
Pioneered and popularized by Howard Gimbel, capsulorrhexis is probably the most challenging task to learn in cataract surgery. In other words once a good rhexis is done half the battle is won. All the post-graduates and beginners struggle to do a ideal rhexis. This small write-up shares small tips and tricks to do rhexis better.
Ideally rhexis should be continuous and curvilinear i.e Circular, Central & of Correct size (5.5-6 mm).
- Circular: for proper IOL centering and stabilization in the bag
- Continous: to prevent rhexis extension
- Correct size: for IOL centering and to ensure anterior capsule overlapping IOL optic 360 degrees.
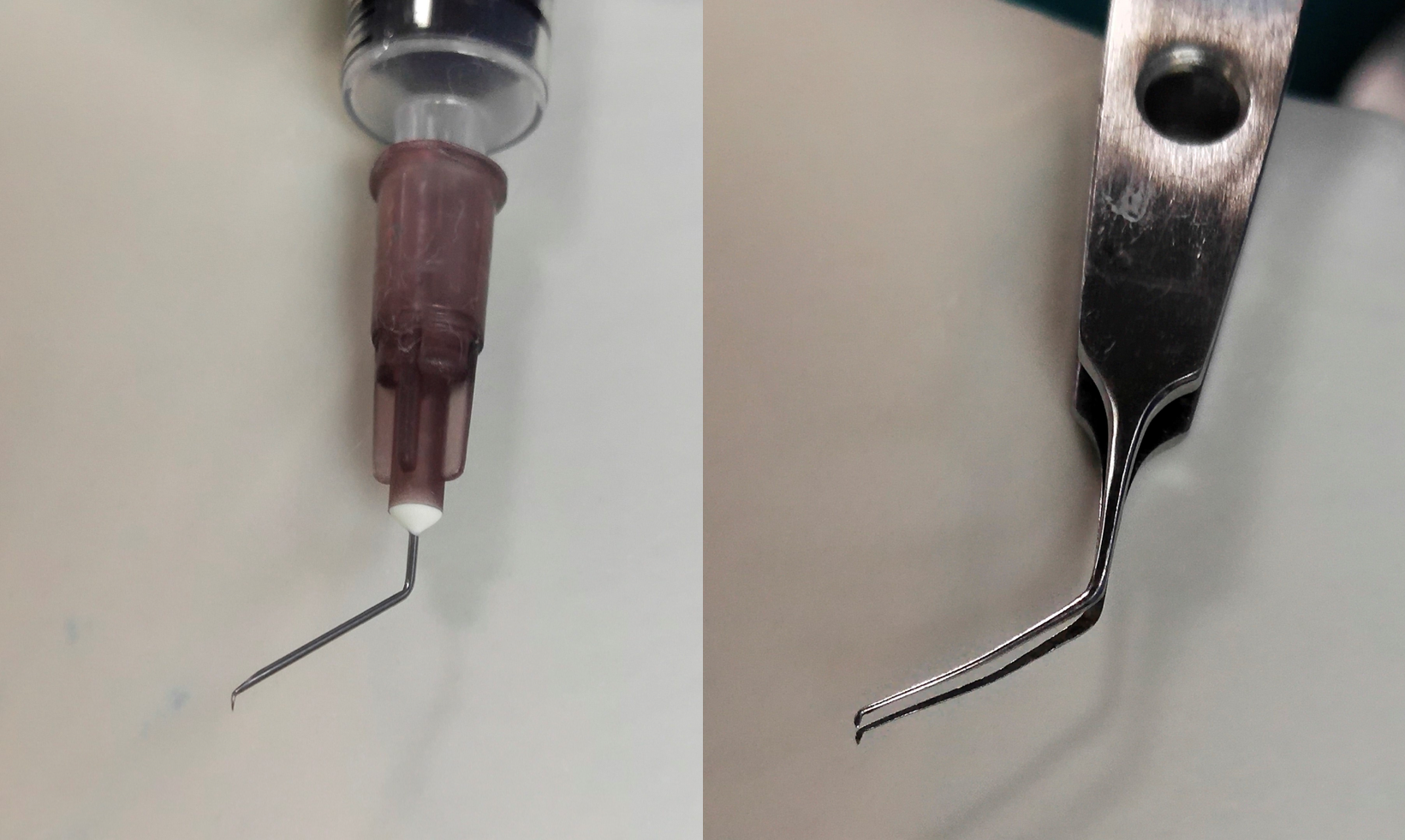
It can be done with the help of double bent 26 G/27 G needle or rhexis forceps.
