

What is astigmatism?
Astigmatism is a type of refractive error/ametropia that occurs when parallel rays of light entering the ocular media (non-accommodative state) are not focused well on the retina. In an optical system with astigmatic error, light rays propagate in two different planes and the incident light rays fail to converge at a single focal point rather they have two different foci. This causes a difference in the degree of refraction in different meridians and the retinal images of both distant and near objects tend to appear blurred. In the case of astigmatism, the steepest and flattest meridians of the eye are called the principal meridians and the amount/degree of astigmatism is calculated as the difference in their refractive powers.
What are the symptoms of astigmatism?
Astigmatism leads to symptoms such as blurred or distorted (horizontal, vertical, or diagonal) vision, asthenopia including headache, eye strain, fatigue, etc., squinting/squeezing of eyes, head tilt, difficulty in driving at night/low lit conditions, glare, photophobia, etc.
What are the types of astigmatism?
Based on the anatomical location/etiology
- Anterior or Posterior corneal astigmatism: a most common type, caused by the irregularities in the anterior or posterior corneal curvature (e.g. Keratoconus, Corneal scar, Limbal dermoid, etc.)
- Lenticular astigmatism: caused by the variation in the curvature (e.g. Lenticonus), position (e.g. Subluxation), or refractive index (e.g. Nuclear sclerosis) of the crystalline lens
- Retinal astigmatism: Commonly caused by the oblique placement of the macula, directional variability in the arrangements of photoreceptors, etc.
Based on the magnitude of astigmatism
- Mild: < 1.00 D
- Moderate: > 1.00 to 2.00 D
- Severe: > 2.00 D to 3.00 D
- Extremely severe: > 3.00 D
Based on the axis of the principal meridian/orthogonality
- Regular: Most common type in which the principal meridians are perpendicular to each other i.e. 90º apart
- Irregular: Principal meridians are not 90º apart instead they are separated by any other angle and can be macro-irregular or micro-irregular astigmatism
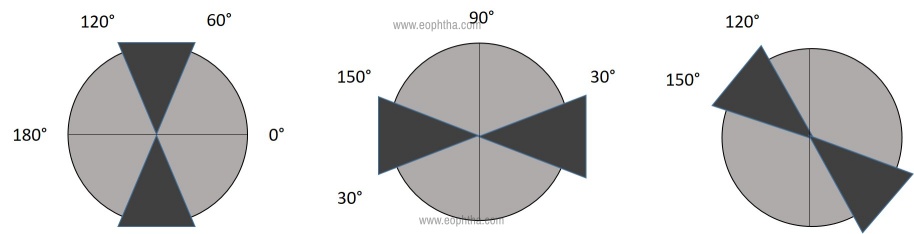
Based on the location of the steepest meridian as illustrated in Figure 1
- With-the-rule: with steep vertical meridian, 90 ± 30 (e.g. +0.00 DS/-0.75 DC x 180)
- Against-the-rule: with steep horizontal meridian, 180 ± 30 (e.g. +0.00 DS/-1.25 DC x 90)
- Oblique: the steepest curve lies in between degrees outside that of 90 ± 30 and 180 ± 30 (i.e. between 120 and 150 degrees and 30 and 60 degrees). For e.g. +0.00 DS/-2.00 DC x 40
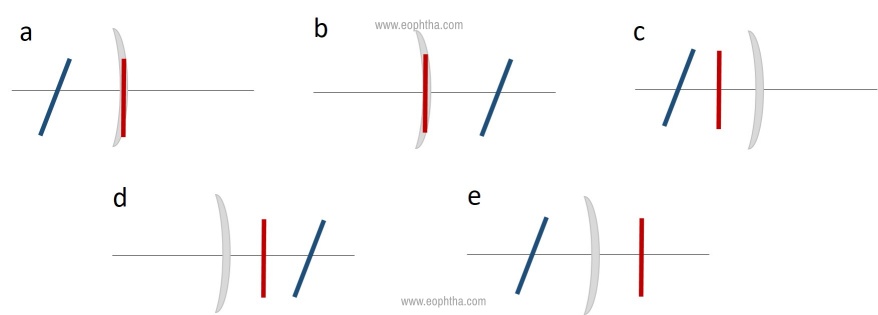
Based on the location of the focal lines as illustrated in Figure 02
- Simple myopic: +0.00 DC x 90/-2.00 DC x 180
- Simple hyperopic: +3.25 DC x 110/+0.00 DC x 20
- Compound myopic: -2.00 DC x 170/-3.50 DC x 80
- Compound hyperopic: +2.00 DC x 180/+1.75 DC x 90
- Mixed: +4.00 DC x 180/-3.00 DC x 90
What are the clinical methods to diagnose astigmatism?
