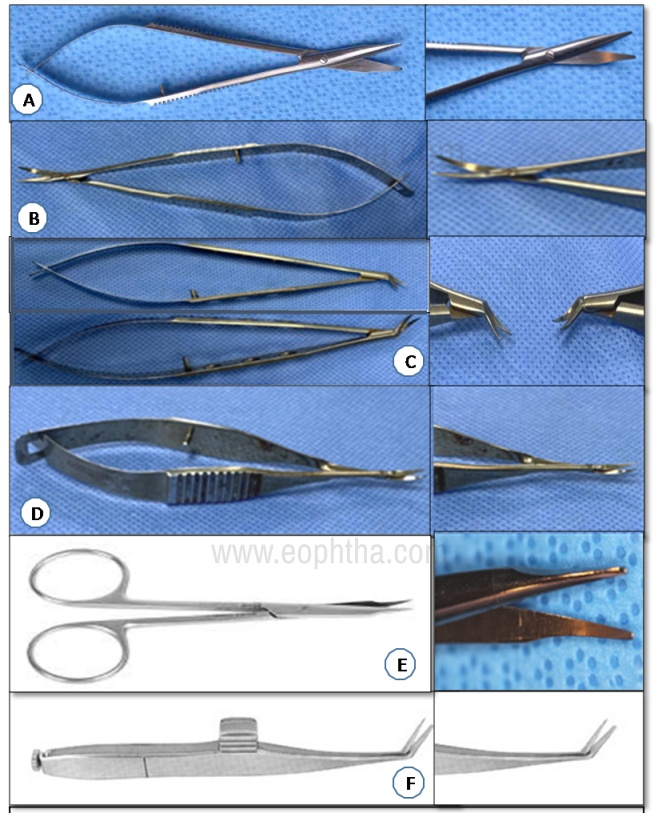
A. Westcott tenotomy scissors B. Castroviejo corneoscleral scissors with C. left and right scissors D. Vanna’s scissors E. Steven tenotomy scissors F. De Weckers scissors
Forceps:
Forceps are two-bladed instruments with a handle used to grasp or compress the tissue while performing surgery.
Consist of three principal parts:
Handle: Generally, cross serrated to provide a better grip to the surgeon. May have fenestrations to make the instrument lighter
Shaft: Connects the handle with the tip. It can be straight (direct access), curved (restricted access), angled (access at angle), cross action (maximum tip opening with a small incision)
Tip: Working end of forceps. Can be:
- plain (for removing cilia),
- serrated (atraumatic grasp over tissue),
- platform(for tying, holding, burying, removing of sutures),
- notched(holding tissue, tube, needles),
- toothed (for grasping tissues) etc
22. Plain forceps:
Identification- Straight forceps, grooved and fenestrated handle and non-tooth tip
Uses
- Handling of delicate tissue like conjunctiva, Amniotic membrane etc
- For suture tying
Advantages- Atraumatic
23. Kelman Mc Pherson’s forceps:
Identification - Fine, medium-sized, plain, angled forceps, angled at 8mm from the tip. Serrated handle for better grip. Tip has a tying platform.
Uses
- For suture tying and burying
- Holding of the optic of IOL while insertion
- Grasping delicate tissue like a capsular flap, pupillary membrane, etc
- Grasping and manipulating fine sutures
Advantages- Has a tying platform and no tooth, making it ideal for grasping delicate tissue and tying fine sutures.
24. Jaffe’s suture tying forceps:
Identification - Can be straight or curved, with very fine jaws, a 6mm tying platform, flat handles with serrations and fenestrations
Uses
- For suture tying and burying
- Grasping delicate tissue like capsular flap, pupillary membrane etc
- Grasping and manipulating fine sutures
Advantages –
- Long tying platform ideal to handle monofilament nylon and prolene sutures
- Smooth jaws and long platform prevent injury to fine sutures
- Spring handle ensuring maximum control
25. Pierse Hoskins forceps:
Identification – Small, fine forceps with 6mm platform and a 0.2mm, precision notched tip
Uses – To hold conjuncti va and muscles during extraocular and intraocular surgery
Advantages - Less traumatic than other forceps
Disadvantages - Less firm grip
26. Lim’s corneoscleral forceps:
Identification - Grooved handle, curved forceps with 1x2 teeth at tip for holding tissue
Uses - For holding the cornea or scleral edge while suturing. One of the most commonly used forceps in corneal surgery.
Advantages – Very fine teeth grasps the tissue edge gently but firmly, so prevents slipping and damage
27. Colibri forceps :
Identification – Colibri is an italian word meaning bird. Fine forceps with a grooved handle, flat platform, angulated /curved shaft giving it a bird beak like appearance, and a straight tip with 1x2 teeth
Uses - For holding cornea/sclera edge while suturing
Advantage -
- Able to fit within incisions as narrow as 1.8mm
- Bowed, thin arm provides clear view of the surgical site
- Fine teeth ideal for holding delicate tissue, prevents damage
28. Dastoor’s superior rectus holding forceps
Identification – Stout forceps with a grooved handle, holes with the guard, S-shaped double curve near tip, 1x2 teeth
Uses - To hold superior rectus tendon while passing bridle suture, traction suture
Disadvantages – Can be traumatic
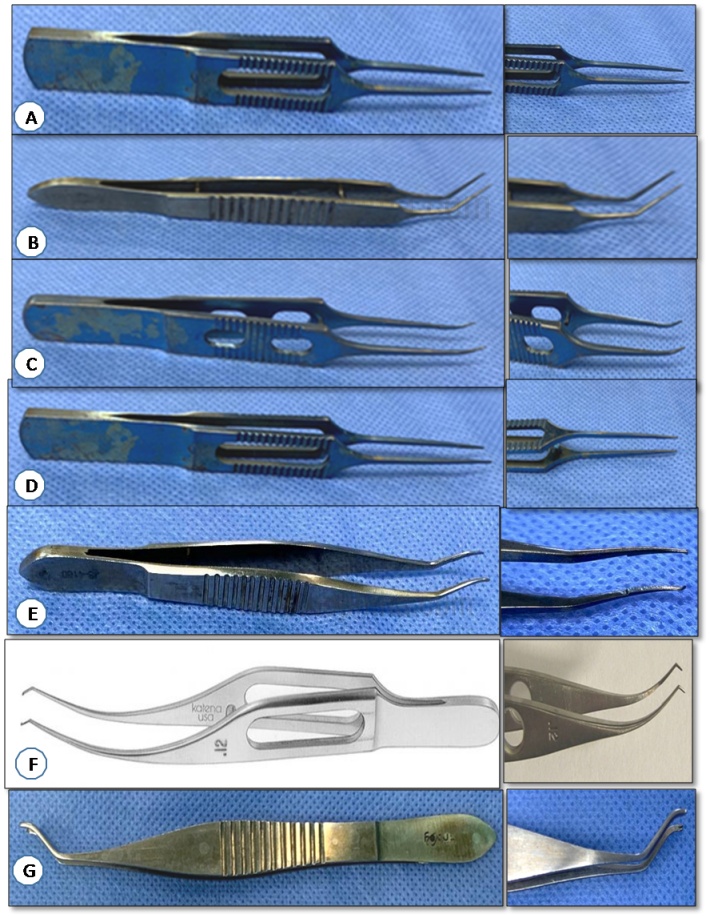
A. Plain forceps B. Kellman McPherson forceps C. Jaffe suture tying forceps D. Pierse Hoskins forceps D. Lim’s corneoscleral forceps E. Colibri’s forceps F. Dastoor’s superior rectus holding forceps
Cannulas:
By definition, a cannula is a thin tube inserted into a body cavity to administer medication, drain off fluid, or insert a surgical instrument.
It consists of:
Hub – Made of metal (reusable) or plastic (disposable), it connects to the IV tubing (for irrigation) or a syringe (for irrigation or aspiration).
Tube or shaft – It connects the hub to the tip, it can be straight, curved or angled, can have fenestrations
Tip – It is the working end of the instrument. It goes into the cavity for irrigation, aspiration or other manipulations. Mostly blunt.
29. Rycroft air injection cannula:
Identification – Can be 27G or 30 G, blunt tip, 45 degrees angled tube, 5mm from tip to bend disposable.
Uses – For injection of air to form the anterior chamber during various intraocular procedures
Disadvantages - Single use
30. Hydrodissection cannula:
Identification - Range in size from 23G to 30G, 32 degrees angled shaft, 8mm from bend to tip, with flattened smooth oval-shaped tip. The tip is designed to separate the cortex from the capsular bag. The flat end allows gentle insertion and suitable irrigation.
Uses –
- Nucleus hydrodissection and delineation during cataract surgery
- To hydrate the wound to form the anterior chamber
- To irrigate and moisten cornea during the procedure
31. Visco-elastic cannula:
Identification - Disposable, 23G to 27G, 11mm from bend to tip, have blunt tip. Ready to use, for intraocular injection of OVD substances
Uses - To inject OVD substance during intraocular surgery

