

Nystagmus is defined as an involuntary rhythmic oscillation of one or both the eyes. Clinical assessment and eye movement recordings are important to diagnose and classify nystagmus. It is essential to have patience while examining a child, as anxiety often increases nystagmus.
1.Classification
Physiological eye movements have to be differentiated from pathological eye movements. The older etiology-based classification of nystagmus is redesigned into characteristics-based new classification by CEMAS (Classification of Eye Movement and Strabismus). Infantile nystagmus syndrome (INS) is characterized by horizontal conjugate nystagmus, infantile-onset, accelerating slow phase, increase with fixation attempt, convergence dampening, and presence of null zone with decreased amplitude. Fusion maldevelopment nystagmus syndrome (FMNS) is characterized by decelerating slow phase, associated strabismus, a latent component with fast phase towards fixing eye and decrease in intensity with adduction and binocular fusion. Spasmus nutans syndrome consists of head nodding, abnormal head position and low amplitude high-frequency oscillations with/without normal neuroimaging.
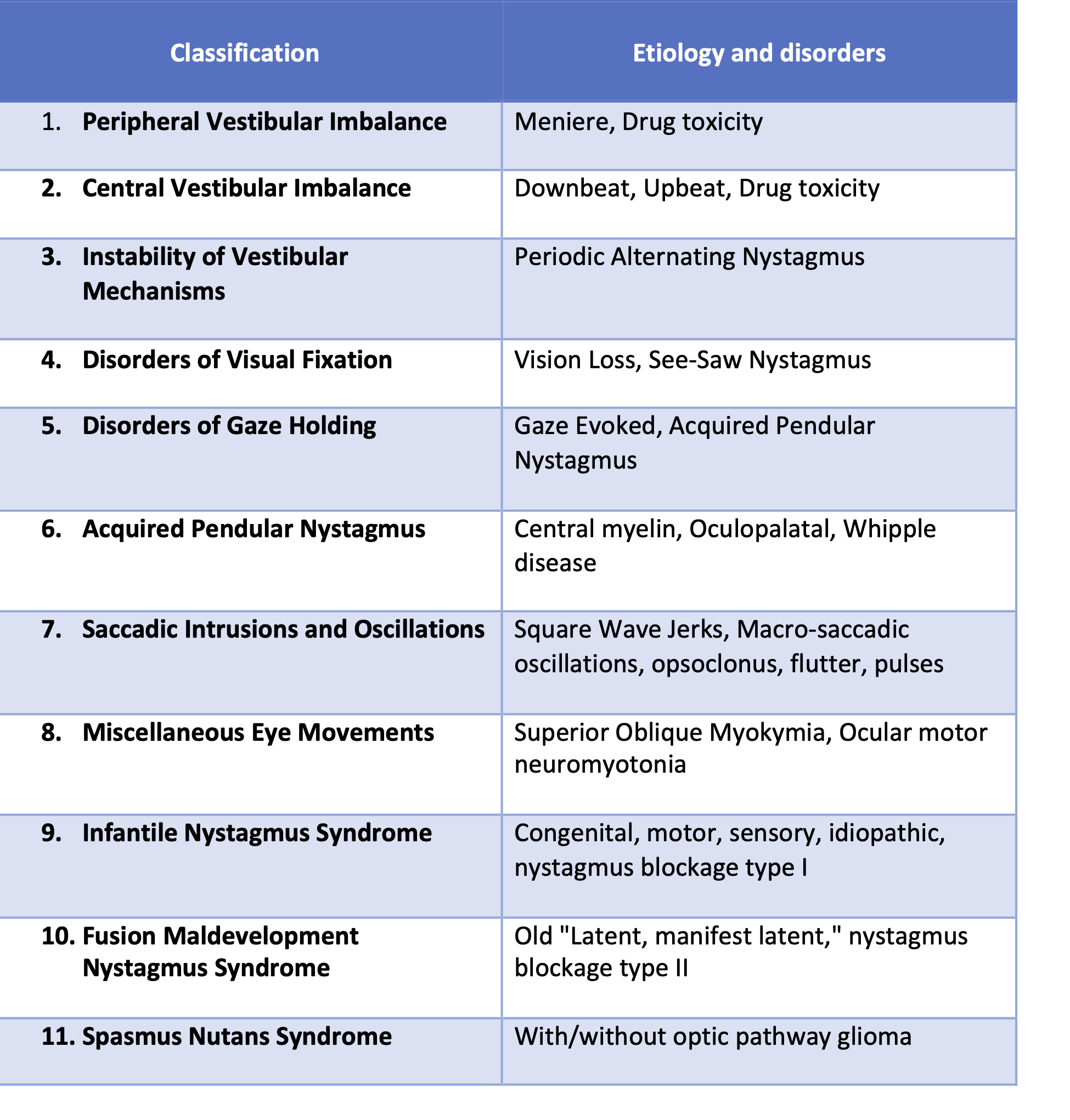
Table 1 Classification of nystagmus according to CEMAS.