- Comprehensive clinical history: Specific focus on symptoms for arriving at the tentative diagnosis (Refer to the paragraph on symptoms)
- Visual Acuity (VA) assessment:
- The level of visual acuity depends on the type and severity of the astigmatism
- The variation in acuity depends on the accommodative demand on each type of astigmatism
- VA is reported to be better when one of the focal lines lie on the retina irrespective of the axis orientation as in the case of simple myopic/hyperopic astigmatism
- Objective and Subjective refraction including refinement procedures
- Stenotopic slit (a refractive tool): It is a black opaque disc (trail case accessory) with a rectangular slit aperture (1-2 mm in width by 15 mm in length) that is useful to screen a high degree of astigmatism and find out its axis. The opaque part limits the admission of light and allows light rays to pass via a single meridian
-
-
- After achieving the best spherical correction, for e.g. -2.00 DS, fog the eye with +1.50 DS, then place the slit in front
- Rotate the slit manually, 360°, until the patient reports the clearest vision through the slit
- For e.g. if the vision is clearest when the slit is coinciding with axis 90, then it is our first principal meridian
- Slowly defog in +0.25 DS steps until the patient reports the best VA
- Then rotate the slit by 90°apart (in this case 180°) and reduce the remaining fogging lens in +0.25 DS steps, until the patient reports good VA
- The direction of the slit where the patient reports the best VA is the axis of the cylinder and the amount of defogging done to get the best VA in the power meridian is the magnitude of the cylinder
-
-
- Astigmatic fan: is used to detect the presence of astigmatism, and if present it helps in determining the axis and magnitude of the cylinder. The test chart consists of a series of radiating lines mostly spaced at 10°intervals (rays of the rising sun).
-
-
- Occlude one eye of the patient and fog the testing eye with +1.50 DS
- Ask the patient to look at the astigmatic fan
- If there is no presence of astigmatism, all lines will appear equally clear, sharp, and dark
- If astigmatism is present, one or more, lines of the chart will appear clear, sharp, and dark than the others
- The patient is instructed to identify the clock position of the meridian which is blurred, hence the axis of the correcting cylinder is at the right angle/perpendicular to the clearest/sharpest line
- Now the cylindrical axis is set and the power is increased until all the lines are equally clear, then defogging can be performed
-
-
- JCC (Jackson Cross Cylinder): A combination of two equal yet opposite astigmatic lenses with spherical equivalent being zero. JCC is useful in refining the axis of the astigmatic error followed by fine-tuning the power
- Done monocularly under fogging or without (two schools of thought)
- Refining astigmatic axis - Align JCC handle parallel to the corrective cylinder’s axis, flip the side and ask the patient if both the sides are equal or slightly better than the other
- Depending on the response, rotate the cylindrical lens axis 5° towards the Red dot of JCC
- Again align the JCC handle to the new cylindrical axis, flip and repeat the question again (Side 1 or 2), rotate in the same direction or reverse the rotation according to the patient’s response
- Endpoint – Letters equally clear/blurred in both the sides
- Refining astigmatic power – Align JCC axis parallel to the corrective cylinder’s axis, flip the side, and ask the patient if both the sides are equal or slightly better than the other
- If the patient reports the red line side is better, then add -0.50 to the existing power or the other way round
- To maintaining the circle of least confusion on the retina, a +0.25 D is added for every -.050 DC or vice versa
- Again align the axis of the JCC to the new cylindrical axis, flip and repeat the question again (Side 1 or 2), adjust the power of the cylinder according to the patient’s response
- Endpoint – Letters equally clear/blurred in both the sides
- JCC (Jackson Cross Cylinder): A combination of two equal yet opposite astigmatic lenses with spherical equivalent being zero. JCC is useful in refining the axis of the astigmatic error followed by fine-tuning the power
- Keratometry:
- Measure of the curvature and refractive power of the cornea,
- Determines the degree of astigmatism and its axis of orientation
- Helps to identify corneal pathology, to differentiate refractive error as corneal or axial, aids in IOL power calculation
- Higher diagnostics including Corneal topography, Pentacam, Aberrometry etc.