A. OVD Cannula B. Hydro-dissection Cannula C. Rycroft air injection Cannula
32. Simcoe’s irrigation-aspiration cannula:
Identification - Has a 15mm long 0.3mm diameter aspiration port, and a 21G to 23G front opening irrigation port. Aspiration through tubing hub attached to a 2-5ml syringe and irrigation through a lure-lock hub
Uses
- Irrigation and aspiration of cortex in cataract surgery
- Washing of OVDs at the end of the surgery in various procedures like cataract, PK, DALK etc
- AC wash to remove exudates, hypopyon etc from the anterior chamber
- Can be used for posterior capsule polishing
Advantages
- Irrigation, as well as aspiration, can be done by a single instrument, so no need to make extra openings.
- Continuous irrigation during aspiration protects the endothelium and keeps the anterior chamber formed and maintained thus avoiding sudden decompression.
Other variants: Reverse Simcoe, U shaped Simcoe (right or left)

Knives and blades:
33. Bard Parker handle:
Identification - Flat serrated handle, long cylindrical end with two longitudinal grooves for sliding over of any scalpel blade (11No, 15No, etc)
Uses - To mount and handle surgical scalpel blades for making incisions in various extra-ocular and intraocular procedures
Advantages – A single handle can be used to mount different blades, reusable
34. 15-degree blade:
Identification - 15 degree angled, stainless steel blade, smooth plastic handle, and lancet-shaped tip
Uses - For scleral incision, side port incision etc.
Advantages - Makes a micro-track which is self-sealing
Disadvantages - Single use
35. Crescent knife:
Identification – Disposable, single-use metal blade, with smooth plastic handle. Rounded blades with bevel up and a cutting, dissecting edge and tip.
Uses
- For making scleral tunnel during SCIS, DMEK
- For making scleral flaps in trabeculectomy, SFIOL, iridolysis repair
- For dissection of the head in pterygium surgery
- For dissection into the limbus in Simple limbal epithelial transplant (SLET)
- For lamellar dissection in keratoplasty
Advantages –
- Makes a self-sealing wound.
- Beveled tip follows the contour of sclera and cornea
Disadvantages – Single use
36. Tooke knife:
Identification – Flat serrated handle, ending in a short, flat blade with a blunt edge. Overall length is 119mm, with a 3x28mm smooth blade
Uses –
- To separate conjunctiva at limbus during various procedures
- To make a pocket for initiation of lamellar dissection
- Can be used for removal of corneal foreign body
Advantages – Flat, blunt edge minimize trauma to surrounding structures
37. Keratome
Identification - Disposable, single-use metal blade, with smooth plastic handle. Have a triangular blade with cutting edges and a sharp tip.
Sharp angled/straight/curved/ pointed arrow-shaped blades
Available in sizes 1.2mm to 3.5mm
Angled at 45 degrees to handle
Uses
- Making corneal incision of various dimension and depth
- Anterior chamber entrance
- Wound extension
Advantages – Makes precise size entry into the anterior chamber
Disadvantages – Single use
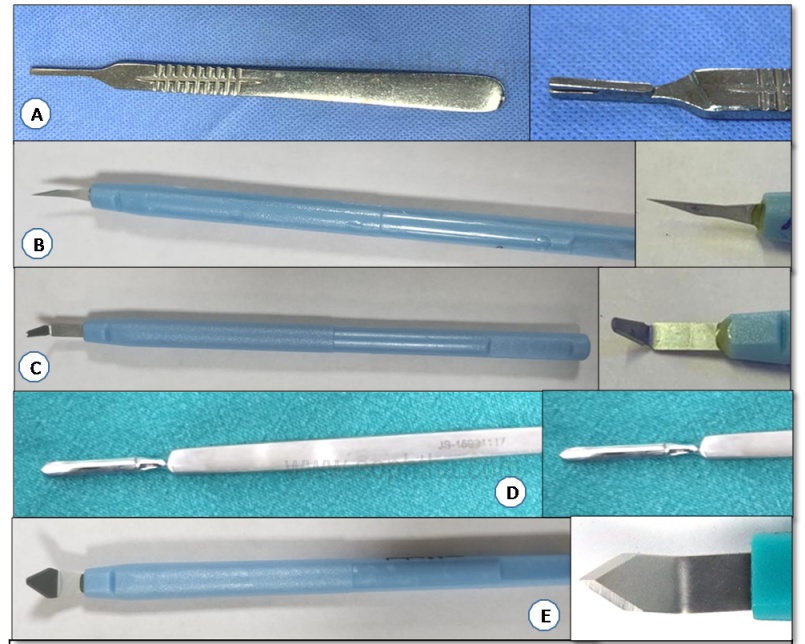
A. Bard Parker handle B. 15 degree side port blade C. Crescent knife D. Tooke knife E. Keratome
Others:
38. Castroviejo calipers:
Identification - Dividers like instrument with one fixed arm that is attached to a graduated curved scale in millimeters and another movable arm
Uses-
- Measurement during squint, ptosis, pterygium, scleral bucking, corneal surgeries
- To measure the size of excised pterygium defect for calculating graft size
- Intraoperative measurement of the size of corneal opacity or lesion
- Determine the length of scleral incision in SICS
- Determine the distance from limbus for intravitreal injection, vitrectomy ports
- Measure corneal diameter
- To measure laceration wound in globe injury
- To measure the size of host incision for appropriate trephination in PK, DALK, etc
Advantages – Portable, accurate when properly calibrated

