
4.jpg)
Intermittent exotropia (IXT) is the most common type of strabismus in children as well as adults, especially in the Asian and South Asian populations. Owing to the intermittent nature of exotropia there is usually good binocular function and stereoacuity at near fixation Small-angle exotropia is observed in normal neonates which usually disappears by the age of 2-4 months. Most adults will have small exophoria usually less than 10 when fully dissociated.
Epidemiology
Like all forms of strabismus, exotropic deviations can be manifest or latent, and if the former, intermittent or constant. Intermittent exotropia is by far the most common form of manifest XT.
Exodeviations occur about one-third less frequently than esodeviations in North America and Europe and occur more frequently in the Asian population. Intermittent exotropia is more common in females with a ratio of 2:1 (F: M). Intermittent exotropia usually noticed by parents in early childhood (2-5 years).
Clinical features
Intermittent exotropia is usually observed by parents in early childhood or late infancy as an infrequent outward deviation of one eye. They tend to manifest their deviation under conditions of fatigue, illness, daydreaming, or inattentive. Adult patients will often become exotropic after taking sedatives or drinking alcoholics.
Children with IXT may intermittently close the nondominant eye in bright sunlight. This light sensitivity, called “photalgia,” was thought to be due to avoidance of diplopia by auto-occlusion when the eye starts to deviate. Hence also called as “diplopia-phobia”.
Without suppression, older children and adults complain of asthenopia, blurred vision, headaches, diplopia or visual confusion, and reading difficulties— especially after prolonged periods of near work. Patients commonly complain of losing their place while reading and needing to repeatedly start on the same line. Accommodative convergence is rarely used to control exodeviation at a distance so that objects appear smaller and closer leading to micropsia. Usually, patients with intermittent exotropia initially will have normal fusion with excellent stereopsis (40-50 seconds of arc) and amblyopia is rare.
Natural history:
The natural history of intermittent exotropia is not completely understood yet, but spontaneous resolution is rare, and an increase in deviation is noted over the years. The deviation is noted to increase in a phased manner as below,
Phases of exodeviation :
- Exophoria at distance/orthophoria at near. (asymptomatic)
- Intermittent exotropia for distance, orthophoria or exophoria for near. (symptomatic for distance)
- Exotropia at distance, exotropia / intermittent exotropia at near. Suppression scotoma at distance.
- Exotropia at distance as well as near, lack of binocularity.
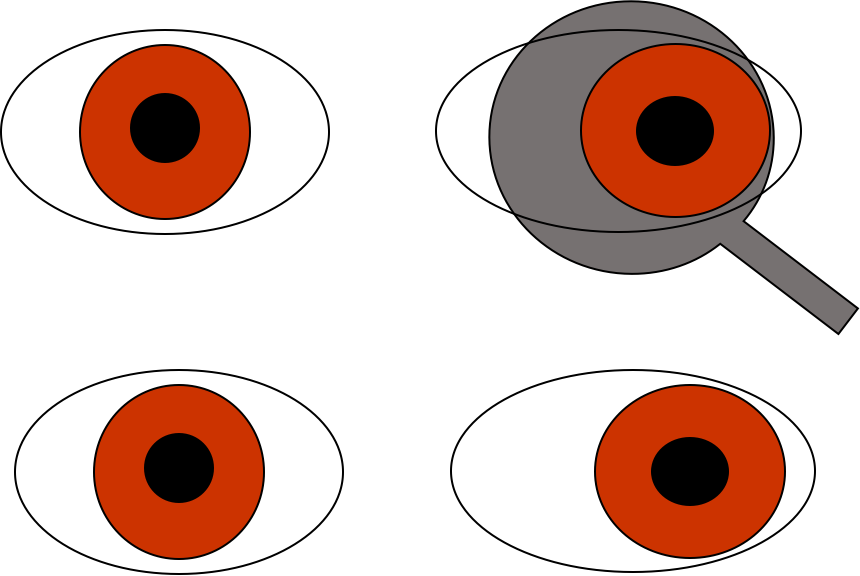
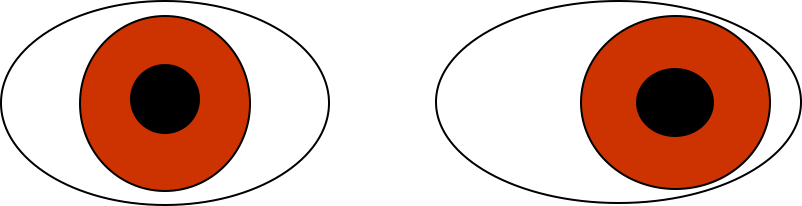
The ability to control the deviation is graded in various ways either qualitatively or quantitatively as follows, ( Fig 1,2,3)
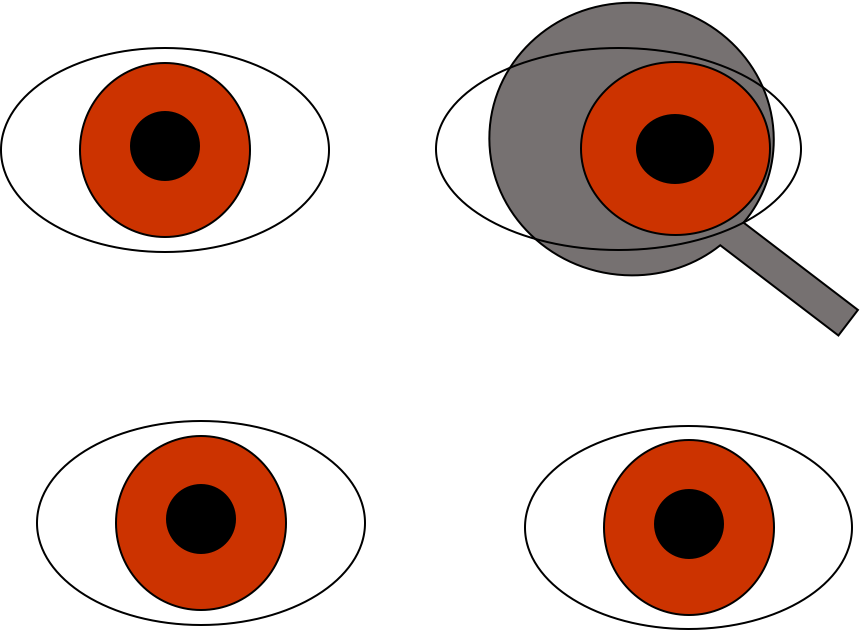
cover and refixes immediately or with a blink or refixation
|
Good control |
Exotropia manifests only after cover testing, and the patient resumes fusion rapidly without blinking or refixating. |
|
Fair control |
Exotropia manifests after fusion is disrupted by cover testing, and the patient resumes fusion only after blinking or refixating. |
|
Poor control |
Exotropia manifests spontaneously and may remain manifest for an extended time |
cover and remains manifest for prolonged time
More objective methods for grading the control include the Newcastle Control Score (NCS grading ) based on home and clinic control and is most commonly used.
|
Newcastle control score |
|
|
Control |
Score |
|
Home control XT or monocular eye occlusion Never > 50% of time fixing at distance <50% of time fixing at distance <50% of time fixing at distance+seen at near. |
0 1 2 3 |
|
Clinical control Near Immediate realignment after dissociation Realignment with aid of blink or refixation Remains manifest after dissociation or prolonged fixation Manifest spontaneously Distance Immediate realignment after dissociation Realignment with aid of blink or refixation Remains manifest after dissociation or prolonged fixation Manifest spontaneously |
0 1 2 3 0 1 2 3 |
|
Total: NCS = home+near+distance |
|
Signs of progression:
1. Increasing frequency of manifest phase squint (loss of fusional control) as noted by the scoring/ grading of control of IXT