What are the management options for astigmatism?
Optical correction
- Eyeglasses
- Plano-cylindrical lenses
- Sphero-cylindrical lenses
- Aspheric lenses (Any ophthalmic refracting surface other than a spherical refracting surface comes within the classification of aspheric, in which one of the type is ‘Toric surfaces’ which are primarily used for the correction of astigmatism)
- Contact lenses
- Spherical CLs with spherical equivalent power
- Spherical CLs with Plano-cylindrical glasses
- Toric CLs (Soft and RGP) or customizable designs
- Rigid Gas Permeable (RGP) CLs
- Piggyback CLs (RGP on top of a soft CL) – preferred to patients who have discomfort due to lens awareness, and here the soft CLs offer a shield/cushion to provide additional visual comfort
- Rose-K lenses
- Semi-scleral and scleral CLs
Non-surgical and Surgical management options
- Orthokeratology
- LASER and other refractive surgery procedures (LASIK, Epi-LASIK, LASEK, PRK, SMILE etc.)
- Methods (techniques) for astigmatic correction at the time of cataract surgery
- Toric Intra Ocular Lens (IOL) implants (1-4 dioptres)
To prescribe or not to prescribe?
Neonates are normally symmetrically hypermetropic with a minimal amount of astigmatism. Literature has shown that the occurrence of astigmatism in childhood naturally declines with the process of emmetropisation. With-the-rule astigmatism is observed most commonly in young adults and with increasing age the axis shifts from a predominance of with-the-rule astigmatism to against-the-rule astigmatism caused by the alterations in corneal curvature. The reasons behind this change are usually attributed to the alterations in the position and tension (tightness) of the eyelid, biomechanical properties of the cornea, extraocular muscles, etc. along with the genetic factors.
There are numerous guidelines that have been published to help vision practitioners for prescribing astigmatism. The visual system may not be very sensitive to the blur induced by astigmatism in the first of life, but there onwards uncorrected astigmatic error (specifically oblique) can induce retinal blur during the early developmental phase leading to a condition called meridional amblyopia (MA), or best-corrected visual defects that are greater for or are present only for, specific stimulus orientations. It is advised to correct astigmatism of 1.00 DC or more as early as two years to optimize the acuity development, we are herewith providing a brief guideline for prescribing optical correction in cases of astigmatism (Table 1). In current clinical practice, astigmatism-related amblyopia in the absence of anisometropia, strabismus, and other ocular abnormalities are treated by providing the individual with clear visual input through optical correction of astigmatism (Reading recommendation: reference number 4).
Table 1: Brief prescribing guidelines in cases of astigmatism
|
Prescribe partial (50%) cylindrical correction |
|
Prescribe full cylindrical correction, in cases of previously uncorrected astigmatism, begin with reduced amount for better adaptation |
|
Prescribe 75% cylindrical correction, after an age of 2 years shift to full correction |
|
> 0.75 DC with or without visual symptoms and even lesser amount if symptomatic should be prescribed with full correction |
Astigmatism in young adults can be treated using non-invasive methods while in older patients with cataractous lenses, the management of astigmatism can even be combined with cataract extraction. In patients implanted with conventional IOLs (monofocal), uncorrected astigmatism might have an impact on the distance and near vision. Studies have suggested that a minimal under correction of myopic astigmatism (<1.00 D) can result in a partial restoration of near acuity with a proportional loss of distance acuity. Whereas uncorrected hyperopic astigmatism results in the decline of both distance and near acuities of pseudophakic eyes (Reading recommendation: reference number 7).
Toric IOLs are one of the recent choices to correct significant pre-operative astigmatism of more than 1.00 D. The standard Toric are available in powers of 1.5 D to 6.0 D and are intended to correct regular corneal astigmatism (ranging from 0.75 D to 4.75 D). There are customized toric IOLs available to correct higher cylinder powers. The visual outcomes post implantation of toric IOLs are decided by several factors including the preoperative case selection, investigations, and accurate intraoperative alignment and postoperative care.