2. The mechanism for stable eye movements
Three mechanisms help in preventing the deviation of line of sight from the object of regard. First is ‘visual fixation’ in which the visual system can detect retinal image drift and program corrective eye movements to suppress the unwanted saccadic movement. Secondly, ‘Vestibulo-ocular reflex’ compensates for head rotations and the third is ‘gaze holding system’. This consists of a“neural integrator system” that changes the resting firing rate to the extraocular muscle to overcome the viscoelastic forces of orbit and maintain a position of eccentric gaze.
3. Acquired nystagmus
Disorders of an afferent visual pathway or the visual-motor calibration system result in nystagmus such as acquired pendular nystagmus of the blind eye and seesaw nystagmus in parasellar lesions. Disorders of the vestibular system could arise in the periphery, which consists of mixed horizontal-torsional nystagmus and can be attenuated with visual fixation. Central vestibular nystagmus is usually vertical and does not attenuate by visual fixation. Acquired periodic alternating nystagmus is due to disinhibition of central velocity related functions mediated by the cerebellum. Neural integrator consists of nucleus prepositus glossi-medial vestibular nucleus for horizontal eye movements, interstitial nucleus of Cajal for vertical gaze and flocculus of the cerebellum. Disorders of these structures impair the ability to hold eccentric gaze and results in gaze-evoked nystagmus. Oscillopsia is experienced by patients of acquired nystagmus and is usually absent in congenital nystagmus, except in cases of decompensated strabismus and progressive retinopathy.
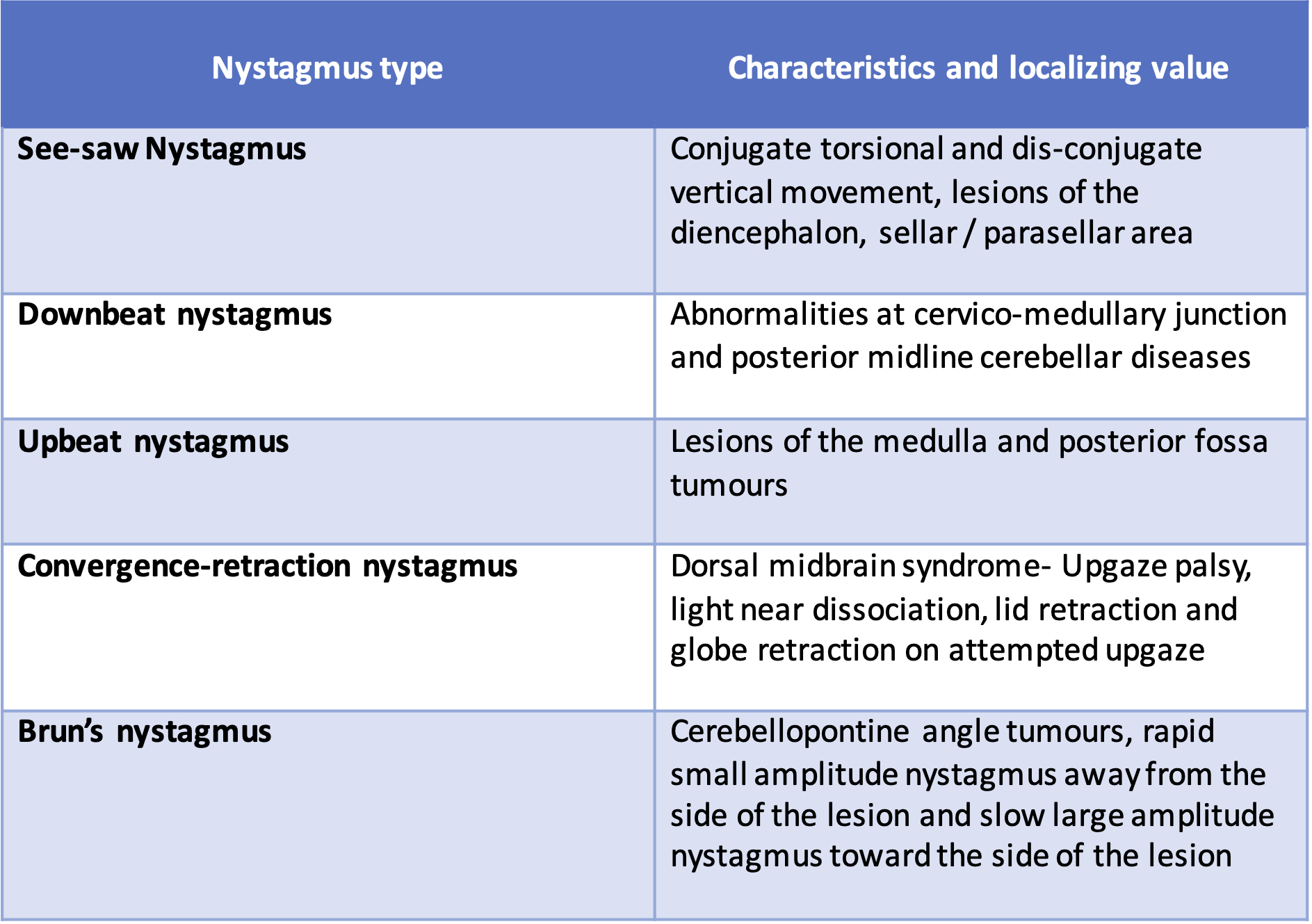
Table 2 Localizing value of certain types of nystagmus.
