
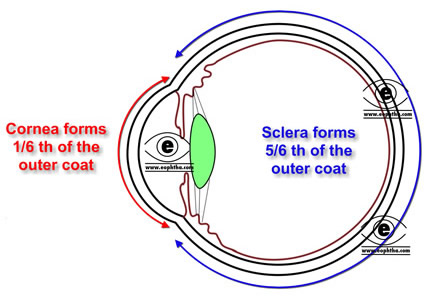
The term sclera is derived from Greek word scleros meaning "hard".Sclera is an opaque, elastic, and resilient tissue of the eye. It can be compared with an incomplete shell comprising approximately 90% (five-sixths) of the outer coat of the eye. Anteriorly it begins at the limbus and terminates at the optic nerve canal posteriorly. The primary function of the sclera is to protect the eye and maintain the shape of the eye ball.
Amazing Fact:
Human beings are the only primates with white sclera
Embryologically like corneal stroma and endothelium, sclera originates from mesoderm.
The human sclera is white in colour. This white appearance is because of the scattering of all wavelengths of light by dense irregular bundles of collagen in sclera. In children, a bluish hue is observed because of the extremely thin sclera which allows the visibility of underlying choroid. In older age the sclera may appear slightly yellowish because of the deposition of fat.
Thickness of sclera:Sclera is thicker in males than in females. Human sclera is thickest near the optic nerve, where it is approximately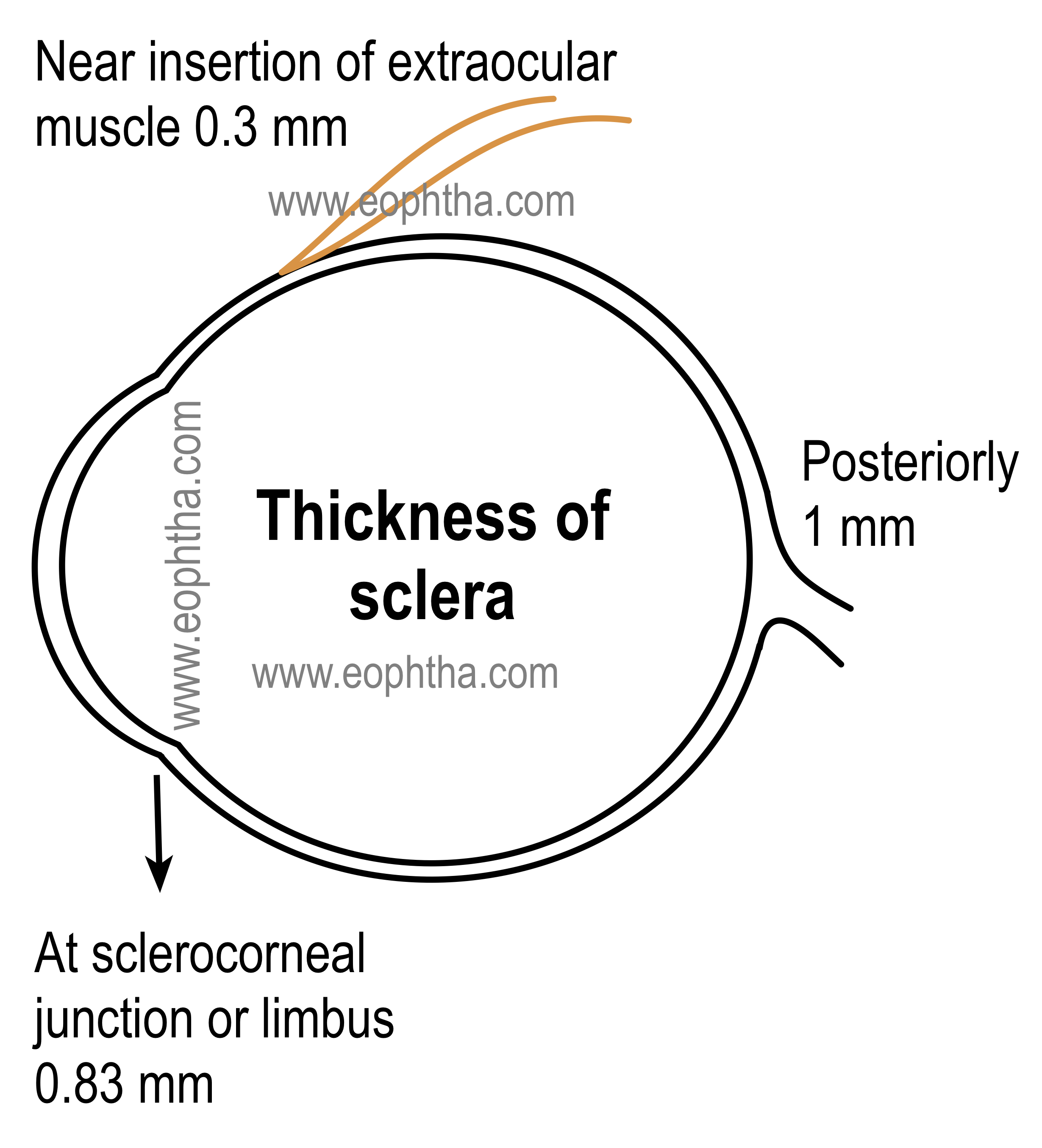 1 mm in thickness and thinnest at the insertion of extra ocular muscles (0.3 mm). The tendon of the extra ocular muscles are of same thickness here at this point of insertion, so with merging of these tendons, the collective thickness of sclera reaches to 0.6 mm here. Sclera gradually thickens towards cornea and at limbus the thickness of sclera is 0.83 mm.
1 mm in thickness and thinnest at the insertion of extra ocular muscles (0.3 mm). The tendon of the extra ocular muscles are of same thickness here at this point of insertion, so with merging of these tendons, the collective thickness of sclera reaches to 0.6 mm here. Sclera gradually thickens towards cornea and at limbus the thickness of sclera is 0.83 mm.

Important Note:
Scleral rupture following trauma primarily occurs immediately behind the insertion of the recti or in an area parallel to the limbus
Structure of Sclera:
Ultra-structurally, Sclera can be divided into three parts:
1. Episclera:The episclera is the thin densely vascularized layer of connective tissue overlying the sclera and situated below the tenon’s capsule. Apart from the vessels and unmyelinated nerve fibres, it contains bundles of collagen and also cells like fibroblast and occassional melanocytes. Anteriorly episclera blends with subconjunctival tissues and tenon’s capsule 1 to 3 mm behind the limbus. It becomes very thin and indistinct posterior to the equator. Episcleral is supplied by anterior ciliary arteries anteriorly where as posterior ciliary artery supplies the posterior part of episclera.
Note: Scleritis is always accompanied by an overlying episcleritis. On the other hand, episcleritis per se is very rarely associated with scleritis
2. Sclera proper:sclera proper or scleral stroma is also called substantia propria. Ultrasructurally, sclera is composed of collagen bundles, elastic fibres, fibroblasts and ground substances. These ground substances are proteoglycans and glycoproteins. Collagen bundles in sclera are of varying sizes and are irregularly arranged the reason why sclera is not transparent like cornea. These variation in scleral collagen fibres are more marked in mid-sclera, where the diameter of the fibres range from 50 to 400 nm. The scleral fibroblasts play an important role in synthesis and organisation of collagen,proteoglycans and glycoproteins .
3. Lamina Fusca:Lamina fusca is the innermost layer of sclera. It is characterised by abundance of pigmented cells or melanocytes, mostly migrated from choroid. The connective tissue of this layer is loosely arranged than rest of the sclera. Lamina fusca is separated from choroid by a thin potential space known as suprachoroidal or perichoroidal space.