Twenty Clinical Pearls in Astigmatic Care
- Patients might have different tolerance levels to visual blur, hence decide on the astigmatic power prescription depending on the patient’s sensitivity as certain patients might be sensitive to even a 0.25 D of change
- Always confirm the power and axis of the cylinder with the subjective refinement techniques during refraction and objective techniques using a keratometer
- Consider the refinement of the spherical power whenever changes are made to the cylindrical power
- If the patient has a high magnitude of astigmatism and first-time wearer of glasses or astigmatism detected at a later age of 35 years or more, it is advisable to give a lesser amount of cylinder or partial correction at first and progressively increase the strength overtime period (~0.50 D steps in ~3 to 4 months)
- Always consider the patient’s age, visual needs, and work environments while prescribing e.g. print size, working distance, duration of use, etc.
- If the patient is in the pre-presbyopic age (35 years or more), and presenting with a complaint of near vision difficulty, always rule out the presence of cylindrical/sphero-cylindrical error for distance as the distance correction will enhance the quality of near vision as well
- In pediatric patients less than 5 years of age (>1.0 D anisometropic astigmatism and >2.5 D isometropic astigmatism) the primary concern is to prevent amblyopia, hence the amount of correction has to be decided according to the age (Table)
- In high refractive errors, low astigmatism corrections can be compensated with spherical equivalentif patients are visually comfortable and don’t appreciate a significant difference
- If there is a presence of astigmatic error >1.5 D, it is advisable to document the Keratometry values to quantify the corneal contribution
- In irregular astigmatism, frequent changes of glasses, and progressive cylindrical power is found, ensure to evaluate the patient in detail for the presence of corneal ectasia
- In a rare situation, some patients might accept different cylindrical power and axis for distance and near vision, then prescribe separate distance and near
- If the patient is already a glass wearer, don’t make a change to the astigmatic power or axis unless needed/mandatory
- Advising the right type of lens depends on the degree of astigmatism, generally, the higher the magnitude, the thinner should be the lens of choice (e.g. Trivex, high-index, etc.)
- Anti-reflection coating can be advised to reduce glare off the lens surface, particularly in high-index lenses
- A flatter frame is generally preferred for higher astigmatism powers than wraparound frames
- Along with the conventional design of spectacle, new commercially available approaches can also be recommended to patients depending on their visual demand and the pattern of occupation
- Frame shape can be chosen based on the facial features of the patient for better patient comfort, satisfaction, and compliance
- It might be worthwhile to advise for a spectacle frame change when there is a significant change in prescription, i.e. 1.00 D or more in the sphere, 0.75 D of more in cylinder, or 15° or more in cylindrical axis
- Educate the patients well on the refractive condition and adaptation levels, remember children can adapt faster than the adults in most of the cases
- Generally, pseudophakic patients with high astigmatism tend to accept full correction and show a swift adaptation
References:
- Burnett SM. A Theoretical and Practical Treatise on Astigmatism. JH Chambers & Company; 1887.
- Namba H, Sugano A, Murakami T, Utsunomiya H, Nishitsuka K, Ishizawa K, Kayama T, Yamashita H. Age-Related Changes in Astigmatism and Potential Causes. Cornea. 2020 Nov 1;39: S34-8.
- Remón L, Monsoriu JA, Furlan WD. Influence of different types of astigmatism on visual acuity. Journal of optometry. 2017 Jul 1;10(3):141-8.
- Harvey EM. Development and treatment of astigmatism-related amblyopia. Optometry and vision science: official publication of the American Academy of Optometry. 2009 Jun;86(6):634.
- Leat SJ. To prescribe or not to prescribe? Guidelines for spectacle prescribing in infants and children. Clinical and experimental Optometry. 2011 Nov;94(6):514-27.
- Kaur M, Shaikh F, Falera R, Titiyal JS. Optimizing outcomes with toric intraocular lenses. Indian journal of ophthalmology. 2017 Dec;65(12):1301.
- Singh A, Pesala V, Garg P, Bharadwaj SR. Relation between uncorrected astigmatism and visual acuity in pseudophakia. Optom Vis Sci. 2013 Apr;90(4):378-84.