

Introduction
The cornea is prone to a variety of injuries by virtue of its location as the window of the eye. Apart from chemical injuries, physical trauma to the cornea can range from epithelial abrasions to loss of integrity of the stroma. Corneal injuries of this nature can occur in two distinct populations – in young children from play-related activities, and in young adults from due to their work environment. Although the general principles of management are not too different, special consideration in the pediatric population must be given to the timing of appropriate surgical interventions as the developing visual system in children is prone to amblyopic visual loss. Males are usually more prone to ocular injury than females; this is seen clearly in children, while the ratio of boys vs girls involved in accidents with ocular trauma is 4:1 [1].
The injuries can be caused by large blunt objects often resulting in ruptures of other parts of the ocular coats as well. On the other hand, sharp projectiles can cause more limited corneal trauma, with the nature and velocity of the injuring missile determining whether the trauma stops with the cornea or passes into the eye, damaging other structures as well. These factors also determine if the injuring agent is retained within the intraocular structures. Apart from the physical damage to the ocular structures from the injuring agent, it is also important to remember that larger projectiles are quite frequently contaminated with infective agents, and infection of the cornea and other structures may contribute significantly to the morbidity arising from such injuries. Medicolegal implications will also have to be considered.
Pre-operative Assessment
One of the most important determinations when examining a patient with corneal trauma is to distinguish between penetrating (Fig 1) and perforating injuries (Fig 2). Penetrating injuries breach the outer corneal layers but are contained within the corneal tissue itself whereas perforating injuries cause full-thickness corneal damage. The importance of this determination stems from the fact that in the latter, there is a potential for infection to enter the eye and all such eyes must be treated as potential endophthalmitis until proven otherwise. Similarly, these eyes are also at risk of having a retained intraocular foreign body, and investigations for the same are mandatory, and in the event of such a complication, the care of the eye may require the assistance of a Vitreo-retinal colleague. Finally, penetrating corneal injuries may not require early or immediate surgical intervention, whereas perforating injuries often do.
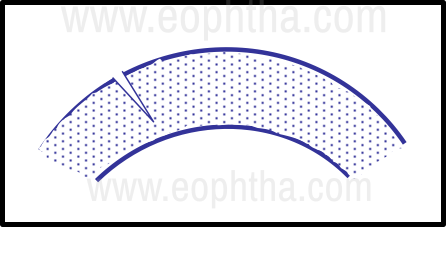
Figure 1 - Penetrating corneal injury
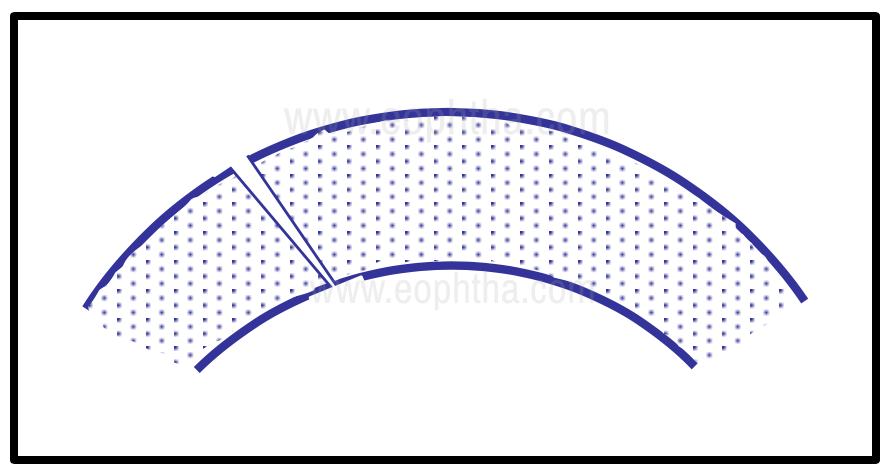
Figure 2 - Perforating injury
It is important to first look for co-existing life-threatening systemic injuries in cases of severe corneal trauma, which if present should take priority in management. A brief history as to the nature of the injuring agent and the circumstances of the injury are relevant as they help determine the possibility of a retained foreign body and its nature, the chances of infection, and possible medico-legal issues. A quick assessment of the visual acuity of the injured eye must be performed before commencing the eye examination. In ocular trauma, the occurrence of an anterior or posterior hemorrhage may preclude assessment of the visual potential of the eye and also the state of the intraocular structures during subsequent examinations. Documentation of very poor visual acuity at presentation serves to protect the examiner in the event of subsequent medico-legal litigations. Of particular importance to corneal trauma is whether the location of such damage involves the visual axis of the eye. This may help guide discussions regarding the visual consequences of the injury and the need, nature, and timing of subsequent surgical interventions.