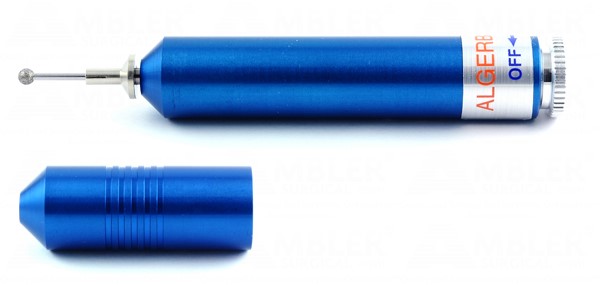
39. Electrocautery probe:
Mechanism - Heat is generated through an electric current and flows to the metal tip to coagulate blood vessels and stop bleeding.
Two forms are available -unipolar and bipolar
Unipolar cautery is applied through a handheld active electrode and travels back to the generator through an inactive electrode attached to the patient (the grounding pad), so the patient is part of an electric circuit
In bipolar cautery, the current is passed between one tip of the forceps to the other, hence limited amount of tissue is cauterized
Identification - Metal insulated handle, ending at a prong, foot pedal/ hand-held control button, monopolar has single tip, while bipolar has forceps prong.
Uses –
- Commonly used for hemostasis in various surgeries
- Can be used to induce punctal stenosis in patients with dry eye
- Used to closed conjunctival incisions
- Can be used as a surgical marker
- Can be used as cutting cautery for symblepharon release
Advantages – Less tissue damage as compared to heat ball cautery
Disadvantages - Current spread is more with monopolar cautery, hence causes more tissue damage

40. Barraquer iris Spatula:
Identification - 0.5mm diameter, angled tip with a gently curved flat spatula, and a hexagonal serrated handle
Uses –
- To hold the iris in place while manipulating the lens capsule and nucleus
- To reposit the iris back in place if coming through the incision site
- To break posterior synechiae
- To break peripheral anterior synechia
Advantages – Angled tip for easier manipulation while minimizing surgical obstruction

41. Skin marker pen:
Identification – Purple surgical skin marker pen with Gentian violet ink, with fine and standard tip options.
Uses – To precisely mark the surgical site in various procedures:
- In pterygium surgery to mark the area of CLAU needed
- In SLET to mark the clock hours on the limbus
- To mark the trephine before cutting into host tissue
- In toric IOL and Limbal relaxing incision (LRI) to mark the clock hours
- In occuloplasty procedures like ptosis, entropion, ectropion etc
Advantages –
- Gentian violet ink is quick-drying and doesn’t run
- A broad range of applications due to the availability of a variety of tips

42. Illig symblepharon ring:
Identification - Made of smooth PMMA. Large decentred opening leave the cornea uncovered. Have 4 small lateral holes for eventual suture fixation. Size 1 to 10 available.
Individually packaged non-sterile. Sterilisable by:
[a]gamma irradiation
[b] gas (3% formaldehyde. max.60° steam)
[c] 10-minute bath in 3% hydrogen peroxide.
Uses-
- to prevent anticipated or recurrent lid/globe fusions
- in chemical injury
- after mucous membrane graft, fornix forming surgery

Instruments used in Pterygium surgery:
Trolley for pterygium excision with CLAU will have the following instruments:
|
Leibermann Eye speculum |
For proper exposure of palpebral aperture |
|
Lim’s corneoscleral forceps |
To hold the head, neck, or body of the pterygium |
|
Westcott’s tenotomy scissors |
To excise the neck of the pterygium |
|
Bipolar cautery |
To cauterise the active bleeders if needed |
|
Hockey stick blade |
To clear the fibrovascular tissue from the corneal surface |
|
Diamond burr |
To polish the corneal surface |
|
Castroviejo callipers |
To measure the CLAU needed to close the defect |
|
Skin marking pen |
To mark the area of CLAU needed |
|
Barraquer needle holder |
For suturing the CLAU (if glue not available or not used) |
|
Kelman Mc Pherson forceps |
|
|
Tying forceps |
43. Hockey stick microblade:
Identification - Hockey shaped blade width 1mm, ultra-sharp cutting edges. Available in re-usable as well as disposable variants. It should be kept perpendicular to the corneal plane during dissection.
Uses
- Epithelial debridement in procedures like Collagen cross-linking, PRK etc
- Pterygium excision
Advantages - Non traumatic, more control

44. Diamond burr:
Identification – Consists of a handpiece with motor and batteries, a chuck and a round, fine grit diamond burr with a cap. Burr is available in different sizes, largest upto 5mm in diameter. The motor provides the necessary torque for smoothly polishing the corneal surface
Uses - To smoothen the corneal surface in certain abnormalities involving the front layer of the cornea like:
- Recurrent corneal erosions and epithelial basement membrane dystrophy (also known as anterior basement membrane dystrophy and map-dot-fingerprint dystrophy)
- For rust ring removal
- For polishing the cornea after pterygium excision
Advantages – Can be performed in the office using topical anesthesia
Instruments used in penetrating keratoplasty:
Trolley for Penetrating keratoplasty will have the following instruments:
|
Barraquer wire speculum |
For adequate exposure of palpabral aperture |
|
Castroviejo callipers |
To measure the diameter of host area to be excised |
|
Teflon block |
To punch the donor cornea |
|
Trephine/ Endothelial punch |
|
|
Flieringa ring/ blepharostat |
To stabilize the globe (if needed) |
|
15-degree blade |
Paracentesis to enter the host anterior chamber |
|
OVD canula |
To fill the anterior chamber before trephination |
|
Radial marker |
To mark the host as a guide for sutures |
|
Trephine |
To mark and punch the host cornea |
|
Castroviejo corneo-scleral scissors (left and right) |
To excise the host cornea completely |
|
Patton’s spatula and spoon |
To transfer the graft from block to host |
|
Barraquer needle holder |
For suturing graft to the host, and burying of the sutures |
|
Colibri’s forceps/ Pollack forceps |
|
|
Kelman Mc Pherson forceps |
|
|
Jaffe suture tying forceps |
|
|
Portable keratometer |
To assess suture induced astigmatism |
|
Simcoe’s irrigation-aspiration cannula |
To wash the OVD from anterior chamber |
|
Deweckers scissors |
To perform peripheral Iridectomy (if needed) |
|
Rycroft air injection cannula/ Hydro cannula |
To form the AC with BSS or air |
45. Flieringa scleral fixation ring:
Identification – Scleral expansion rings made of stainless steel and polished finish. Available as a set of 8 rings from size 12mm to 23mm
Uses – They are sutured to the sclera with vicryl sutures before keratoplasty. Maintains the rigidity of the recipient’s globe after trephination and prevents collapse of the eyeball.
Advantages - Secures globe during open sky procedures like keratoplasty

