
A 55-year-old female presented to the Cornea clinic with gradually progressive diminution of vision in both eyes for 1 year, which was associated with intermittent photophobia and colored haloes around lights, especially on waking up in the morning. The blurry vision gradually became clearer as the day progressed.
No history of associated pain, watering, redness, itching, or discharge.
Past Ocular History:
No history of ocular trauma or surgery in the past
Past Medical History/ History of Medication:
No significant systemic history could be elicited. Patient was not on any medication. No addictions.
Family History:
No significant family history found
Review of Systems/Systemic Examination
Systemic examination was within normal limits. All vitals were within normal limits.
OCULAR EXAMINATION
Best Corrected Visual Acuity (Snellen)
Right eye (OD): 6/36
Left eye (OS): 6/12
Ocular Motility/AlignmentFull, free, and painless in all gazes
Intraocular Pressure (IOP)
OD: 16 mm of Hg
OS: 16 mm of Hg
PupilsOU Round, regular and reacting to light
Confrontation visual fields: CVF full
Slit-lamp examination:
|
OD |
OS |
|
|
Lids/lashes |
Normal |
Normal |
|
Conjunctiva/sclera |
Normal |
Normal |
|
Cornea |
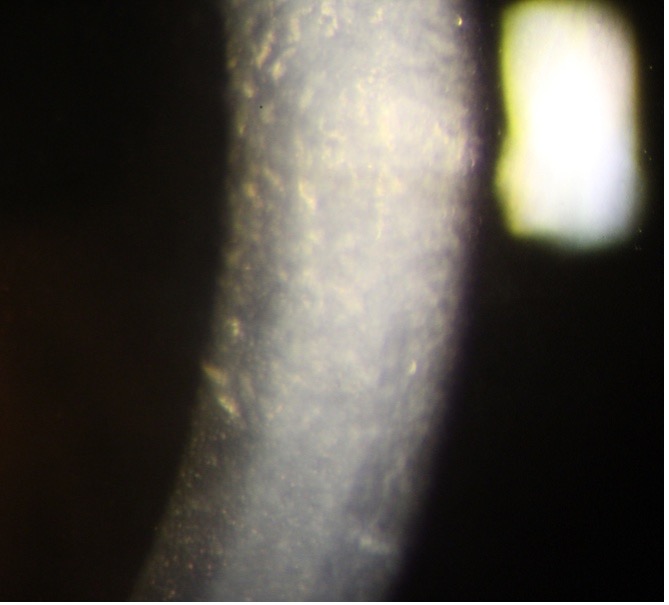
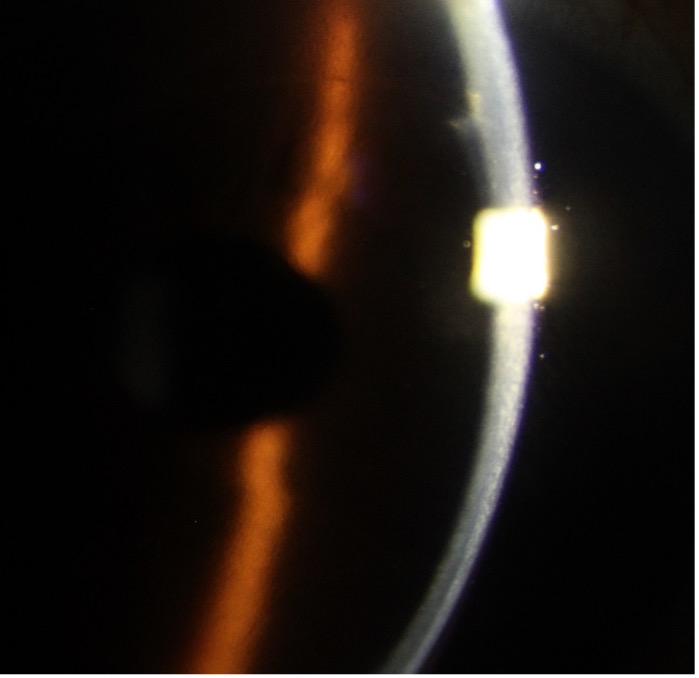
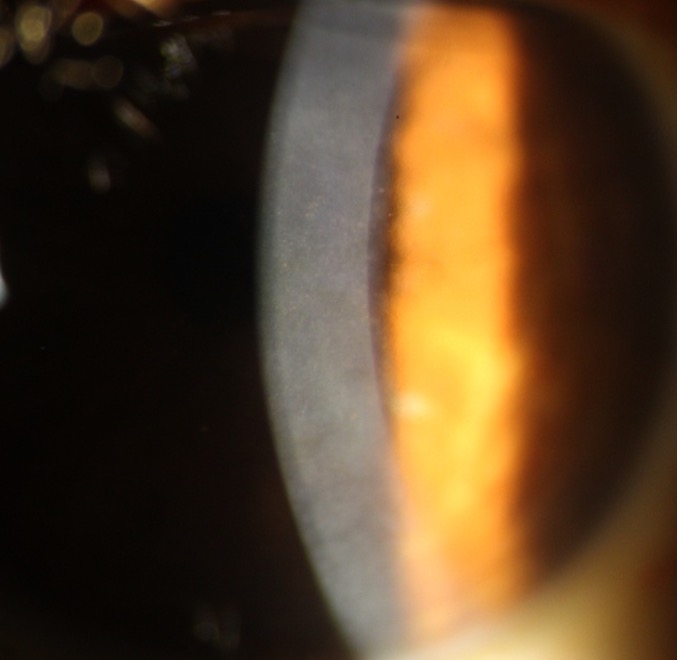