The presence of foreign bodies located within the corneal stroma in penetrating corneal trauma and within the tissues of the eye in perforating ocular trauma should be looked for. The presence of and potential for infection must be determined. The status of tetanus prophylaxis of the individual must be ascertained and in the event of a surgical repair being considered, the timing and nature of the last meal of the patient must be recorded, and the patient should be instructed to remain on a nil oral diet since general anesthesia may have to be used during the surgical repair. In addition to the above considerations, perforating injuries of the cornea are often associated with iris prolapse, lens damage, and retinal and choroidal injury. The eye must also be assessed for evidence of endophthalmitis at presentation.
Classic signs of an associated scleral rupture are the presence of a boggy chemosis of the conjunctiva, subconjunctival hemorrhage, often with hyphema and distortion of the pupil, a soft eye, and in severe cases, distorted globe contour (the “scleral step sign” wherein one of the scleral wound edges protrudes more prominently than the eye’s normal contour). These often occur in the superonasal quadrant or at the site of the insertion of the rectus muscles, where the sclera is the thinnest [2].
Once the assessment is complete, the eye must be patched with a pad and a rigid shield while awaiting surgical repair, to prevent further injury. The patient is instructed to avoid straining and to be in bed rest until surgery. In this article, the principles of management of corneal trauma are considered.
Surgical principles
It is best to have a soft eye with no upthrust when performing surgical repair of the corneal tear. Thus, a deep plane of general anesthesia is desirable, and while the speculum chosen should provide good exposure of the cornea, it is important to avoid pressure on the globe from the speculum. Bridle sutures are best avoided and povidone irrigation of the ocular surface should not be performed because of the communication with the intraocular contents in perforating injuries.
The ocular surface should be irrigated well with a sterile balanced salt solution to provide thorough irrigation of the wound and ensure that all debris and contaminants are removed from the surgical field. In eyes with suspicion of corneal infection, a swab from the edges of the wound is helpful in the management of an infection in the postoperative period. A better inspection of the damage is possible in the operating room and the morphology of the tear, scleral and limbal involvement and any loss of corneal tissue is determined.
Sutures for the wound are readied. Generally, 8-0 nylon for sclera, 9-0 nylon for limbus, 10-0 nylon for cornea, and 11-0 nylon for complex corneal tears are preferred. The use of polyglactin (8-0 or 10-0 Vicryl) sutures is ideal for scleral and conjunctival closure. If iris is incarcerated in the wound and has not actually exited onto the surface of the eye, the use of intracameral pilocarpine or adrenaline may be tried to see if the movement of the iris is able to retract the incarcerated tissue into the anterior chamber. However, if the iris has prolapsed out onto the corneal surface and has been exposed for greater than 24 hours, there is a risk of introducing surface epithelium into the eye if the tissue is reposited. In this situation, it is important to abscise the prolapsed iris, by gently tugging on it and amputating it flush with the corneal surface. The presence of a minimal ooze of blood from the cut end is a sign that all devitalized iris has been excised and only viable tissue is retained.
In the presence of a shallow, but formed anterior chamber, a diamond knife is used to create a paracentesis opening before manipulations of the wound result in a total loss of the anterior chamber. This provides a port of access into the anterior chamber for use during subsequent maneuvers, such as the introduction of viscoelastic to protect the endothelium, injection of air to maintain the chamber during suturing, and the use of a spatula to release iris adhesions to the wound. Excessive manipulations through the corneal tear are to be avoided.