4. Nystagmus evaluation
An extensive history, including onset, familial history, birth history and developmental milestones is to be elucidated. Look for abnormal functional components of vision such as photophobia, nyctalopia and delayed visual development. The following have to be kept in mind while seeing a patient of nystagmus. These evaluation points become more important when motility recordings are not available and the onus of diagnosing nystagmus is on clinical examination only.
- Direction- Note the direction of the fast phase in jerky nystagmus, it can be horizontal as well as vertical. Always observe the patient for 3-5 minutes to detect periodic alternating nystagmus in which the direction of nystagmus changes in the opposite direction.
- Plane – Nystagmus can be purely horizontal, vertical, torsional or a combination of either of these.
- Intensity- Document amplitude and frequency, along with the alteration of nystagmus in different gazes.
- Normal eye movements – Observe the changes in normal eye movements such as pursuits, saccades and vestibulo-ocular reflex
- Conjugacy- Nystagmus can be conjugate as in INS or disconjugate as in seesaw nystagmus and internuclear ophthalmoplegia.
- Associations- Look for any associated strabismus and presence of abnormal head posture.
- Cover- Check if the direction of nystagmus changes towards the fixing eye on monocular covering of the eye. In cases of FMNS, patients keep their fixing eye in extreme adduction which is though known as adduction null, but is not a true null point. They utilize the Alexander’s law to their advantage, which state that the jerk nystagmus usually increases in amplitude upon gaze in the direction of the fast component.
- Convergence- Document the effect of convergence on the nystagmus. This can be tested by introducing 7 Dioptre base-out prisms and documenting the change in visual acuity and nystagmus intensity.
5. Extensive Workup
Binocular visual acuity (person’s acuity) is usually more than monocular visual acuity (eye’s acuity) and hence vision should be assessed by fogging the other eye.
- Pupil evaluation to detect afferent pupillary defects, anisocoria, and paradoxical responses
- Anterior and posterior segment - The examiner should watch for high refractive errors, iris transillumination defects, foveal hypoplasia, pigmentary retinopathy, and optic nerve dysplasia.
- Visual field testing on Standard automated perimetry or Goldmann visual fields can be performed for better assessment of the patient’s visual function where possible.
- Visual Evoked Potential (VEP) – It measures the global visual function from the retina to the visual cortex. This is particularly useful for assessment of the central visual field and misrouting of optic nerves in young boys and girls.
- Optical Coherence Tomography (OCT)- Difficult to obtain in a small child but in older children can help in diagnosing foveal hypoplasia and macular changes in other retinal dystrophies.
- Electroretinogram (ERG) should be done in cases of suspected retinal dysfunction such as Leber congenital amaurosis or rod monochromatism.
- Eye movement recording is essential in all cases to classify the type of nystagmus.
- Neuroimaging- MRI is important in cases of oscillopsia, asymmetric, disconjugate, and vertical nystagmus to rule out structural anomalies or tumors of anterior visual pathways.
- Other specialty- Appropriate genetic workup with pedigree analysis should be done. In cases of a structural anomaly, a full assessment by a pediatric neurologist and endocrinologist should be sorted. Conjunctival biopsy and urine/serum may be sampled to screen for diseases of abnormal metabolism.