2. Increase in the magnitude (size) of deviation.
3. Development of suppression and decreased stereo acuity at distance and near
Classification :
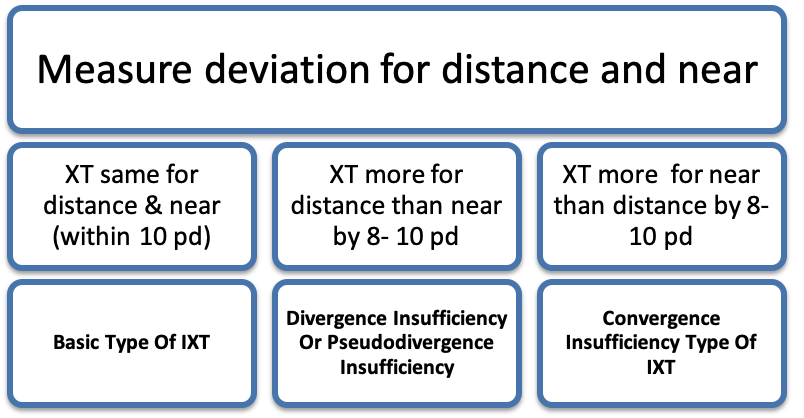
Sensory tests for stereopsis and fusion should be done at the start of the evaluation as visual acuity and alignment tests are dissociating and may adversely affect the assessment. Prism and alternate cover testing should be used to evaluate the exodeviation at fixation distances of 6 m and 33 cm. A far-distance measurement(<6m)(eg, at the end of a long hallway or out a window) is also be a useful measurement in IXT The divergence insufficiency type of IXT can be further divided into true divergence excess or pseudo divergence excess based on patch test and AC/ A ratio.
Patch test: When the exodeviation at distance is larger than the deviation at near fixation by 10Δ or more, one of the eye is patched for 45- 60 min. The near deviation is re-measured after patch test without allowing the binocular fusion. If the near deviation increases and becomes equal to or within 8-10pd distance deviation then it is termed as pseudo divergence excess.
AC/A ratio: If the distance deviation is more than near deviation after patch test then +3.00 D lens test is done to note high AC/A ratio. Near deviation is measured with and without +3.00 D lenses and AC/A ratio noted .
AC/A can also be calculated using the heterophoria method. This is also termed as pseudo divergence excess type of IXT
If the distance deviation remains more than near deviation after patch test and +3.00 D test then its termed as True divergence excess type of IXT
If the near deviation is more than distance deviation by 10 pd, then it is convergence insufficiency type of IXT. This can be further subdivided into true or pseudo convergence insufficiency types. True convergency insufficiency type of IXT can be due to low AC/A ratio or fusional convergence insufficiency.
The most commonly employed classification is summarized below,
|
Burian’s classification |
Kushner’s classification |
|
Divergence excess |
Proximal convergence High AC/A ratio |
|
Simulated divergence excess( based on monocular occlusion) |
Tenacious proximal fusion |
|
Simulated divergence excess (based on +3.00 D lenses) |
High AC/A ratio |
|
Basic |
Basic |
|
Convergence insufficiency |
Low AC/A ratio(accommodative convergence Insufficiency) |
|
Normal AC/A ratio( Fusional convergence Insufficiency) |
|
|
Pseudo-convergence insufficiency (equalizes after monocular occlusion) |
Lateral incomitance
Lateral incomitance is the presence of difference in size of the deviation in primary position and lateral gaze. It is considered significant if there is a reduction of 20% or more of size of angle of deviation in lateral gaze compared to primary position or a difference of 5 to 10 PD.