After determining the configuration (especially in common linear tears), it is best to start the suturing at the limbus, where the presence of the limbal palisades provides a good visual clue to the anatomic landmarks and allows precise apposition of the tear edges. Once the limbus has been reconstituted, sutures are placed to divide the tear into equal halves and the process is continued until the entire length of the tear has been sutured. Another important principle is to ensure that the suture placement is perpendicular to the orientation of the tear at the point of the suture (Fig 3).
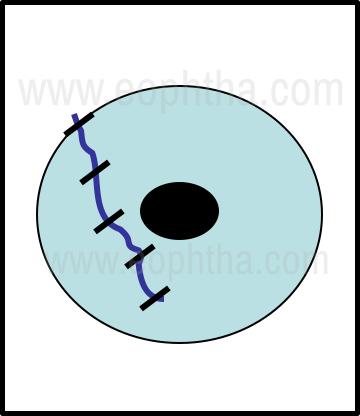
Figure 3 - Linear corneal tear suturing
When dealing with curvilinear tears that extend onto the center of the cornea, it is important to use the sutures to try and restore the shape of the corneal vault. Since deep, long, and tight sutures tend to flatten the cornea curvature, these are used in the corneal periphery. As the corneal center is approached, shorter, more superficial, and less tight sutures are employed. In very curved tears, continuous sutures are best avoided as they tend to try and straighten the suture line when tightened resulting in distortion of the corneal surface. Since each suture supports the wound for a distance equal to its length, it is possible to determine the number of sutures that are ideal for a given length of tear (Fig 4).
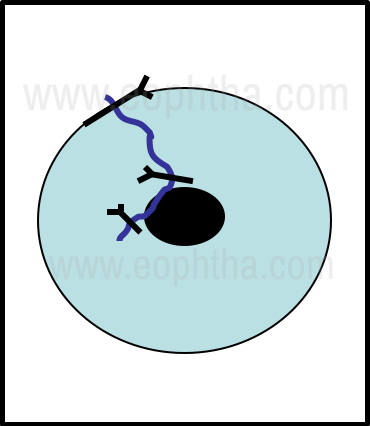
Figure 4 - Curvilinear corneal tear suturing
It is important to ensure that the sutures produce good apposition of the edges of the corneal tear. This helps reduce the degree of induced irregular astigmatism. To achieve this goal, the bites should be of equal depth in both margins of the tear. In corneal tears complicated by extensive edema of the stroma in the edges, it is necessary to use long bites that are anchored in the normal corneal stroma, as this allows better judgment of the extent of suture tightening that is required. In shelved corneal tears, it is important to use the posterior edge of the tear as the guide when determining the length of the suture bite used to oppose the two margins of the tear (Fig 5).
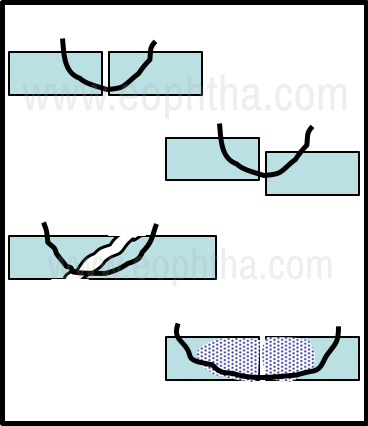
Figure 5 - Principles of corneal suturing
Knot ends of 10-0 nylon sutures that are used for corneal tear repair are best buried in the corneal stroma as they can cause significant discomfort and corneal erosions if left exposed on the surface. After burying the knot, a sharp pull in the reverse direction will reverse the orientation of the suture ends within the stroma and facilitate easier removal at a later date (Fig 6).
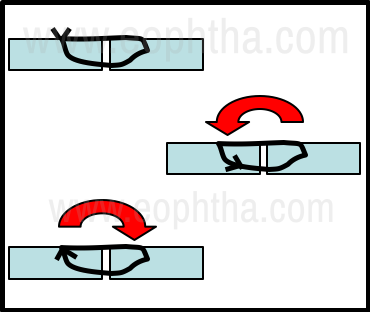
Figure 6 - Principles of corneal suture knot management
In shelving corneal tears, it is preferable to bury the knot on the side of the shorter anterior bite as the direction of the force applied during suture removal will support the wound and reduce the chances of wound dehiscence (Fig 7).