- NAFX - As it is important for motility waveform to be recorded to accurately diagnose nystagmus. Similarly, it is important to document the visual function, as the improvement in visual acuity only does not necessarily indicate the improvement in nystagmus. Additionally, in INS, amplitude, frequency, and intensity, are not good indicators of visual function and should not be used as outcome measures for therapeutic intervention. The waveform characteristics related to overall visual function are foveation time, beat-to-beat foveation position and velocity variation. The eXpanded Nystagmus Acuity Function (NAFX), developed using sophisticated computer programs, evaluates the foveation quality of nystagmus waveforms and quantifies it between 0 and 1. This value is linearly correlated to best-corrected visual acuity in the absence of an afferent defect. However, it is still not widely available and at times not practical as well.
6. Non-surgical management
A single most important step in managing all nystagmus is performing cycloplegic refraction and prescribing appropriate spectacles. Bifocals should be added if hypo-accommodation is present. If convergence dampening is present in patients of INS without strabismus, add 7 diopter base-out prisms in front of each eye with over-minus glasses (-1 sphere). The use of contact lenses that provide exteroceptive feedback also reduces the intensity of nystagmus.
Botulinum toxin injection helps in reducing nystagmus and improve vision in some patients but it acts for a short period and is associated with ptosis. In cases of oscillopsia, retrobulbar injection of Botulinum toxin has been attempted with limited success. Clonazepam and Baclofen have a proven role in treating central vestibular (upbeat and downbeat) nystagmus. Periodic alternating nystagmus has shown improvement with Baclofen (5-10mg TDS). The most effective treatment of acquired pendular nystagmus (associated with disease of central myelin) is Gabapentin and Memantine.
The NAFX documentation could allow the physician to estimate the percentage improvement from intervention and make an informed decision about its therapeutic efficacy.
7. Surgery for Nystagmus
The purpose of extraocular muscle surgery in nystagmus is to center the preferred position of the eye and to improve the oscillation’s beat-to-beat characteristics. Cüppers proposed that in cases of observable convergence dampening with good binocular function, artificial divergence can be created surgically. A bilateralmedial rectus recession of 3mm is done to induce convergence. However, the proportion of INS patients in whom this two-muscle surgery is indicated are small. In the absence of a null zone, abnormal head posture, strabismus or convergence null, patients can benefit from tenotomy and reattachment of all four horizontal muscles. This involves enthesial tenotomy, dissection and reattachment at its original insertion. This procedure results in higher peak NAFX values probably through alteration of the proprioceptive tension-control loop.
8. Surgery for abnormal head posture
Abnormal head posture (AHP) can present as head Turn in cases of eccentric horizontal null position, Tip-up and tip-down (Chin up and down) or head Tilt in cases of torsional null(3T). In cases of a head turn of 15-20°, Anderson's yoke muscle recession can be done while in larger angles Kestenbaum-Anderson’s procedure involving recess-resect of all four horizontal muscles is done. In cases of chin-up posture depressors of the eye (superior oblique and inferior rectus) are weakened while elevators (inferior oblique and superior rectus) are weakened to correct chin down posture. Head tilt is corrected by surgically rotating the eye in the direction of the head tilt. This can be achieved by either operating on oblique muscles or horizontal transposition of vertical muscles or vertical transposition of horizontal muscles.

Figure 1 Face turn

Figure 2 Chin down &Chin up posture

Figure 3 Right and left head tilt
9.Strabismus with AHP
In these cases, straighten the head position by using prisms over the fixing eye, correct the residual strabismus by neutralizing the prisms over the non-fixing eye and perform the surgery accordingly. In cases of multiplanar AHP, it is better to correct the AHP in one plane and stage the surgery later for another plane.
10. Other surgical procedures
In cases of FMNS, it is beneficial to move the eye in abduction to correct esotropia as adduction innervation is required to maintain fixation that dampens the FMNS by taking advantage of Alexander’s law. Nystagmus blockage syndrome is benefited from bimedial recession procedure in type I and performing surgery to straighten the eyes in type II.