Epithelial, stromal edema, and stromal scarring noted. Numerous dark areas s/o guttae, on the central endothelium as seen by specular reflection, causing Beaten metal-like appearance (Fig. 1A) |
Epithelial and mild stromal edema noted. Numerous guttae on the central endothelium as seen by specular reflection causing Beaten metal-like appearance (Fig. 1B) |
|
Anterior chamber |
Normal in depth, quiet |
Normal in depth, quiet |
|
Iris |
Normal color and pattern |
Normal color and pattern |
|
Lens |
Nuclear sclerosis grade II |
Early nuclear sclerosis |
Dilated Fundus Examination:
|
OD |
OS |
|
|
Vitreous |
Clear |
Clear |
|
Disc |
0.4:1, NRR healthy |
0.4:1, NRR healthy |
|
Macula |
FR shining |
FR shining |
|
Vessels |
Normal in calibre, AV ratio maintained |
Normal in calibre, AV ratio maintained |
|
Periphery |
Normal |
Normal |
causing Beaten metal appearance, along with mild
subepithelial scarring
also called guttae
ANCILLARY INVESTIGATIONS:
Specular microscopic examination:
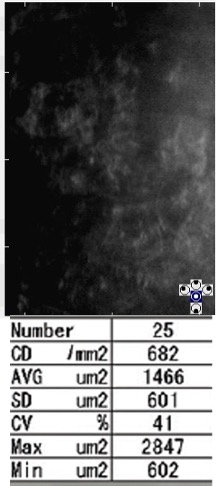
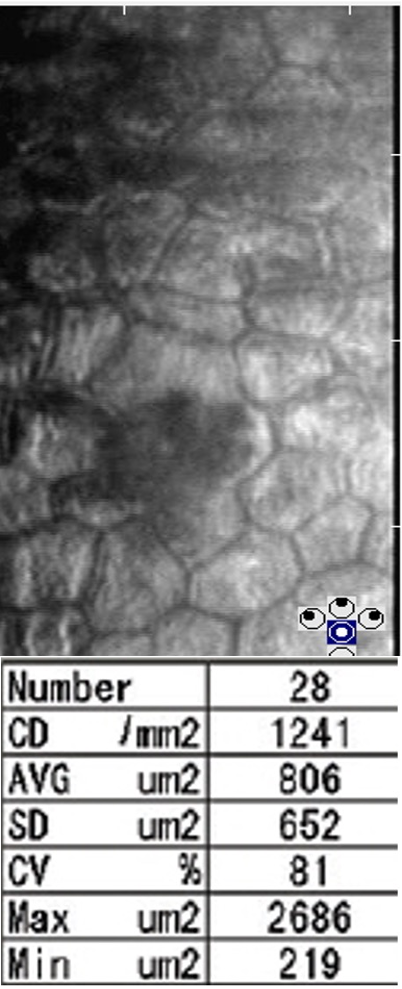
Specular microscopy of the right cornea (Fig 2A) demonstrated large numbers of dark areas. Between the dark areas, the endothelial cells appeared hyper-reflective and their boundaries could not be identified. In the left cornea (Fig 2B) there were fewer dark areas and the boundaries of endothelial cells could be identified. However, the endothelial cells were increased in size and in different shapes showing polymegathism and pleomorphism.