Scleral apertures:
Sclera is penetrated by various arteries and nerves in many places. We will call such penetrations as aperture and can be discussed as :
Posterior scleral apertures:Posteriorly sclera is pierced by many structures and can be sub divided into
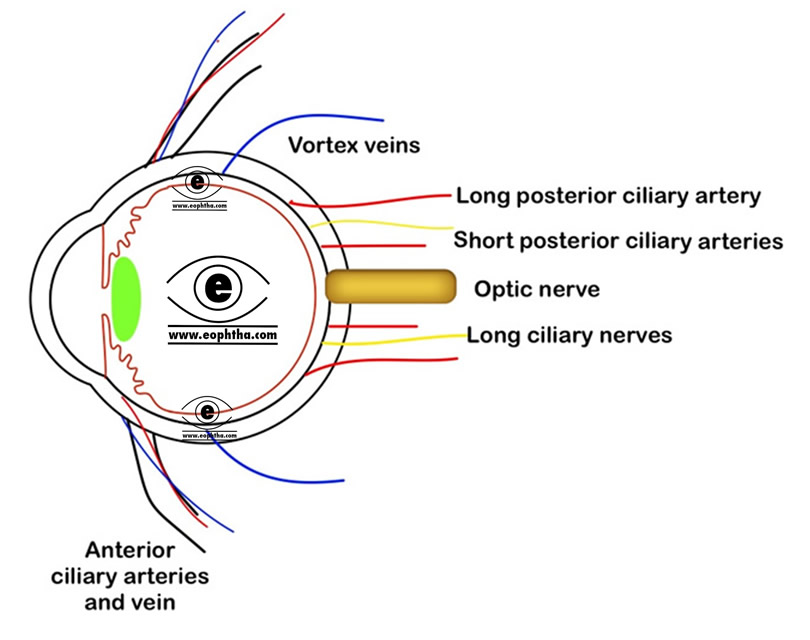
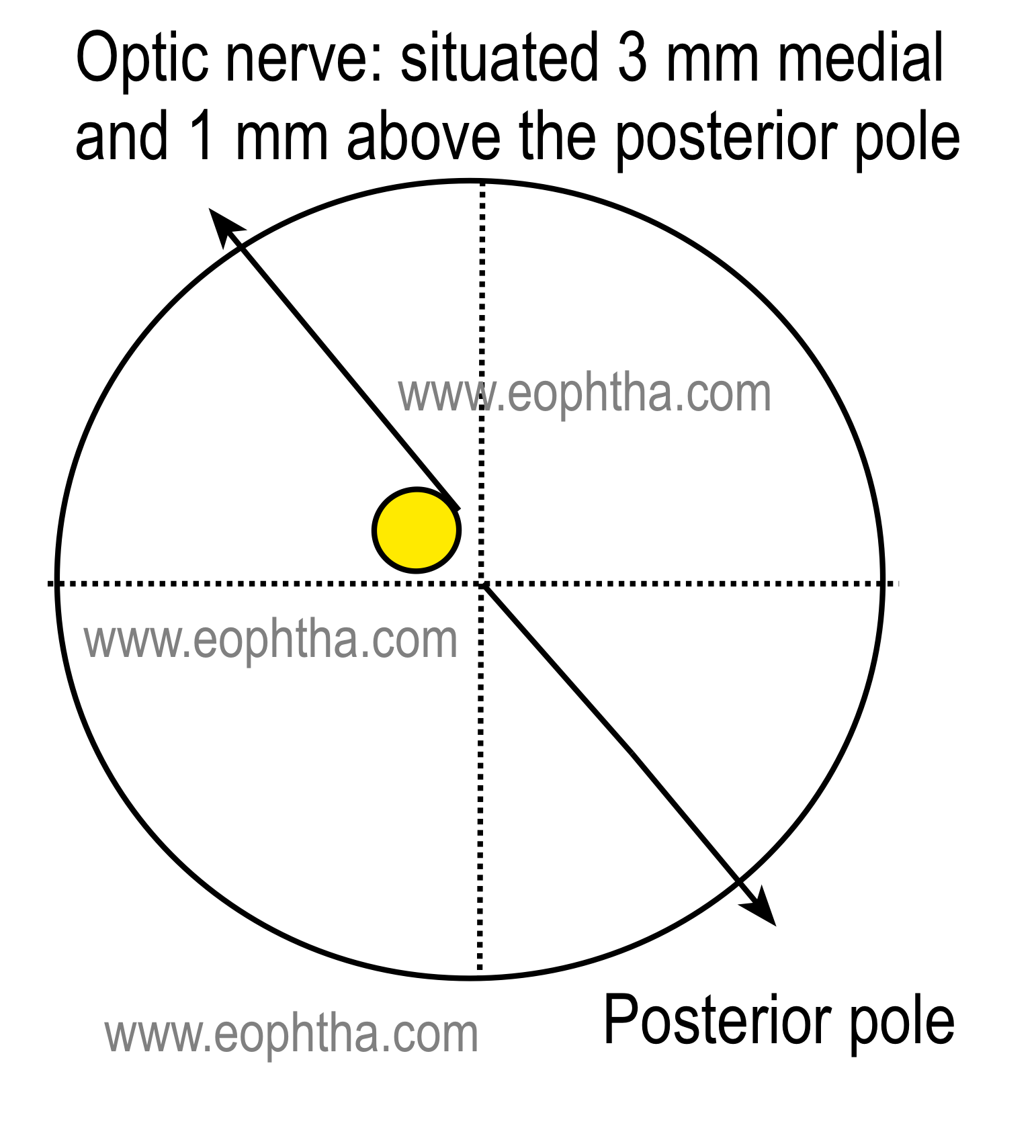
Posterior scleral foramen: Sclera is perforated by optic nerve posteriorly,3 mm medial and 1 mm superior to the posterior pole. At this point of optic nerve exit sclera blends with dural and arachnoid coverings of optic nerve and becomes a sieve like membrane internally (Lamina cribrosa is described below). Sclera is also penetrated by central retinal artery and veins.
 Other posterior apertures : sclera is pierced by 8 to 20 short posterior ciliary arteries in a ring (circle of Zinn). They are often accompanied by short ciliary nerves. Little anterior to these, long posterior ciliary arteries(two in numbers) and nerves also enter the eyeball by piercing sclera.
Other posterior apertures : sclera is pierced by 8 to 20 short posterior ciliary arteries in a ring (circle of Zinn). They are often accompanied by short ciliary nerves. Little anterior to these, long posterior ciliary arteries(two in numbers) and nerves also enter the eyeball by piercing sclera.
Circle of Zinn( also called circle of Zinn-Haller) is named after the German anatomist and botanist Johann Gottfried Zinn. Readamazing facts. It is a circular anastomosis between short ciliary arteries while piercing sclera and supplies choroid, optic nerves and pia maters
Middle scleral aperture:These apertures are situated approximately 4 mm behind or posterior to the equator and represent the exit of the four (occasionally 5 ) vortex veins. Vortex veins drain the veins of choroid, ciliary body, and iris.
Anterior scleral apertures:these are located near the insertions of the recti muscles and allow entry of anterior ciliary arteries.
Each rectus muscle has two anterior ciliary arteries with exception of lateral rectus muscle which has only one anterior ciliary artery
Few special landmark zones of sclera:
Scleral sulcus and Scleral spur :Discussed inanatomy of angle of anterior chamber.
Sclerocorneal junction or limbus :Discussed inanatomy of cornea
Canal of Schlemm:Discussed inanatomy of anterior chamber
Lamina cribrosa:Sclera is thinned with a sieve like appearance where the optic nerve fibres pierce and this region of sclera is called lamina cribrosa. However through one of these sieves, which is comparatively larger than the others, the central retinal artery and vein enter the eye .
As sclera is very weak at lamina cribrosa, it bulges outward in response to longstanding high intraocular pressure producing optic disc cupping.
Blood supply:
The episclera recieves its blood supply from the anterior ciliary arteries, anterior to the insertions of the rectus muscles and the long and short posterior ciliary arteries.