46. McNeill Goldman scleral fixation ring and blepharostat:
Identification – Double wire ring with outer diameter 24mm, inner diameter 17mm, with retractor loops for upper and lower lids, and polished finish
Uses - To provide firm global support with only four strategically placed sutures during keratoplasty
Advantages - This ring features medial and temporal openings for greater access to the surgical field and two lid retractors to prevent eyelid closure by the patient

Trephines:
The word ‘trephine’ is derived from the Greek word ‘trypanon’ which means an instrument used for boring or making a hole. It is a surgical instrument with a circular blade.
Corneal trephines are small, circular saws that are used in keratoplasty to punch or cut a hole in the cornea.
They can be of the following types:
A. Hand-Held trephine –
Examples- disposable trephine, francheschetti-type blades
Available in a wide range of diameter from very small (1.5mm) to very large (16mm)
Disadvantages- reduced visual control under the operating microscope, thus centration may be inaccurate.
B. Motor trephine
Examples –
Mikro-Keratron
- Non-automated motor- driven trephine system for PK
- Rotation may start and stop by pressing down and releasing foot, wide range of trephine diameters are available
- Disadvantage – Depth of cut is not pre-adjusted , hence not used in lamellar keratoplasty
An artificial chamber maintainer is required for graft trephination
Asmotom
- Automated trephine system for PK
- Uses- trephination of recipient, donor eyes as well as corneo-scleral disc can be performed
- Advantage – cutting depth can be pre-adjusted
- Has marker to facilitate centration
- Cutter sets available in 5 different diameters (6-8.2mm)
- Vacuum is applied to both central and perpherial section of cornea
C. Suction trephines
Example - Hessburg-Barron suction trephine
Advantage- The depth of trephination can be predicted, one full rotation is assumed to achieve 250 microns of corneal depth
D. Guided trephines
New generation trephine- as they stabilize the globe at the limbus
Examples -
Krumeich guided trephine system (GTS)
Uses- PK, lamellar keratoplasty, and circular keratotomy
Advantage-
- Trephination of both donor and receipt cornea with the epithelial side up using artificial anterior chamber
- Pre-depth depth of trephination
Disadvantage – Difficult to apply in a patient with narrow lid fissure or deeply set eyes
Hanna trephine
Trephine attaches firmly to eye with help of suction applied to limbal and donor with an artificial anterior chamber
- Advantage – Uniform support over the whole cornea, hence prevent corneal vaulting, can trephine both donor and receipt cornea with epithelial side up , hence reducing shape disparity
E. Laser trephination –
Examples - excimer laser and femtosecond laser
Advantages –
- avoidance of mechanical torsion during trephination, hence provide smooth edges
- reduced host and donor decentration
- avoid deformation and compression of tissue during trephination
- can trephine unstable cornea (descemetocele, post-RK, keratoectasia )
47. Disposable corneal trephine:
Identification – Hard plastic cylindrical body with an ultra-sharp steel blade at one end. Available in sizes from 3mm to 17mm in diameter
Uses - Trephination of donor and recipient cornea during keratoplasty
Advantages – Being single-use, the blade doesn’t become dull and remains sharp for trephination
48. Castroviejo corneal trephine:
Identification - Suction fixation corneal trephine, it goes upto 250 micron depth with each 360 degree rotation, size 6 to 9mm with 0.5mm increments
Uses - Used for controlled complete or partial trephination of the host tissue
Advantages –
- Crosshairs for centration over the host cornea
- Consistency of cut is equal all over
- Can be used in perforated eyes
49. Hessberg Barron vaccum corneal trephine:
Mechanism – This trephine is connected to a vaccum syringe via small silicon tubing with a Luer-Lok hub. An inner ring and an outer ring forms a vaccum chamber, with the blade located 0.07mm inside the inner ring. The blade is mounted on a spoke adapter that allows the blade to precisely cut a depth of 0,25mm per each complete rotation.
Identification - Solid stainless steel blade which is permanently mounted in a nylon housing
The base of the punch has a circular groove for aspirating the epithelial side of the cornea, immobilizing it for the cutting. Blade placed on vacuum fixed donor and pressed with thumb to yield a sharply cut corneal button
Uses - Perform partial-thickness trephination
Advantages –
- Self contained with its own suction source
- Cross hairs allow accurate placement on the cornea
Disadvantages – Single use
50. Suction trephine:
Identification - Have cutting circular blades assisted by the manual suction mechanism
Uses - To trephine a circular corneal button of predetermined diameter
Advantages - Precise, uniform, perpendicular cuts
51. Endothelial punch:
Identification – Mechanical, stand like device that comes with a plunger to punch the donor button from the endothelial side. Used with a disposable trephine and Teflon block
Uses – For donor corneal button trephination from the endothelial side
Advantages –
- Universal, can be used with any size trephine from 6mm to 11mm
- Spring recoil mechanism present, so the trephine retract back after completion of cutting
A. Disposable corneal trephine B. Hessberg Barron vaccum corneal trephine C. Endothelial punch D. Suction trephine E. Castroviejo corneal trephine
52. Lieberman Teflon block:
Identification – White Teflon circular block with an internal concavity similar to the radius of curvature of the cornea and a drainage hole in the center.
Uses – Donor preparation and cutting. Used as a base for trephination of donor tissue
Advantages - Approximates corneal shape and so reduce tissue distortion
Disadvantages - Slippage at the time of cutting

53. Paton spatula and spoon:
Identification - Double-ended instrument with a flat handle, 15mm flat spatula at one end with an angled shaft, 8mm from bend to tip, and a curved 6mm teardrop-shaped spoon with three long openings at the other end.
Uses –
- Spoon end for holding the corneal button during transfer from Teflon block to host in keratoplasty
- Flat spatula is used for iris repositioning, to break synechiae etc.
Advantages –
The spoon end is designed to snugly hold the donor button
The openings in the spoon drain excess OVDs and prevent slippage