Ultrasound pachymetry:
Pachymetry showed the central corneal thickness of OD 718 μm and 589 μm in OS.
Differential Diagnosis:
- Fuch’s endothelial dystrophy
- Herpetic stromal keratitis
- Pseudophakic bullous keratopathy
- Iridocorneal endothelial (ICE) dystrophy
- Congenital hereditary endothelial dystrophy
- Congenital stromal dystrophy
- Posterior Polymorphic Membrane Dystrophy
Diagnosis:
Based on the typical clinical picture and specular microscopic findings, a diagnosis of OU Fuch’s endothelial corneal dystrophy (FECD) with nuclear sclerosis was made
Clinical Course of the condition:
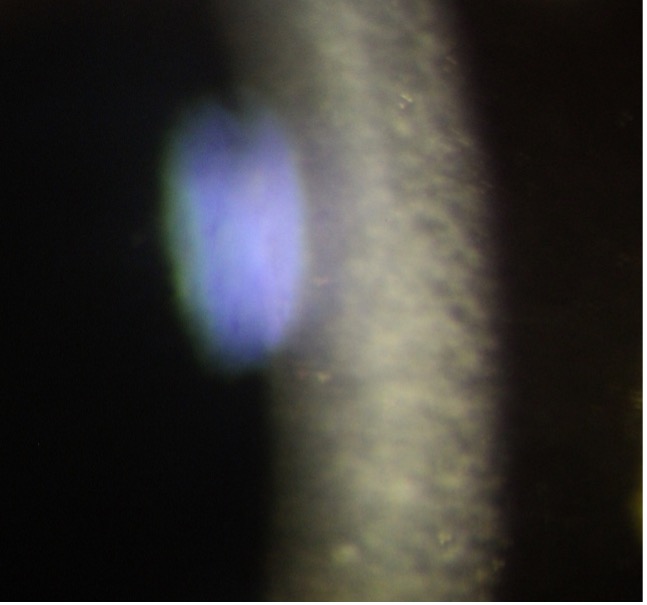
Taking into account the symptoms, BCVA, clinical picture, and specular microscopy findings, the patient was advised OD Descemet stripping endothelial keratoplasty (DSEK) with cataract surgery and IOL implantation. OS being the better eye was managed medically with local dehydrating agents (6% NaCl ointment 3 times a day). At 6 months follow-up visit, the patient was doing well. In OD, the graft was clear (Fig 3A), the BCVA was 6/9 with -1.50D/ -2.00D @ 30. In the left eye, the cornea was clear with minimal edema (Fig 3B), the cataract had progressed to nuclear sclerosis grade II and the BCVA was 6/12 with -1.25D.
and the patient was doing well
corneal edema was reduced and patient
was having minimal symptoms
DISCUSSION
Epidemiology
FECD is the most common posterior corneal dystrophy, characterized by slowly progressive dysfunction of the corneal endothelium leading to corneal oedema and reduced vision, which, if untreated eventually results in corneal blindness. Incidence is estimated at up to 4% in adult population in the world. The disease is less prevalent in individuals of brown and black races.
FECD is more common in females; the reported preponderance ranges from 2.5:1 to 3:1. FECD can be early onset, presenting in the second or third decade, and, late-onset, presenting in the sixth or seventh decade.