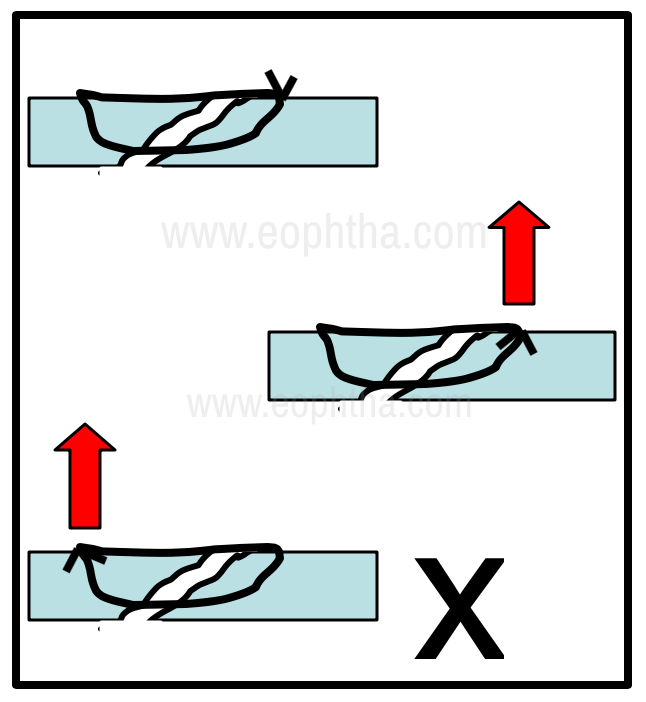
Figure 7 - Management of sutures in a shelving corneal tear
Complex tears with a stellate configuration are harder to manage. It is prudent to suture the individual limbs of the tear first and tackle the stellate apex last. Since this is often composed of thin slivers of corneal tissue, a finer suture like 11-0 nylon may be preferable. The use of a purse-string suture is effective in closing such wounds but may lead to pursing and fish-mouthing of the apex of the tear in some instances. (Fig 8).
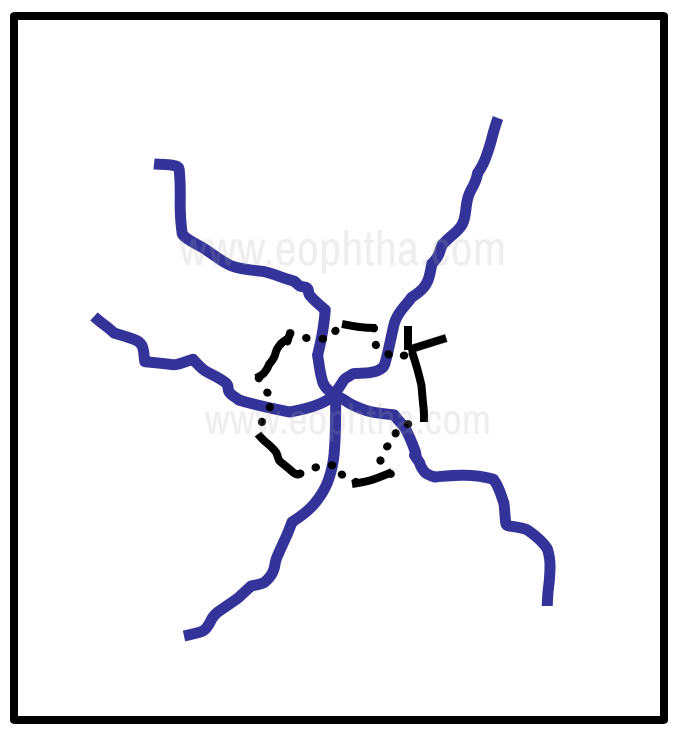
Figure 8 - Management of a stellate corneal tear
In tripartite tears, to avoid this problem, a variant of the purse-string suture, called the ‘star’ suture, may be used. The bridging sutures crossing the apex help prevent fish mouthing of the apical tissues (Fig 9).