54. Pollack forceps:
Identification – Fine forceps with Colibri type, fenestrated, spring tension handle, two-point fixation, 2x2 teeth separated by 1mm (1.2, 1.5 mm in some models), and Pierse type tips. It can be confused with Colibri forceps.
Uses – Used as a fixation forceps during suturing in keratoplasty procedure.
Advantages – Fine teeth prevent injury and provide a firm grip

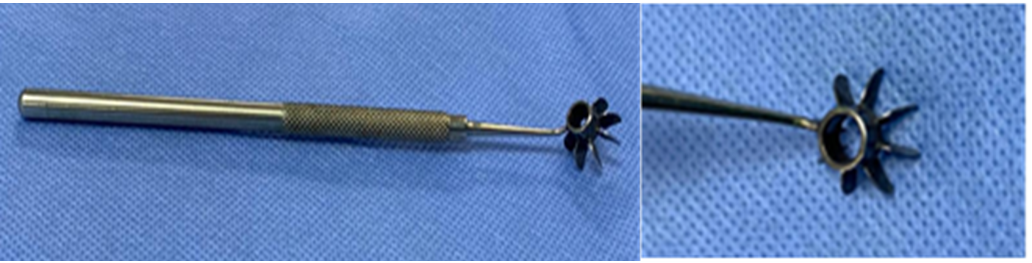
55. Osher Neumann radial marker:
Identification - 16 or 8 blades, on a central 4.5mm ring and fixed round cross serrated handle. It marks radial lines 4mm long. To be used with skin marking pen.
Uses –
- Helps in the orientation of sutures during keratoplasty
- Was previously used in Radial Keratectomy (RK)- not done nowadays
Advantages - Inner ring helps in centration, blunt blades allow minimal marking pressure
56. Bishop Harmon tissue forceps:
Identification - Straight delicate forceps with 1x2 teeth and a fenestrated handle
Uses - Grasp delicate tissue like cornea, conjunctiva, sclera, etc
Advantages – Fine teeth provides a gentle yet firm grip on the delicate tissue
57. Serrefine : (Dieffenbach-Serrafine Bulldog Forceps)
Identification – Short, stout forceps with blunt tips and serrated interlocking jaws
Uses –
- To hold and isolate specific suture in ocular surgeries
- As clamps for holding eye drapes
Advantages - Self-retaining forceps, easy handling, small size
58. Corneal fixation forceps: (Bores, Kremer)
Identification – Can be either straight or curved. U-shaped spread, 1x2 teeth at each tip 0.12mm
Uses – To firmly grasp the cornea while suturing
Advantages –
- Delicate 0.12mm teeth provide firm but gentle grip
- The U shaped tip provides visualization during suturing
59. PSU keratometer:
Identification – Flat shaft, a circular end with a central hole surrounded by concentric placido type rings.
Uses-Intra-operative keratometer for assessing astigmatism, helps to minimise post-operative astigmatism by controlling suture tension intraoperatively.
Advantages- Resuable, light weight
60. Maloney keratometer:
Identification- Cone-shaped instrument, designed to reflect the microscope light in concentric rings like pattern on cornea
Uses - To assess astigmatism intraoperatively.
Advantages- Minimize postoperative corneal astigmatism by controlling suture tension during keratoplasty