Etiology
Although the disease has a proven autosomal dominant inheritance pattern, sporadic cases are the most common. The ICD3 classification 2015 has categorized FCED as:
Category 1 – Gene has been identified and a specific mutation is known. Includes Early-onset FECD – mutations in COL8A2
Category 2 – Identified chromosomal loci, but the genes have not been mapped – Includes Familial FECD. Fuchs corneal dystrophy loci (FCD) 1, 2, 3, 4 have been mapped to chromosomes 13, 18, 5, 9 respectively
Category 3 – Well-defined corneal dystrophy without known chromosomal locus – Includes most of the sporadic cases
Pathophysiology
Endothelial cells are responsible for maintaining a state of stromal dehydration against the influx of aqueous from the leaky barriers between the cells. The endothelial cells contain a number of ion pumps to maintain the fluid influx and to pump out bicarbonate ions out of the stroma and into the aqueous.
In FECD there is a generalized downregulation of antioxidants and oxidative stress-related genes. The resulting oxidative stress leads to nuclear and mitochondrial DNA damage, and eventually, apoptosis.
The stressed endothelial cells deposit banded collagen fibrils and extracellular matrix in the DM, which manifests as guttae. The DM becomes thickened. The total number of endothelial cells is reduced due to apoptosis. The remaining cells become larger to compensate (polymegathism) and the hexagonality is reduced (pleomorphism). The guttae become confluent as the disease progresses.
The continued loss of endothelial cells leads to low pumping capacity and the endothelium eventually becomes incapable of maintaining corneal deturgescence, leading to stromal edema, epithelial edema, and bullae. In the advanced stage of the disease, long-standing edema and oxidative stress leads to subepithelial and stromal fibrosis and eventually opacification.
The Krachmer grading scale is sometimes used to subjectively evaluate disease progression
Grade 0 (G0) – no guttae
Grade 1 (G1) 0–12 central guttae
Grade 2 (G2) greater than 12 central nonconfluent guttae
Grade 3 (G3) 1–2 mm of confluent central guttae
Grade 4 (G4) 2–5 mm of confluent central guttae
Grade 5 (G5) greater than 5 mm of confluent central guttae or G4 with stromal or epithelial edema
Clinical Features
Symptoms:
- None in the very early stages
- Blurred vision more on awakening because of overnight corneal edema
- Glare and photophobia because of corneal edema
- Foreign body sensation due to bullae formation
- Severe pain and watering due to denuded epithelium from ruptured epithelial bullae
- Loss of vision in late stages
Signs:
- Reduced corneal sensations
- Reduced contrast sensitivity
- Excrescences on endothelium (guttata) produce a ‘beaten metal’ like appearance in the central cornea
- Pigment dusting on endothelium
- Central microcystic epithelial edema
- Stromal edema and thickening
- Thickened Descemet’s membrane and folds
- Bullous keratopathy
- Subepithelial scarring and fibrosis
The stages of Fuchs Dystrophy:
|
Stage |
Description |
|
I |
Central, but nonconfluent corneal guttae |
|
II |
Corneal guttae coalesce together to form dark lakes |
|
III |
Epithelial and stromal edema and/or bullae |
|
IV |
Vascularized and opaque cornea |
Ancillary Investigation
Slit-lamp examination:
Specular reflection using the slit lamp biomicroscope is one of the most important tools for screening patients with compromised endothelium. Specular reflections are normal light reflexes bouncing off the posterior corneal surface. It is seen by setting the slit beam arm at about 60° from the viewing arm. The beam width should be kept at about 1mm or less. The guttae are visible as dark gaps in the regular endothelial mosaic.
Another way of assessing the endothelial defects is retroillumination on slit-lamp examination. The cornea is assessed against the fundal red glow through dilated pupil. The arms are kept at a very small angle to each other. Retroillumination photography is used to document the pattern and progression of guttae over time.
Specular microscopy:
Specular microscopy shows a magnified view of the corneal endothelium. Both qualitative and quantitative evaluation of the endothelium is done, with cell density as a quantitative measure and CV and 6A showing pleomorphism and polymegathism for qualitative assessment. Guttae appear as dark round bodies with central hyperreflective areas. In FECD, numerous guttae appear, CD decreases, CV increases, and 6A progresses over time.
