
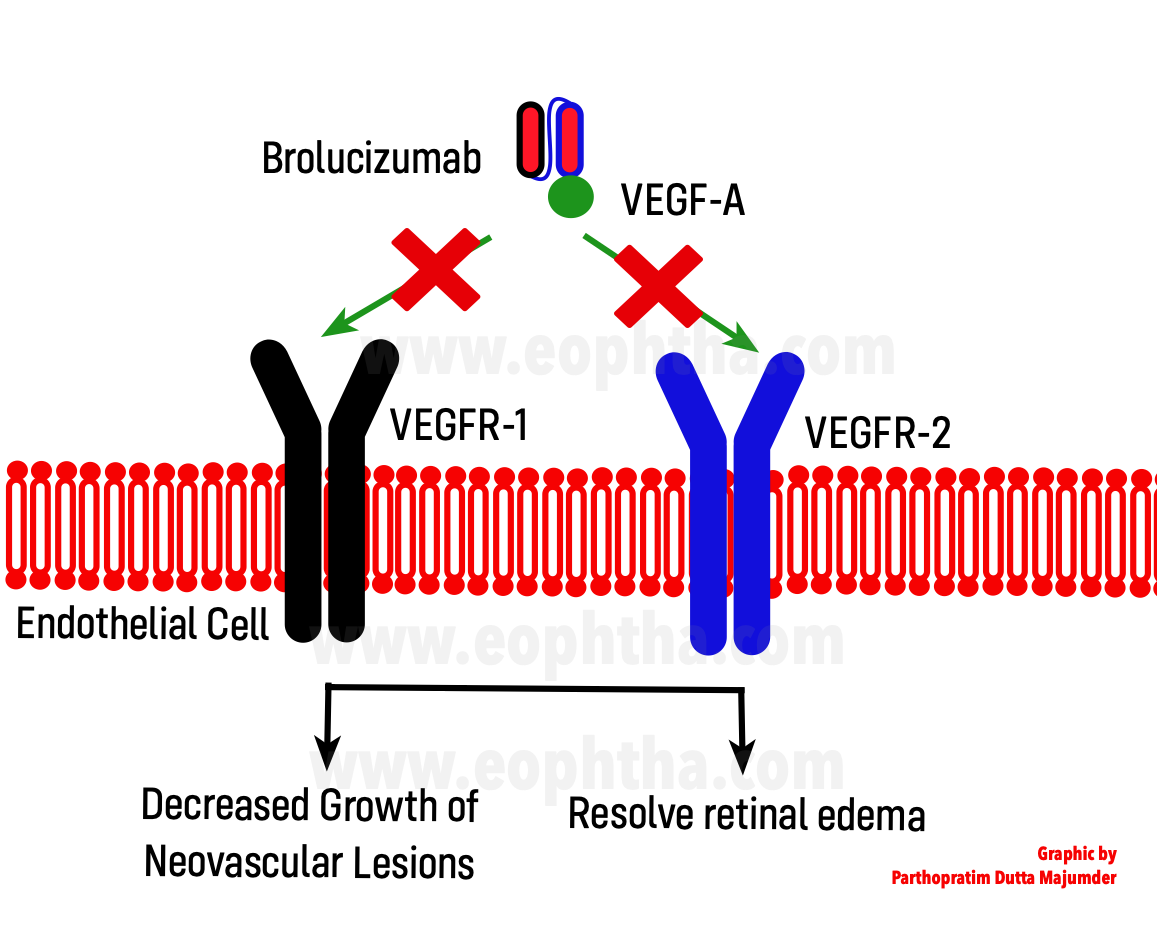
1. Brolucizumab is a humanized, single-chain variable fragment (scFv) antibody with a molecular mass of approximately 26 kDa that inhibits VEGF-A.[1] (An scFv is an autonomous binding agent that is no longer dependent on a heavy molecular support structure but still retains the full binding capacity to its target).

2. The pharmacokinetics of a single intravitreal (IVT) injection of Brolucizumab in cynomolgus monkeys revealed a mean terminal half-life of 2.4 ± 0.3 days in all ocular compartments. It was cleared from the serum with a mean half-life of 51 hours (approximately 2 days).[2]
|
Brolucizumab |
Bevacizumab |
Ranibizumab |
Aflibercept |
|
|
Molecule |
Short-chain variable fragment |
Full antibody (IgG) |
Monoclonal humanized antibody format |
Fusion protein |
|
Clinical dose in neovascular ARMD |
6 mg |
1.25 mg* |
0.5 mg |
2 mg |
|
Equivalent Molar dose |
11.2-13.3 |
0.4-0.5 |
0.5-0.6 |
1.0 |
Table: Molecular properties of anti-VEGF agents (ARMD= Age-related macular degeneration, *= off label use)
3. The safety, tolerability, and efficacy of a single IVT administration of brolucizumab in patients with treatment naïve neovascular age-related macular degeneration (nAMD) were first demonstrated in the SEE study. [3] This study investigated a single intravitreal injection of brolucizumab (0.5, 3, 4.5, or 6 mg) compared with ranibizumab 0.5 mg. This proof-of-concept study demonstrated that 6 mg of brolucizumab was tolerable and effective in reducing central subfield thickness (CST) and improving best-corrected visual acuity (BCVA). The results of the SEE study provided evidence for an effective dose (6 mg) for subsequent studies.