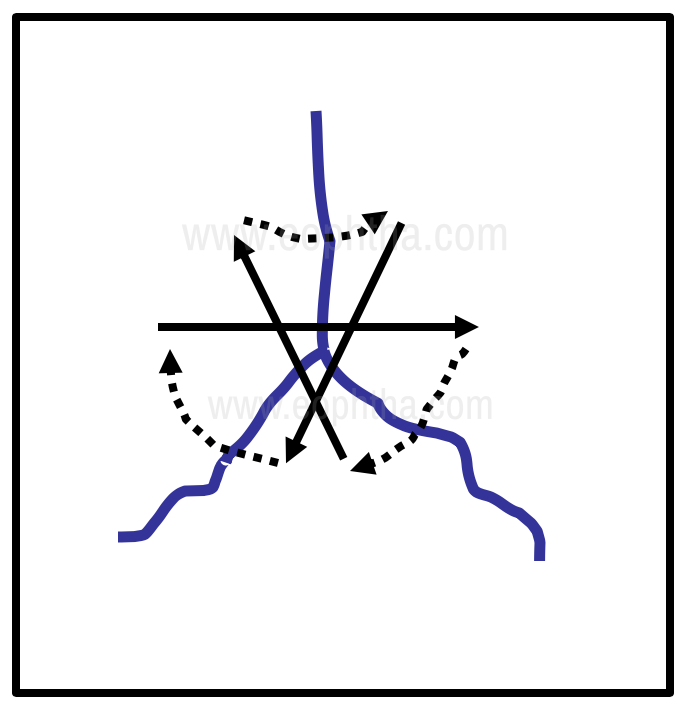
Figure 9 - Management of a tripartite corneal tear
A leaking wound at the conclusion of the procedure is sometimes seen, especially when there has been some degree of tissue loss. If the leak is minimal it often responds to the use of air in the anterior chamber and support with a bandage contact lens. If it is due to tissue loss but is minimal, the use of n-butyl cyanoacrylate glue or fibrin glue may be used to seal the leak, till corneal healing occurs. However, in cases where there has been more extensive tissue loss, corneal tissue transfer may be required to restore corneal integrity. A very challenging situation is in eyes with megalocornea or keratoglobus that have suffered a corneal rupture. These thin corneas are prone to corneal tears following relatively minor trauma. The extremely thin cornea in such eyes often does not support suturing, and multiple leaks from the suture tracks are often seen. The primary corneal replacement may have to be considered for globe salvage in eyes with megalocornea that has undergone severe trauma. It is important that such patients are properly counseled regarding the risks and are encouraged to constantly wear protective spectacles.
The suture removal should be performed at the appropriate time, when adequate wound healing has occurred, using a technique that reduces the risk of tracking epithelium and debris into the suture tract. The corneal surface is first flushed with a sterile solution to remove any debris on the surface of the suture. Antibiotics or povidone-iodine is applied prior to the procedure. The suture is cut flush with the surface of the cornea at the end away from the suture knot, by introducing the tip of a blade or sterile disposable needle under the loop of suture. The instrument is again inserted under the loop of suture on the corneal surface at the knot end and the cut length of the surface suture is retracted onto the surface, without disturbing the corneal epithelium overlying the suture length. The exteriorized suture is then aligned with the knot and gradual pressure helps pull the entire suture out of the tract. (Fig 10).