FECD can be divided into 5 stages based on size, shape and confluence of guttae as seen on specular microscopy.
|
Stage 1 |
Early guttae which are smaller than size of endothelial cell |
|
Stage 2 |
Larger excrescence about the size of endothelial cell, surrounded by normal endothelial cells forming a rosette pattern |
|
Stage 3 |
Large excrescence surrounded by abnormal pleomorphic endothelial cells. The excrescences can be rough or smooth at this stage |
|
Stage 4 |
The large excrescences are coalesced at this stage. Other endothelial cells show polymegathism |
|
Stage 5 |
No recognisable cell boundaries, the cells are dark with bright hyperreflective borders. |
The specular microscopy is unrecordable in advanced FECD with severe corneal edema and has limited value in these cases.
Serial pachymetry
Pachymetry is the measurement of the central corneal thickness, which is increased in moderate to severe FECD owing to corneal edema. It helps in assessing the progression of disease as the cornea edema increases secondary to endothelial cell decompensation. It also helps in decision regarding cataract surgery in FECD along with specular microscopy.
Traditionally, the CD less than 1000/mm2, and pachy values of more than 640µm are taken as cut off values, which can cause corneal decompensation post-cataract surgery.
Confocal microscopy
Confocal microscopy is a particularly useful tool for patients with advanced FECD, where specular microscopy is not possible. This technique focuses the light source and the image on the same focal plane, which allows real-time, in vivo assessment of all layers of cornea. The guttae are visible as hyporeflective, dark bodies about 20-400µm in size with central hyperreflective white reflex about 50-10µm within the surrounding endothelial cell mosaic.
The advantage of confocal microscopy is that it allows the assessment of abnormalities in all corneal layers. In FECD, the changes observed are, epithelial bullae and cysts, subepithelial and anterior stromal scarring, thickened DM and the endothelial changes like pleomorphism, polymegathism and guttae.
Anterior Segment Optical Coherence Tomography (ASOCT):
ASOCT is recently being used for monitoring disease progression in FECD and for assessment of severity. The severity is predicted by corneal central-to-peripheral thickness ratio (CPTR). The CPTR at 4 mm from the centre ratio is higher in advanced than in mild to moderate disease, which again is higher than normal corneas. ASOCT can measure both the central and the peripheral corneal thickness and thus can be a useful test for FECD.
Treatment
1. Medical treatment
- Dehydrating agents- Hypertonic saline drops and ointment
- Antiglaucoma medication- to lower the IOP if it is more than 22 mmHg
2. Palliative treatment for ruptured bullae- Anterior stromal puncture, Bandage contact lenses, cycloplegics
In very low visual potential cases, surgical treatment for ruptured bullae is indicated - Excimer laser phototherapeutic keratectomy, Amniotic membrane grafting, Conjunctival flap
3. Surgical treatment
- DSAEK/DSEK – The donor graft consists of endothelium, DM and a layer of stroma. A variant, ultrathin DSAEK has a minimal stromal layer and graft is just 100 μm thick.
- DMEK- The donor graft consists of the endothelial layer and the DM.
- PK
Surgery is indicated in cases of refractory corneal edema, subepithelial fibrosis, stromal fibrosis and decompensated cornea.
The endothelial keratoplasties are preferred over full-thickness penetrating keratoplasties wherever possible in view of excellent visual prognosis, fewer chances of rejection, and shorter course of post-operative steroids.
Full-thickness penetrating keratoplasty is indicated in advanced disease with moderate to severe fibrosis and opaque cornea.
Cataract surgery in FECD:
Conventionally cataract surgery without keratoplasty is not advised in corneas with CD less than 1000cells/mm2 and pachy values of more than 640µm as these are taken as cut-off beyond which cornea decompensates. In mild to moderate cases, cataract surgery can be done alone with due precautions to protect the endothelium from injury. In such cases, a Dispersive type OVD is used to coat the endothelium throughout the surgery. In severe cases, it is preferable to combine cataract surgery with keratoplasty to reduce further damage to the endothelium.