It can occur primarily or as a result of past surgeries. If significant lateral incomitance is documented, the usual surgical numbers for LR recession should be reduced to avoid overcorrection
Treatment of intermittent exotropia
Non-surgical treatment:
- Correction of refractive errors: as clear retinal image enables better control of exodeviation. Even if hyperopic refractive error is noted, correction is important as they may have some degree of isoametropic amblyopia and hypoaccommodation . And by prescribing the plus lenses, vision and accommodation improve, thus improving convergence and control of the exotropia.
- Over minus lenses : (2-3 D minus over cycloplegic refraction without degrading Visual acuity in each eye) may be used to improve the control as a temporizing measure. Over minus lenses stimulate accommodative convergence and thus control XT . This is useful in younger children with small angle exotropia (5-15PD) or patients where it is preferable to defer surgery for any reason .
- Part-time occlusion therapy: The dominant eye is patched part time to force the non preferred eye to be used, thus providing anti-suppression therapy. In patients with equal ocular preference, alternate eye patching is indicated.
- Orthoptics : Convergence insufficiency type of XT ( fusional convergence insufficiency subtype) responds to convergence therapy . The goal is to increase the fusional convergence amplitudes with exercises. Various exercises employed are ;
- Pencil Push Up exercises
- Brock String exercises
- Cat card exercises
- Prism convergence exercises
- Red filter convergence exercises
Surgical treatment:
Indications for surgery
1. Poor control or deterioration of control of IXT
2. Increase in the angle of deviation
3. Deterioration in stereoacuity
4. Development of suppression
Timing of surgery
Early surgery (<4 years) is not advocated due to the higher incidence of amblyopia with mild postoperative overcorrection. So, surgery is usually planned after 4 years of age.
Choice of surgery
The factors which determine the choice of surgery are:
1. comparative deviation at 33cm,6m, and in the far distance (20 m).
2. AC/A ratio and determining whether the patient has a true or simulated divergence excess.
3. presence or absence of lateral incomitance (change of deviation on lateral versions).
4. if there is A or V Pattern with or without associated inferior oblique or superior oblique overaction.
Surgical Options
|
Basic exotropia (N=D) |
True divergence excess (D |
Convergence insufficiency (N |
|
Bilateral lateral rectus recession |
Bilateral lateral rectus recession |
Bilateral medial rectus resection |
|
Unilateral Recess-Resect |
Augmented lateral rectus recession |
Unilateral Recess-Resect |
A or V patterns if present is corrected with oblique surgeries or vertical shift of recti muscles .Consecutive esotropia of 5 to 10 pd in the immediate post operative period is recommended to achieve long term results
Summary: Intermittent Exotropia is one of the common strabismus seen in our clinic and management depends on the type, control of IXT, and age of the patient in question.
References
- Wright KW Exotropia in Wright KW , Spiegel PH, Thompson LS in Handbook od Pediatric ophthalmology and strabismus.USA : Springer ;2rd edition, 2012. P.266-281.
- Santiago A P, Ing M R, Kushner B J, Rosenbaum A L . Intermittant Exotropia in Rosenbaum A, Santiago A. Clinical strabismus management. Philadelphia: Saunders; 1999. p. 163-175
- Haggerty H, Richardson S, Hrisos S, Strong NP, Clarke MP. The Newcastle Control Score: a new method of grading the
- severity of intermittent distance exotropia. Br J Ophthalmol. 2004;88(2):233–235.
- Pratik Chougule, Ramesh Kekunnaya, Surgical management of intermittent exotropia: Do we have an answer for all?, BMJ open ophthalmology 2019;4: e000243.
- Relationship among clinical factors in childhood intermittent exotropia, Rosanne superstain et al, J AAPOS. 2017 august;21(4):268-273.
- A Randomized trial comparing bilateral lateral rectus recession versus unilateral recess-resect for basic- type intermittent exotropia, Pediatric Eye Study Investigator Group, Ophthalmology. 2019 February; 126(2):305-317. 7.Interventions for intermittent exotropia, Cochrane Systematic Review- intervention|Version published: 31 May 2013