Advantages of rhexis with 26 G/27 G needle(Cystitome):
- Cheap
- Disposable
- Universally available
- Customized
- Small diameter, light weight
- Can be done through side port so less chance of AC shallowing
Cons of rhexis with 26 G/27 G needle (Cystitome):
- Less precise control
- With needle it is difficult to bring rhexis margin back in case of extension
- Risk of inadvertent capsule nick/tear
- Sharp end of needle can cause wound damage during insertion or removal.
Advantages of rhexis with Utrata Forceps
- Precise control
Disadvantages of rhexis with Utrata Forceps
- Bulky vs needle
- Sudden movements can cause rhexis damage
- Needs bigger entry port, needs to be done through main port so risk of repeated AC shallowing
Prerequisites of doing rhexis
- Clear media: Clear cornea, well dilated pupil
- Put visco over the cornea for better visibility .
- Should be done at higher magnification.
- Fill the chamber with viscoelastics.
- Try moving the eye around to get best possible red reflex.
- Globe should be well stabilized while doing the procedure.
Tips to achieve ideal capsulorhexis:
TIP NO.1 PRACTICE PRACTICE PRACTICE…..
- Surgeon should have stable hands and practice fine intraocular micro-movements. Stereoscopic viewing with proper depth perception is essential.
- Theoretical concepts about physics behind tearing and shearing forces , which are in play during rhexis process, should be read and well understood
- You can practice rhexis on the plastic film of lens box or use poached tomatoes or potatoes.

TIP NO. 2KEEP ANTERIOR CHAMBER DEEP
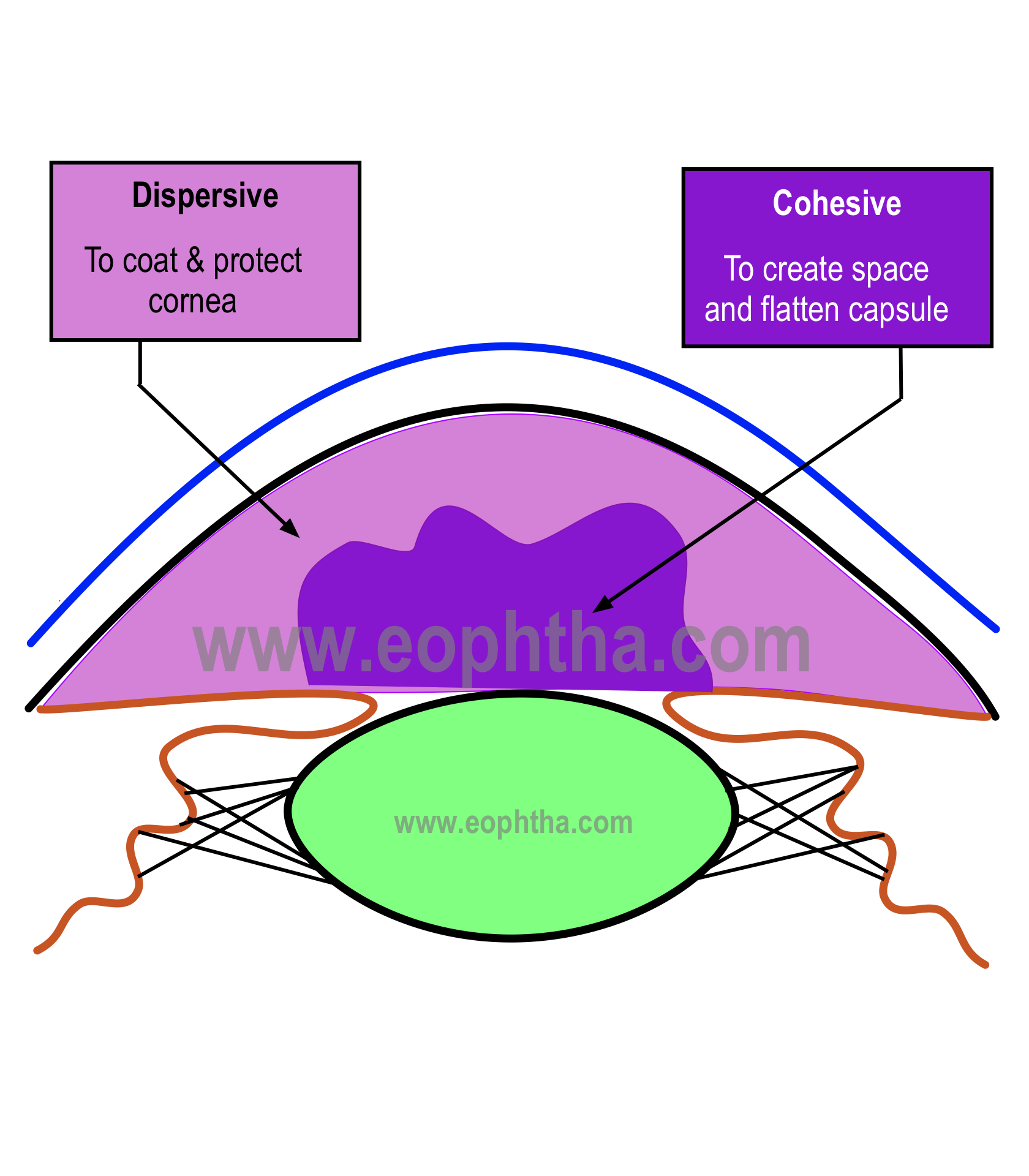