4. Newer modalities
- Topical ROCK inhibitors
The use of a selective ROCK inhibitor, Y-27632, enhances endothelial cell proliferation, promoted cell adhesion to a substrate, and suppress apoptosis. Currently, two drugs, ripasudil and netarsudil are available in India.
- DWEK or primary Descemetorhexis
Also referred to as Descemet's Stripping Only (DSO), DWEK is a newer surgical modality for some patients with Fuchs'. Patients with localized central guttae with healthy peripheral endothelium are candidates for this. A 4mm central disc of cells is stripped without placing any graft. The rationale being, the healthy endothelial cells from periphery will migrate centrally, covering the defect, and providing good quality vision. The procedure is aided by prescribing a rho kinase inhibitor (ROCK) eye drop QID postoperatively.
- Cultured corneal endothelial cells (CEC) transplantation
In this, cultured endothelial cells are transplanted as a sheet or by injection of a cell suspension into the anterior chamber. This is still in the trial phase.
Summary
Fuch’s Corneal Endothelial Dystrophy (FCED) |
|
|
Etiology:
|
Signs:
|
|
Symptoms:
|
Differentials:
|
|
Investigations:
|
Treatment:
|
References:
- Vedana G, Villarreal Jr. G, Jun A. Fuchs endothelial corneal dystrophy: current perspectives.Clin Ophthalmol. 2016;10:321-330
- Eghrari AO, Gottsch JD. Fuchs' corneal dystrophy.Expert Rev Ophthalmol. 2010;5(2):147-159. doi:10.1586/eop.10.8
- Elhalis H, Azizi B, Jurkunas UV. Fuchs endothelial corneal dystrophy. Ocul Surf. 2010 Oct;8(4):173-84. doi: 10.1016/s1542-0124(12)70232-x. PMID: 20964980; PMCID: PMC3061348.
- Zhang J, Patel DV. The pathophysiology of Fuchs' endothelial dystrophy--a review of molecular and cellular insights. Exp Eye Res. 2015 Jan;130:97-105. doi: 10.1016/j.exer.2014.10.023. Epub 2014 Nov 1. PMID: 25446318.
- Nielsen E, Nielsen K, Ivarsen A, Greenhill NS, Davis PF, Hjortdal J. Fuchs Endothelial Corneal Dystrophy: A Systematic Immunofluorescence Study of Collagen Type VIII Suggests Heterogeneous Pathophysiology. Cornea. 2016 Jun;35(6):872-7. doi: 10.1097/ICO.0000000000000848. PMID: 27078008.
- Nanda GG, Alone DP. REVIEW: Current understanding of the pathogenesis of Fuchs' endothelial corneal dystrophy.Mol Vis. 2019;25:295-310. Published 2019 Jun 5.
- Chaurasia S, Vanathi M. Specular microscopy in clinical practice. Indian J Ophthalmol 2021;69:517-24
- Benetz, Beth Ann CRA, FOPS; Lass, Jonathan H. MD Specular Microscopy, Cornea: June 2018 - Volume 37 - Issue - p S7-S8
- doi: 10.1097/ICO.0000000000001642
- McCarey BE, Edelhauser HF, Lynn MJ. Review of corneal endothelial specular microscopy for FDA clinical trials of refractive procedures, surgical devices, and new intraocular drugs and solutions.Cornea. 2008;27(1):1-16. doi:10.1097/ICO.0b013e31815892da
- Nagarsheth M, Singh A, Schmotzer B, et al. Relationship Between Fuchs Endothelial Corneal Dystrophy Severity and Glaucoma and/or Ocular Hypertension.Arch Ophthalmol. 2012;130(11):1384-1388. doi:10.1001/archophthalmol.2012.1969
- Naoki Okumura, Shigeru Kinoshita, Noriko Koizumi,"Application of Rho Kinase Inhibitors for the Treatment of Corneal Endothelial Diseases",Journal of Ophthalmology,vol.2017,Article ID2646904,8pages,2017.https://doi.org/10.1155/2017/2646904
- Moshirfar M, Parker L, Birdsong OC, et al. Use of Rho kinase Inhibitors in Ophthalmology: A Review of the Literature.Med Hypothesis Discov Innov Ophthalmol. 2018;7(3):101-111.