Scleral stroma is relatively avascular and receives its nutrition mainly from episcleral vascular bed and, to some extent from the underlying choroidal vasculatures. The sclera contains numerous channels or passages through which the arteries,veins and nerves pass. These channels or passages are known as emissary canals.
|
Vascular plexuses |
Locations& Vessels |
Mobility of vessels |
Colour (when inflammaed) |
Clinical importance |
|
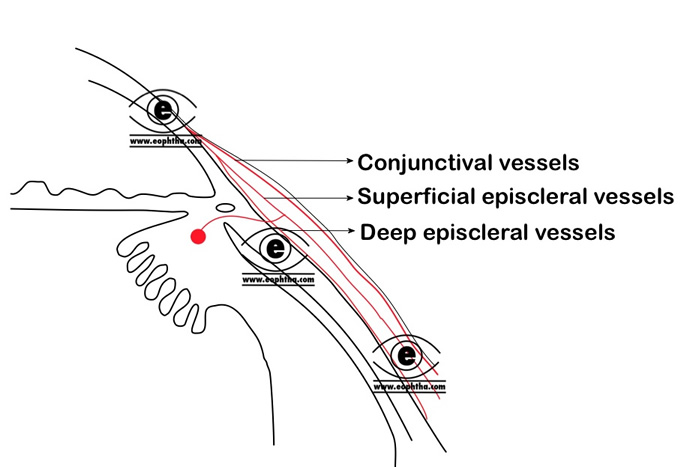
Conjunctival plexus |
Most superficial Arteries are tortuos and veins are straight. |
Freely mobile |
Bright red |
Congested in conjunctivitis. |
|
Superficial episcleral plexus |
Lies at the level of Tenon's capsule . Vessels are straight with radial configuration. |
Mobile over deeper layers |
Salmon pink |
Congested in episcleritis. |
|
Deep vascular plexus |
Lies deep to the Tenon's capsule and over sclera . Vessels are arranged in criss cross pattern. |
Immobile |
Violeaceous |
Congested in scleritis. |
Sclera is arelatively avascular structure except for some vessels that pass through the emissary canals.
The low vascularity of sclera can be explained with low metabolicdemand of the tissuebecauseoftheslowturnover rate of its collagen and cells .
Scleritis occurs more commonly anterior to the equator because of the more abundant anterior vascular supply.
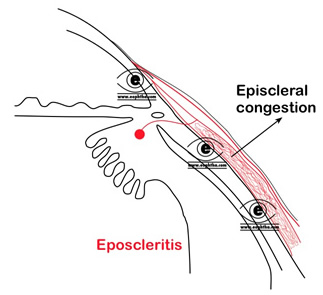
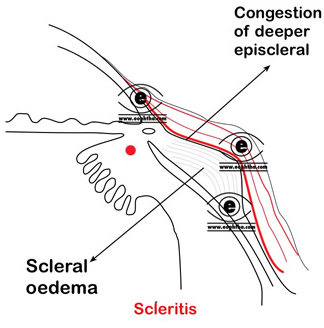
Broadly scleral inflammations can be divided into the episcleritis and scleritis. Both episcleritis and scleritis are recurrent inflammation. Episcleritis is a benign, self-limiting disease. Scleritis is a severe inflammation of the scleral tissue. This severe painful inflammatory condition is characterized by edema and cellular infiltration of the sclera and episclera. If not treated properly and well in time, it can cause a significant threat to vision.
Since sclera is mainly dependent on episclera providing a response to an inflammatory stimulus, scleritis is almost always accompanied with overlying episcleritis. However episcleritis is usually not associated with scleritis.
Sclera is richly supplied with nerves. The posterior ciliary nerves enters the sclera near the optic nerve. The anterior part of sclera is mainly innervated by the two long posterior ciliary nerves and posterior part receives nerve supply from numerous short posterior ciliary nerves.
Important Note:
Direct damage to or the stretch of these nerves is the cause for severe pain in scleritis. And because of the insertion of the extra ocular muscles in sclera, the eye movement increases the intensity of pain in scleral inflammation.