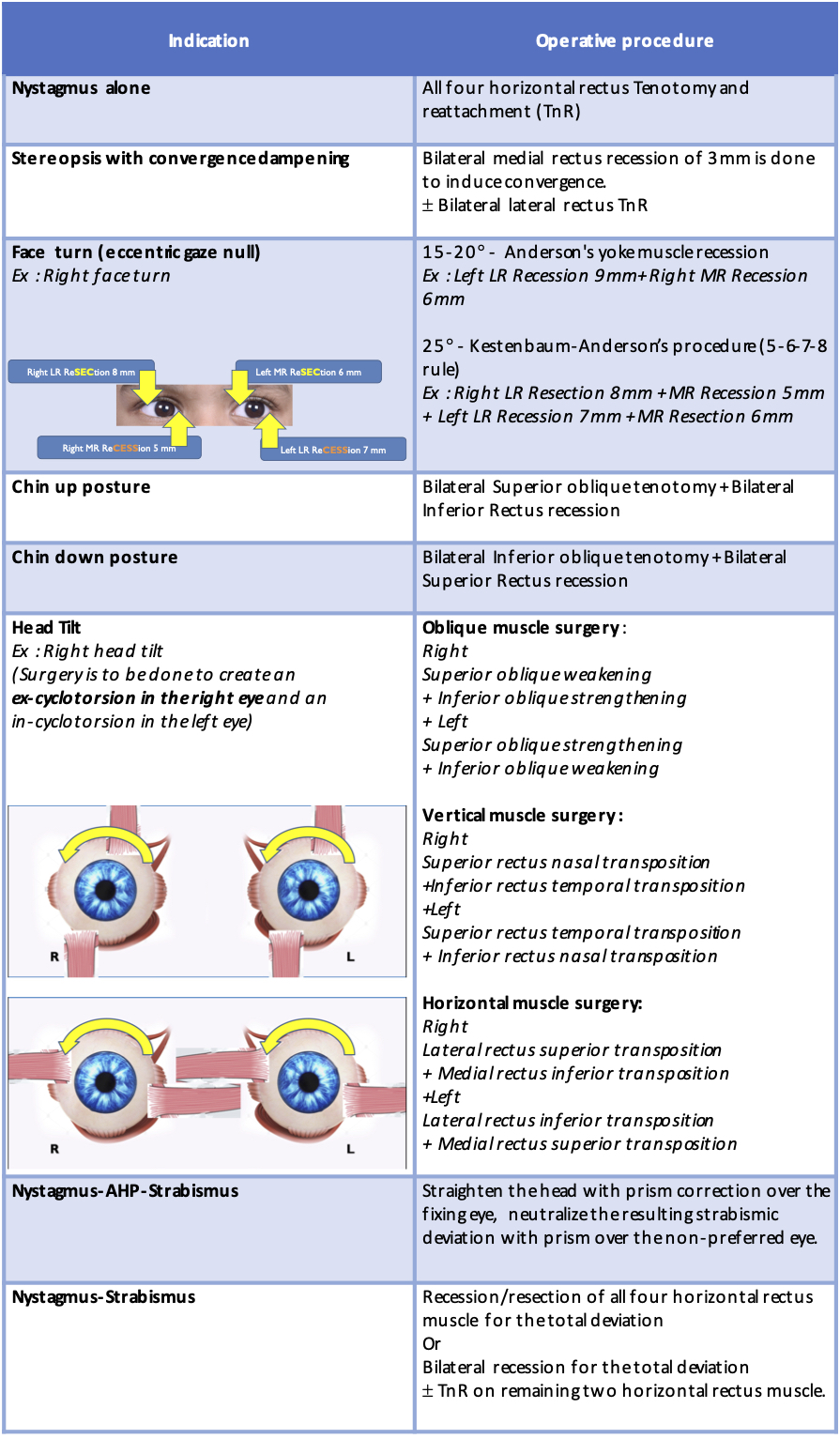
Table 3 Operations in nystagmus
References
- CEMAS Working Group. A National Eye Institute sponsored workshop and publication on the classification of eye movement abnormalities and strabismus (CEMAS). The National Eye Institute Publications. 2001:1-75.
- Stahl JS, Averbuch-Heller L, Leigh RJ. Acquired nystagmus. Arch Ophthalmol. 2000;118(4):544–9.
- Hertle RW. Nystagmus and Ocular Oscillations in Infancy and Childhood. In: Handbook of Pediatric Neuro-Ophthalmology 2006 (pp. 289-323). Springer, New York, NY.
- Noval S, González-Manrique M, Rodríguez-Del Valle JM, Rodríguez-Sánchez JM. Abnormal Head Position in Infantile Nystagmus Syndrome. ISRN Ophthalmol. 2011;2011(iii):1–7.
- Ehrhardt D, Eggenberger E. Medical treatment of acquired nystagmus. Curr Opin Ophthalmol. 2012 Nov;23(6):510–6.
- Hertle RW. Nystagmus in infancy and childhood. Semin Ophthalmol. 2008;23(5):307–17.
- Hertle, R. and Dell'Osso, L., 2013.Nystagmus In Infancy And Childhood. New York: Oxford University Press.
- Yang H, Yu T, Sun C, et al. Spectral-domain optical coherence tomography in patients with congenital nystagmus.Int J Ophthalmol. 2011;4(6):627‐630