A. Bishop Harmon tissue forceps B. Serrefine C. Corneal fixation forceps D. Maloney keratometer E. PSU keratometer
Instruments used in Deep Anterior Lamellar Keratoplasty (DALK):
Trolley for Deep Anterior Lamellar Keratoplasty will have the following instruments:
|
Wire/Liebermann speculum |
For adequate exposure of palperbral aperture |
|
Castroviejo callipers |
To measure the host cornea to be excised |
|
Trephine |
For trephination of host cornea upto a depth of 90% of stroma |
|
Fogla pointed dissector |
To create a stromal pocket |
|
Fogla air injection cannula |
To inject air posteriorly to make a big bubble |
|
Fogla trifacet spatula |
To safely incise the stroma over the sharp facet of the spatula |
|
15o blade |
To create paracentesis and release aqueous |
|
OVD cannula |
To fill the AC with OVDs |
|
Fogla left and right scissors |
To excise the remaining stroma |
|
Cellulose spears |
To remove endothelium from the donor cornea |
|
Trephine |
For trephination of donor cornea |
|
Barraquer needle holder |
For suturing the lamellar graft to the host |
|
Colibri’s forceps/ Pollack forceps |
|
|
Kelman Mc Pherson forceps |
|
|
Jaffe suture tying forceps |
|
|
Portable keratometer |
To assess suture induced astigmatism peri-operatively |
|
Simcoe’s irrigation-aspiration cannula |
To wash the OVDs from AC |
|
Rycroft air injection cannula/ Hydro cannula |
To form the AC with BSS or air |
61. Paufique sclerotomy knife:
Identification – Flat handle with a cleaver type angled blade of size 6mm*3mm and a tip of 1.75mm
Uses - Used to make incisions and stromal pockets during keratoplasty. The knife features a sharp, rounded blade and is used to dissect the deep stromal tissue of the cornea parallel to Descemet's membrane. After this incision, the anterior lamellar kertoplasty may proceed.
Advantages – Angled sharp tip helps in precise corneal cleavage
62. Fogla pointed dissector:
Identification - Has sharp tip and rounded shaft Round bodied 27G with pointed taper tip
Uses - For creation of lamellar pocket in DALK for allowing introduction of 27G air injection cannula for creation of the “big bubble” (plane separation between Descemet’s membrane and corneal stroma).
Advantages - The sharp tip and rounded shaft give a more controlled creation of the lamellar pocket in DALK surgery
63. Fogla air injection cannula:
Identification – 25G or 27G cannula with flattened contour, closed rounded tip, and a bottom port at the tip. This cannula is attached to a 5cc air-filled syringe
Uses - Used while injecting air into deep corneal stroma in DALK surgery. The bottom port directs air posteriorly in order to achieve the “big bubble”. Air injection is continued in a controlled manner till the bubble outline reaches the edge of trephination
Advantages
- The blunt tip helps avoid deeper perforation into the anterior chamber
- The flattened cannula is easily inserted into the corneal stromal pocket.
Disadvantages –Sometimes if the placement of the cannula is a superficial significant amount of stromal emphysema may occur which makes it difficult to visualize the formation of a big bubble
64. Fogla trifacet spatula:
Identification – Long, slender, cross-serrated handle with an angled shaft with trifacet design and a blunt tip.
Uses - Introduced into space between Descemets membrane and corneal stroma after the formation of the “big bubble”, the anterior stroma is safely incised over sharp edge of spatula in order to enlarge the opening without damaging the Descemet’s membrane.
Advantages – Protects the underlying DM while incising the stroma
65. Fogla intrastromal pocket dissector:
Identification – Spring action, with reverse action jaws and rounded tips
Uses - To create a stromal pocket during the manual DALK procedure, the reverse action jaws spread when squeezed, applying counter traction that allows the edge geometry to separate stromal fibers efficiently.
Advantages - Rounded tips are designed for gentle insertion into the peripheral corneal stroma
66. Fogla scissors (left and right):
Identification – Small scissors come in pair of left and right. Spring action, serrated handles, and small blades. The lower blade of the scissors is thinner and 1mm longer than the upper blade which displaces Descemet’s membrane, protecting it from being damaged by the blades.
Uses - Used to divide stromal tissue into 4 quadrants and remove the residual corneal stroma separated from the Descemet’s membrane
Advantages – Thin blades remove stromal tissue without any damage to DM
67. Dastoor corneal graft holding forceps:
Identification – Small, stout forceps with serrated cross action handles with a screw-type lock. At the tip is a fenestrated convex inferior plate topped with a ring with four fixation prongs. It can be confused with a chalazion clamp.
Uses – Used to hold the graft for Lamellar Keratoplasty.
Advantages – Cross action lockable handle and four prongs at the tip holds the graft firmly and prevents slippage.
A. Paufique sclerotomy knife B. Fogla pointed dissector C. Fogla air injection cannula D. Fogla intrastromal pocket dissector E. Fogla trifacet spatula F. Fogla scissors G. Dastoor corneal graft holding forceps
Instruments used in Descemet Stripping Endothelial Keratoplasty (DSEK):
Trolley for Descemet Stripping Endothelial Keratoplasty will have the following instruments:
|
Wire speculum |
For adequate exposure of palpebral aperture |
|
15o Blade |
For paracentesis to enter the AC |
|
Visco cannula |
To form theca with OVDs |
|
Crescent blade |
To make a 5mm temporal sclera-corneal tunnel |
|
DSEK marker and skin marker pen |
To mark a ring of planned donor size as a guide for descemetorhexis |
|
Lewicky AC maintainer |
To keep the AC at optimum pressure for Descemetorhexis |
|
Reverse Sinsky hook |
To score and strip the host DM as marked previously |
|
Keratome |
To enter the anterior chamber through the corneo-scleral tunnel |
|
Kelmann-McPherson forceps |
To remove the detached DM from the AC |
|
DSEK stromal scrubber |
To roughen up the peripheral stromal bed to enhance adhesion |
|
Artificial anterior chamber |
To mount the donor tissue for manual lamellar dissection |
|
Corneal dissectors |
For manual lamellar dissection leaving about endothelium, DM, and a thin layer of stroma |
|
Trephine |
For trephination of the donor lenticle |
|
Simcoe I and A cannula |
To wash the OVDs from AC |
|
Busin glide |
For donor lenticle insertion by a pull-through method |
|
Rossenwasser forceps |
For donor lenticle insertion by taco push-in method |
|
Hydro cannula |
To float and unfold the lenticle in AC |
|
Air cannula |
To pressurize the AC to enhance lenticle adhesion |
|
Suture set |
To close the corneoscleral tunnel and paracentesis to prevent expulsion of the lenticle |
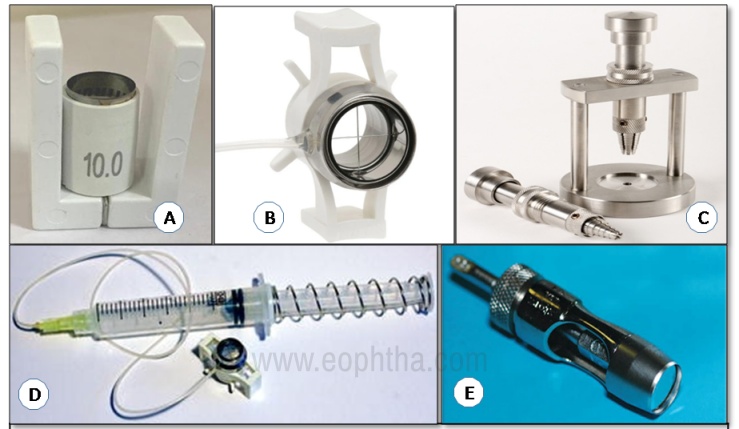
68. Fogla new artificial anterior chamber:
Identification - Comprised of three pieces (titanium made) - Base with tissue pedestal, tissue retainer, and locking ring. The base has one port with silicon tubing, an in-line pinch clamp, and a leur-lok hub
Uses – For lamellar dissection during lamellar keratoplasty
Advantages - Maintains adequate pressure during lamellar dissection of the cornea
69. Barron Artificial anterior chamber:
Identification – The base has two ports with silicon tubing, pinch clamps, and Luer-Lok connectors. It has a pedestal to mount the tissue epithelial side up, a tissue retainer, and a locking ring. Ports can be used to inject or aspirate saline, visco-elastics, or air. The design of the chamber allows the surgeon to firmly hold the donor button epithelial side up on a bed of OVD, pressurize it and perform lamellar dissection
Uses – Manual lamellar dissection
Advantages-
- Mounts donor tissue epithelial side up, and hence preserves and protects the endothelium.
- Maintains adequate pressure while lamellar dissection is carried on
- Bright blue colour provides a high contrast background for lamellar dissection
70. Corneal dissectors:
Identification – Available in a set of 2 to 3. Also known as DALK spatula.
Triangular spatula to dissect downward into the cornea until the desired stromal depth is reached
8mm curved spatula with a rounded tip to dissect up to two-third across the cornea
12mm curved spatula to dissect complete 360 degrees across the cornea
Uses - Manual deep stroma dissection
Advantages– Sharpened edges to create smooth interface hence the risk of interface haze is reduced
71. Busin glide:
Identification–Long rounded handle with a sliding guide at the end. Can be with or without lateral loading winglets. Donor lamella is loaded endothelial side up into the glide
Uses–As a sliding guide for the donor lenticle insertion in DSEK/ DSAEK through 4 mm incision.
Advantages–
- Facilitates the unfolding of the graft and centration of the donor button in the anterior chamber
- Helps to minimize the manipulation of the graft and thus endothelial loss
72. Lewicky AC maintainer:
Identification - Threaded tip of 20 G /23G, the overall length of tip 12mm, with 200mm long silicone tubing, and an adaptor at another end