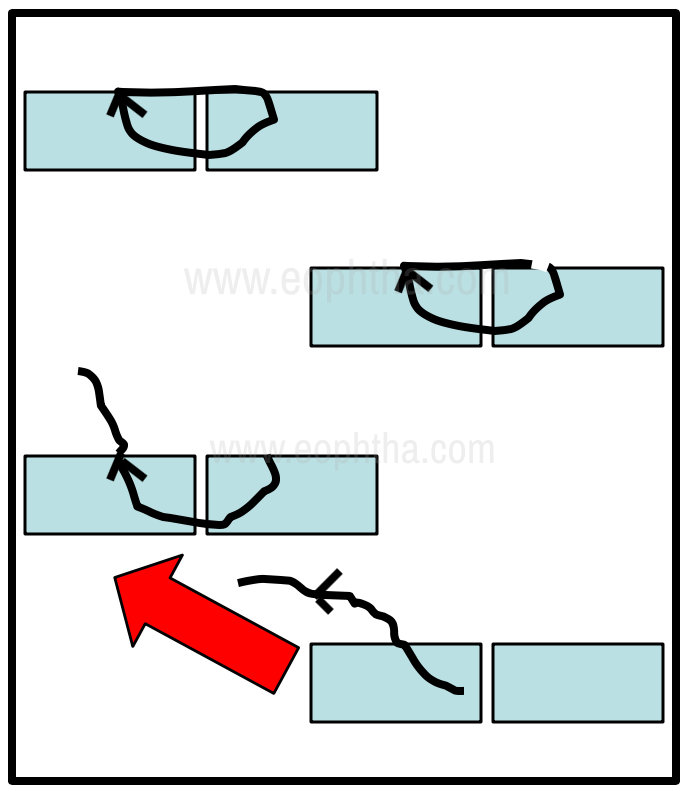
Figure 10 - Principles of corneal suture removal
Penetrating trauma - Management
When examining the cornea, the length, depth, and morphology of the corneal tear, presence of limbal involvement, the extent of corneal edema, and the presence of tissue loss if any must be determined (Fig 11).
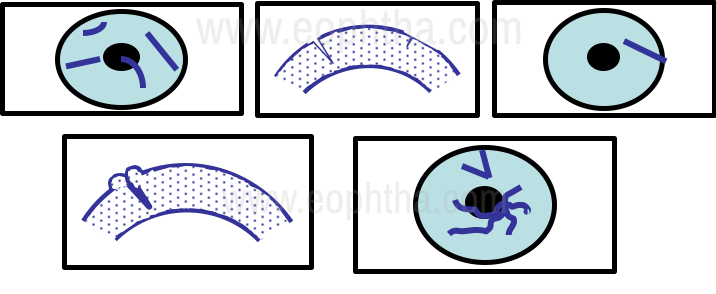
Figure 11 - Assessment of Penetrating corneal trauma
General principles regarding the treatment of penetrating corneal trauma include the use of tetanus prophylaxis if required, antibiotic cover, the use of lubricants, and a protective shield. Specific therapy is determined based on the characteristics of the wound. In the simplest situation, when the wound is less than 2 mm, is of less than 25% of corneal thickness, and is away from the visual axis with no associated edema, treatment would consist of careful observation with the use of prophylactic topical antibiotics, lubricants and assessing if there are any changes in refraction after wound healing (Fig 12).
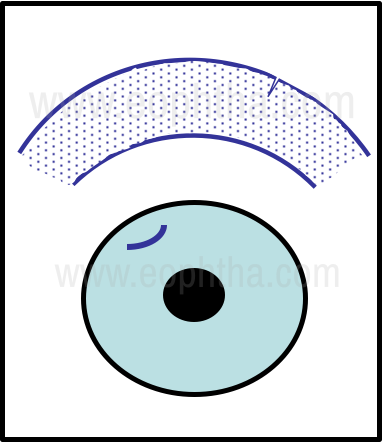
Figure 12 - Small Penetrating tear
Larger tears extending 5 to 6 mm in length, involving 50% of corneal thickness, sparing the visual axis, having a shelving configuration, can be managed by splinting the tear with a bandage contact lens to support wound healing. Once the corneal edema resolves and scar progression is completed, ensuing changes in refraction can be addressed. Medical management includes the liberal use of topical lubricants along with topical antibiotic prophylaxis. (Fig 13).
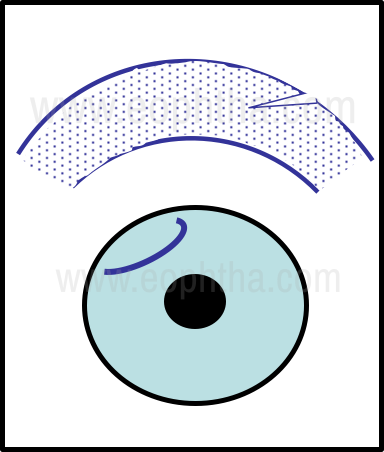
Figure 13 - Large Penetrating tear
In the complicated situation where the corneal tear extends longer than 6 mm and involves a corneal depth greater than 50%, with visual axis involvement and a complex morphology – often stellate, it is necessary to suture the wound appropriately. (Fig 14).