4. The OSPREY Phase 2 study examined the efficacy and safety of brolucizumab compared with aflibercept (approved for 8 weekly dosings) to treat nAMD.[4] The OSPREY study demonstrated that brolucizumab was as efficacious as aflibercept in an 8 weekly regimen with regard to BCVA, and brolucizumab treatment achieved a greater fluid resolution compared with aflibercept.
5. The USFDA approved Brolucizumab (6mg/0.05 ml single-dose vial marketed as Beovu by Novartis, USA) for the treatment of nAMD based on results of the pivotal HAWK and HARRIER studies [5], which were 2-year, double-masked, multicenter Phase 3 studies. These studies demonstrated that a brolucizumab q12-week regimen maintains efficacy and safety while reducing the treatment burden associated with regular IVT injections for patients with nAMD. Brolucizumab (q12/q8- week) achieved non-inferiority in mean change in BCVA compared with aflibercept (q8-week) in the Phase 3 trials; however, brolucizumab was a more potent drying agent, with a significantly greater proportion of patients demonstrating an absence of intra-retinal fluid/sub-retinal fluid at both weeks 16 and week 48 compared with aflibercept.
6. The comparatively more potent SRF-resolution effect of Brolucizumab has been ascribed to better penetration into the retinal tissue and its low-molecular-weight. (the anti-VEGF binding capacity are 11 and 22 times greater than what can be clinically administered for aflibercept and ranibizumab, respectively).[1]
7. The most common adverse events (>=5% of patients) with Brolucizumab were blurred vision, cataract, subconjunctival hemorrhage, vitreous floater, eye pain, and intraocular inflammation (which included anterior chamber flare, anterior chamber inflammation, iritis, iridocyclitis, vitreous haze, vitritis, and choroiditis).[5]
8. Recently, more serious adverse events have been reported. The occlusive events may span from peripheral vasculitis to occlusion of large retinal arteries around the optic nerve or macula with severe vision loss.[6,7]
9. Brolucizumab is available in India under the trade name of Pagenax (120mg/ 1ml vial), currently in the price range of around 23 to 25 thousand INR.
10. Thus, the advantages of Brolucizumab are its small molecular size, prolonged duration of action (leading to potential cost-effectiveness), better penetration, and relatively quick clearance. However, one must consider the potentially serious adverse events before administration.
References:
- Nguyen QD, Das A, Do DV, Dugel PU, Gomes A, Holz FG, Koh A, Pan CK, Sepah YJ, Patel N, MacLeod H, Maurer P. Brolucizumab: Evolution through Preclinical and Clinical Studies and the Implications for the Management of Neovascular Age-Related Macular Degeneration. Ophthalmology. 2020 Jul;127(7):963-976.
- Nimz EL, Van’t Land CW, Yáñez JA, Chastain JE. Intraocular and systemic pharmacokinetics of brolucizumab (RTH258) in nonhuman primates. Poster presented at: The Annual Meeting of the Association for Research in Vision and Ophthalmology (ARVO); May 1-5, 2016, Seattle, Washington.
- Holz FG, Dugel PU, Weissgerber G, et al. Single-chain antibody fragment VEGF inhibitor RTH258 for neovascular agerelated macular degeneration: a randomized controlled study. Ophthalmology. 2016;123:1080-1089.
- Dugel PU, Jaffe GJ, Sallstig P, et al. Brolucizumab versus aflibercept in participants with neovascular age-related macular degeneration: a randomized trial. Ophthalmology.2017;124:1296-1304.
- Dugel PU, Koh A, Ogura Y, Jaffe GJ, Schmidt-Erfurth U, Brown DM, Gomes AV, Warburton J, Weichselberger A, Holz FG; HAWK and HARRIER Study Investigators. HAWK and HARRIER: Phase 3, Multicenter, Randomized, Double-Masked Trials of Brolucizumab for Neovascular Age-Related Macular Degeneration. Ophthalmology. 2020 Jan;127(1):72-84.
- Baumal CR, Spaide RF, Vajzovic L, Freund KB, Walter SD, John V, Rich R, Chaudhry N, Lakhanpal RR, Oellers PR, Leveque TK, Rutledge BK, Chittum M, Bacci T, Enriquez AB, Sund NJ, Subong ENP, Albini TA. Retinal Vasculitis and Intraocular Inflammation after Intravitreal Injection of Brolucizumab. Ophthalmology. 2020 Oct;127(10):1345-1359.
- Witkin AJ, Hahn P, Murray TG, Arevalo JF, Blinder KJ, Choudhry N, Emerson GG, Goldberg RA, Kim SJ, Pearlman J, Schneider EW, Tabandeh H, Wong RW. Occlusive Retinal Vasculitis Following Intravitreal Brolucizumab. J Vitreoretin Dis. 2020 Jul;4(4):269-279.