Uses – Provide control over the depth of anterior chamber during eye surgical procedure where AC depth control is important eg: IOL exchange, hyphema evacuation, Blumenthal method of cataract surgery
Advantages - 23G shaft is easy to insert, self-retaining threaded tip assures stable fixation within the corneal stroma
73. Rosenwasser forceps:
Identification - Thin vaulted 12mm long shanks and a precalibrated heel stop
Uses - Donor lamella insertion in DSEK
Advantages - Precalibrated heel stop to prevent tips from closing
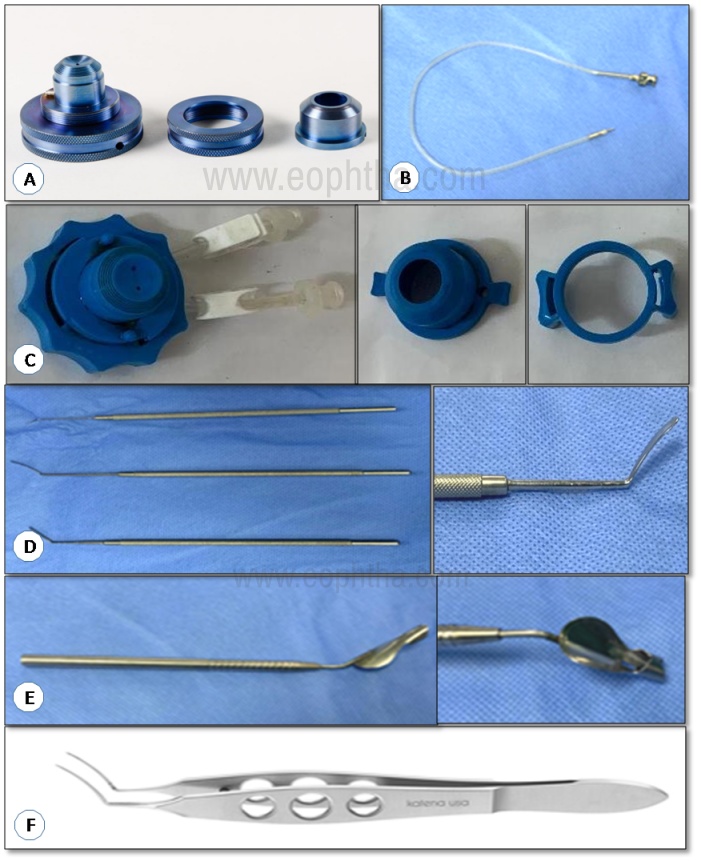
A. Fogla new artificial anterior chamber B. Lewicky AC maintainer C. Barron artificial anterior chamber D. Corneal dissectors E. Busin glide F. Rossenwasser forceps
74. Fogla endothelial grasping forceps:
Identification – Rounded tip bent upward at a 900 angle with reverse action cross serrated handle
Uses - To remove unhealthy DM during DSEK, DSAEK, and DMEK surgery
Advantages - Tip is designed to prevent damage to corneal stromal fibers when pressed against the cornea to break DM
75. DSEK stromal scrubber:
Identification - 8mm tip diameter, curvilinear bent in tip with a strongly vaulted shaft, round handle, and overall length 114mm
Uses - Roughens the inner corneal stroma within the area of descemrtorhexis circle
Advantages - Facilitate disc adhesion to recipient cornea hence reduce the possibility of donor tissue detachment, the curvilinear design allows easy access of inner-corneal dome
76. DSEK donor lamella shovel:
Identification – Cross serrated round handle with angled shaft and flat platform over the tip
Uses - For insertion of donor lamella, it helps to prevent the folded donor Lamella from sliding off during insertion
Advantages - It prevents the folded donor lamella from sliding off during insertion
77. Reverse Sinsky's hook:
Identification– Long slender instrument with 0.22mm diameter blunt tip, 0.7mm height pointing upward, 450 angled shaft with 10mm length, overall length 118mm.
Uses- For scoring of Descemet’s Membrane the beginning of descemetorhhexis.
Advantages- Gently strip the membrane
78. Steinert Descemet stripper:
Identification–A long slender instrument with diamond serrations on the handle, an angled shaft, and a sandblasted ball tip.
Uses- Allow uniform detachment of host DM without damage to the corneal stroma
Advantages-
- Unique design allows for excellent apposition to the inner-dome curvature of recipient cornea
- Curvilinear design is effective in reaching DM over all inner curvature of recipient cornea
- Round handle permits rotational movement along the long axis of the instrument.
79. DSEK double marker:
Identification – Unique double-sided instrument with 8 mm ring on one side and 9mm ring diameter on the other, flat handle, and serrated grip. Made of titanium or stainless steel.
Uses –
The most commonly used diameter for Descemetorrhexis is 8.0 or 9.0 mm. This instrument has both the commonly used diameters in one marker. This provides a circular mark on the recipient corneal epithelium which helps as a guiding mark while performing Descemetorrhexis.
Advantage – A single instrument has 2 most commonly used diameter markers.
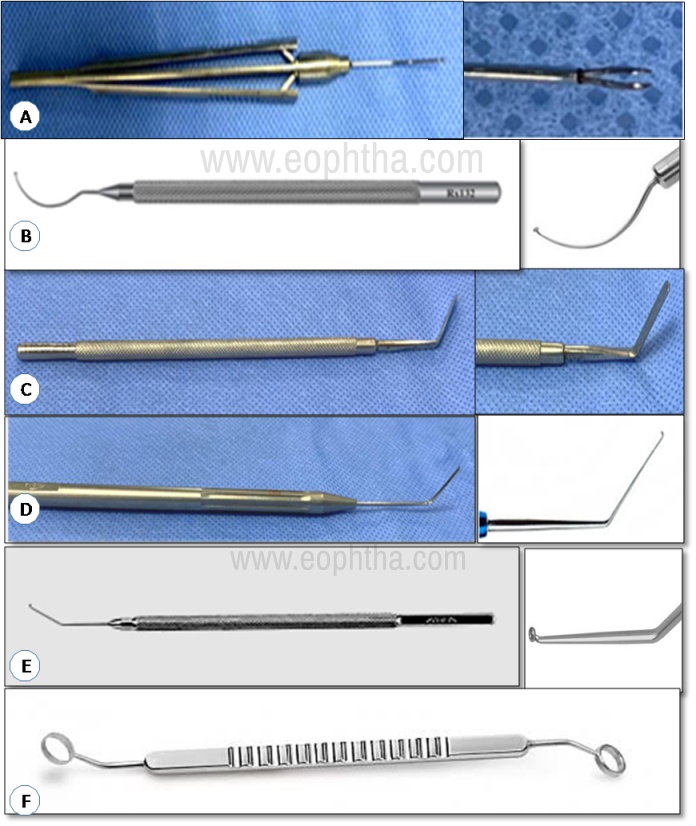
A. Fogla endothelial grasping forceps B. DSEK stromal scrubber C. DSEK donor lamella shovel D. Reverse sinskey’s hook E. Steinert descemet stripper F. DSEK double marker
Instruments used in Descemet Membrane Endothelial Keratoplasty (DMEK):
Trolley for Descemet Membrane Endothelial Keratoplasty will have the following instruments:
|
Wire speculum |
For adequate exposure of palpebral aperture |
|
15o blade |
To create 2-4 paracentesis |
|
Visco cannula |
To form the AC with OVDs |
|
Marker and skin marking pen |
To mark recipient epithelium as a guide for descemetorhexis |
|
Reverse Sinskey hook/ scorer/ Dexatome spatula |
To score and peel the recipient DM along the mark made previously |
|
Keratome |
To make a temporal corneal incision |
|
Kelmann McPherson forceps |
To pull the peeled DM from the AC |
|
Simcoe I and A cannula |
To remove the OVDs from AC |
|
Hydrocannula |
To inject pilocarpine and BSS |
|
Twin Teflon block |
To place the donor tissue for dissection |
|
Trypan blue |
To stain the donor endothelium |
|
Scorer |
To create a liftable edge in the DM |
|
Fogla stripping peeling forceps |
To grasp and peel the DM from the donor tissue |
|
Trephine |
To punch the donor to the required size |
|
Fogla F marker |
To mark the DM/stromal side |
|
DMEK injector/ modified Jones tube |
To aspirate and insert the lenticle through the corneal incision |
|
Hydrocannula/ Air cannula |
To perform the air-fluid exchange and pressurize the chamber with air |
|
Suture set |
To suture the corneal incision and paracenteses |
80. DMEK scorer:
Identification – Rounded, fenestrated handle, with angled shaft and sharp tip. The tip is bent upwards at a 90o angle.
Uses –
- To score the DM prior to stripping it off
- To remove unhealthy DM during DSAEK, DSEK, and DMEK
Advantages –
- Angled shaft and bent tip helps to reach under the corneal dome
- The tip is designed to prevent damage to the stroma when pressed against the cornea to break DM
81. Fogla stripping peeling forceps:
Identification -Forceps with serrated handles and elongated tips perpendicular to the shaft, anatomically designed for the stripping/peeling of the delicate Descemet membrane.
Uses- The forceps grasp the membrane at the edge and perform the detachment of Descemet lenticle by means of peeling action
Advantages – Tips are designed for grasping and peeling the DM with minimal injury
82. Fogla cleavage hook:
Identification – Rounded, fenestrated handle with triangular-shaped, atraumatic tip.
Uses –
- Delicate blunt hook for DM cleavage.
- Used to perform cleavage at the edges of the lenticle previously secured to the suction DMEK support.
Once the correct thickness of DM is achieved, DM is peeled off.
Advantages – Fine blunt hook protects the delicate DM from injury
83. Fogla F marker:
Identification - F shaped marker with 2mm tip on a long, rounded, fenestrated handle with a 35 angled shaft
Uses – To mark stromal side of donor lenticle in DMEK
Advantages – Helps in identifying stromal side of the lenticle and hence prevents insertion of reverse graft.
Other variants available for marking orientation of graft are:
S-marker- 1.25*2.5mm sized S shape on the tip
P-marker – 2mm tip with a P shape
84. DMEK crystal spatula:
Identification -This spatula has a smooth, rounded, olive tip which is specially designed for use on the donor Descemet's membrane within the recipient anterior chamber to facilitate unrolling of the donor DM. It has a long, slender, rounded, and fenestrated handle
Uses- It is used to unravel the Descemet’s membrane in the anterior chamber and help with the proper orientation of the Descemet’s membrane prior to air-attachment to the patient’s cornea
Advantages –
- Smooth (atraumatic)olive tip to handle DM
- When a no-touch technique is not successful these spatulas help complete the procedure
85. DMEK rake:
Identification – Round, fenestrated handle with a blunt T-shaped tip
Uses - Careful separation of donor DM without direct contact with endothelial surface
Advantages - Wider, flat surface allows for gentle manipulation of donor tissue while harvesting the endothelial graft
86. Twin teflon block:
Identification–Rectangular teflon block with two wells having a central hole each
Uses– Specially designed to hold donor cornea and help surgeon in donor preparation. Helps in separation, staining, and temporary placement of the donor DM and endothelial cells until transplanted to the recipient cornea
Advantages–
- Central hole helps in accurate positioning
- Aspheric curvature to match corneal curvature
- Twin wells help during donor tissue manipulation
87. Dexatome spatula:
Identification - Strongly vaulted shaft, 17mm long from bend to tip, with a rounded handle
Uses –
- Smooth uniform Descemetorhexis and removal of the Descemet’s membrane as a single disc
- Used to mark the cornea at 10mm
Advantages-
- The unique multi-curve design facilitates complete scoring of Descemet's membrane 360° without exiting the anterior chamber
- The single instrument allows for both Descemetorhexis and Descemet's membrane detachment and subsequent removal
88. DMEK injector:
Identification – Fine oval tip with rounded larger opening of the cartridge. It is attached to a disposable syringe along with a piece of silicon tubing.
Uses – Used for contactless intake of the graft into the cartridge and gentle injection into the anterior chamber
Advantages -
- Safe and easy intake of graft due to rounded opening
- Minimum incision size due to fine oval opening tip
A. Fogla stripping peeling forceps B. Fogla cleavage hook C. Fogla F marker D. DMEK rake E. Twin Teflon block F. Dexatome spatula and tip G. DMEK scorer H. DMEK injector tip I. Crystal spatula and tip
Instruments used in eye bank (enucleation):
Lancaster eye speculum (already described)
Steven tenotomy scissors (already described)
89. Elshnig fixation forceps:
Identification- Straight shaft with 2mm, 1x2 Elschnig style teeth, and a narrow serrated handle
Uses- Fixation of globe during intraocular procedures
Advantages –
- Atraumatic
- Firm grip