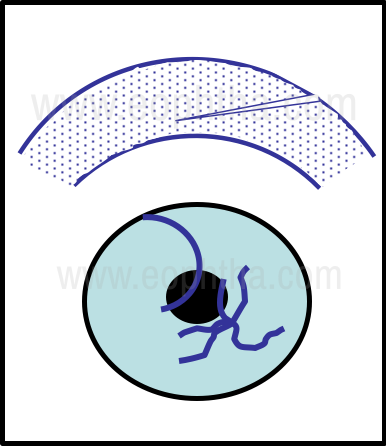
Figure 14 - Complex Penetrating tear
Under antibiotic cover, after confirming the clinical absence of corneal infection, the careful introduction of topical steroids may help reduce the extent and severity of corneal inflammation and resultant scarring. Sutures should be removed at the appropriate time to lessen the chances of complications from loosening, vascularization, and infection. The involvement of the visual axis will require further intervention to restore vision quality.
Perforating trauma – Management
As with penetrating trauma, after a detailed assessment, treatment is considered, although in this context it is often surgical. However, in contrast to penetrating corneal trauma, topical medications especially ointments are avoided as the injury tract provides a pathway into the eye. Conservative management by use of a bandage contact lens can only be considered in the mildest form of such an injury with the following features:
- the small tract that is less than 2 mm in size
- self-sealed and Seidel test negative
- no iris prolapse or uveal tissue incarceration
- absence of signs of infection
In eyes with larger tears, that are Seidel test positive, or have an active leak with a flat anterior chamber, iris prolapse, and or tissue loss, it would be best to suture the wound closed. General anesthesia is preferred, although very small, uncomplicated tears can be repaired using preservative-free topical anesthetics. In any event, the eye should be protected with a pad and rigid shield till surgery, and if general anesthesia is considered, it would be necessary to avoid the use of a depolarizing muscle relaxant like succinylcholine, and to remove the supportive pad only after anesthesia induction is completed.
Visual Rehabilitation
Common to both penetrating and perforating corneal trauma, injuries involving the visual axis will compromise visual function to varying extents after wound healing, depending on the location and density of the corneal scar. In minimal scarring, a change of spectacles may suffice, but with the increasing irregularity of the corneal surface, the use of a rigid contact lens may have to be considered. The presence of a dense scar with severely reduced visual acuity will require corneal replacement surgery. The techniques of lamellar and full-thickness corneal replacement have already been discussed in earlier chapters. The use of the appropriate surgical procedure is at the discretion of the treating surgeon, (considering scar morphology and surgeon experience). The use of Phototherapeutic keratectomy (PTK) can be considered for superficial scars.
Conclusion
Although corneal trauma is not unusual, provided it is recognized promptly and attended to, the resulting morbidity can be minimized. Paying attention to the principles described in the chapter can help restore useful visual function in many of these eyes.
References
LaRoche GR, McIntyre L, Schertzer RM. Epidemiology of severe eye injuries in childhood. Ophthalmology. 1988 Dec;95(12):1603–7.
Yucel OE, Demir S, Niyaz L, Sayin O, Gul A, Ariturk N. Clinical characteristics and prognostic factors of scleral rupture due to blunt ocular trauma. Eye (Lond). 2016 Dec;30(12):1606–13.
Corneal Surgery – Theory, Technique, Tissue (4th ed). Frederick Brightbill Peter McDonnell Charles McGhee Ayad Farjo Olivia Serdarevic, Mosby, 2008.
Corneal Trauma – Prinicples and Practice. Ferenc Kuhn, Dante J Pieramici. Thieme, 2002.
Eye Trauma - Shingleton, Bradford J.; Hersh, Peter; Kenyon, Kenneth R. CRC Press, 1991.
Eye Surgery – An introduction to Operative Technique. Georg Eisner. Springer Verlag, 1980.