- Use soft shell technique to deepen the AC and make the anterior capsule flat.
- Use sideport for all you maneuvers, it prevents visco leakage.
- Avoid undue pressure on eye ball
- Keep refilling visco as and when required
TIP NO. 3DON’T LIMIT YOURSELF TO ONE TECHNIQUE
- One should be well versed with cystitome and utrata forceps.
- You might have to use either one or combination of both depending on the situation
TIP NO. 4PROPER VISUALIZATION
- Use trypan blue dye to stain anterior capsule and improve visualization.
- Increasing the magnification, “you see well-you do well”. Higher magnification also improves the visualization and can help you in early identification of extension.
- Retro-illumination is one of the greatest tools available to us in the microscope. It makes use of coaxial illumination to increase the Red Glow.
- Proper patient positioning is also a measure to improve red reflex, when the iris lens diaphragm is parallel to the ground the red improve as the microscope becomes coaxial and one has good red glow
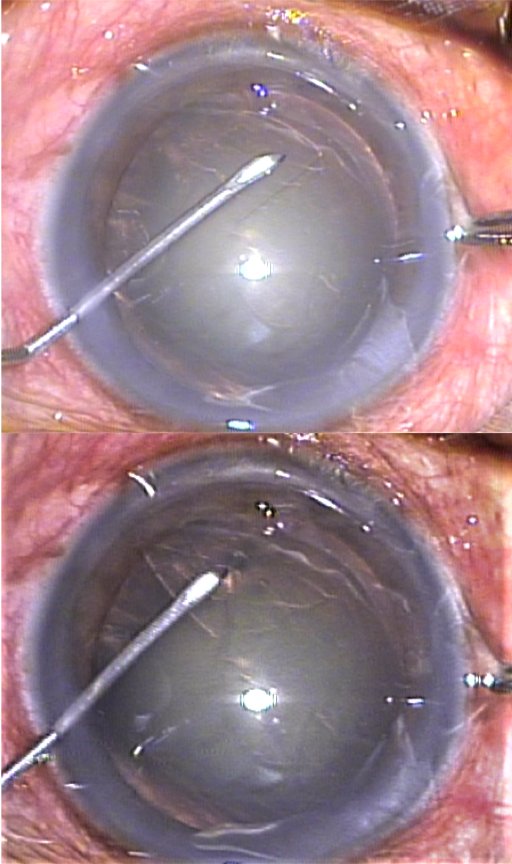
TIP NO. 5ALWAYS KEEP THE FLAP FLAT OVER THE ANTERIOR CAPSULE.
- When the flap is crumpled, the cut /leading edge of rhexis is not visible, increasing the risk of irregular rhexis or extension.
- By keeping the flap well spread and flat over the anterior capsule you would improve you control and it is very easy to achieve the desired size and shape.
Secret to a Perfect Rhexis
- Good visualization
- Proper staining
- Higher magnification & good focusing of the capsule
- Deep AC
- Flat capsular flap on the anterior capsule