90. Graefe muscle hook:
Identification- Straight shaft with a flattened tip, 10.5mm hook and a flat handle
Uses- To hook and isolate extraocular muscles
Advantages – Atraumatic tip to minimise muscle injury

91. Enucleation scissors (Metzenbaum or Storz):
Identification – Long, heavy and curved blades with blunt, rounded tips and ring handle
Uses–
- Cutting of optic nerve during enucleation
- Lateral canthotomy
Advantages –
- The length provides good access to optic nerve near orbital apex
- Blunt tips avoid injury to vital orbital structures
- Broad blades provide adequate force to cut optic nerve.
- The ring handle helps in firm hold and application of force

92. Halsted mosquito artery forceps:
Identification – Straight or curved shaft, with slender serrated jaws and a ratchet lock for clamping small vessels
Uses –
- Hemostasis- for grasping and compressing an artery to control bleeding
- To clamp small tissue E.g. recti muscle before cutting
Advantages –
- Ratchet lock ensures adequate clamping of the blood vessels
- Slender jaws can grasp small delicate arteries and tissue

93. Wells enucleation spoon:
Identification- Spoon like, shallow ,concave, hemispherical end attached to long shaft. Has a guide or groove for engagement of optic nerve
Size available from 15 to 21mm diameter
Uses –
- Enucleation while harvesting eyeball
- Perform therapeutic enucleation in painful eye
- Advanced malignant intraocular tumors
Advantages – Concavity follows the natural eye contour and allows the globe to rest over the spoon
