
A 53-year-old female presented to the emergency with chief complaints of drooping of the left eyelid for 3 days and sudden loss of vision in the left eye for 2 days.
History of Present Illness:
The patient was recovering from COVID-19 infection prior to presentation when she noticed a sudden, rapidly progressive drooping of the left eyelid over 3 days duration. It was associated with the limitation of extraocular movements. Loss of vision was sudden, associated with pain, and fullness around the eye. She had a history of the left-sided nasal block along with altered sensation over the left cheek for 1 day. She had no history of fever, toothache, trauma, hospitalization, or intake of steroids.
Past Ocular History:
Underwent cataract surgery in both eyes 2 years back.
Past Medical History/ History of Medication:
She tested COVID positive 2 weeks prior to the current presentation and was advised home quarantined. CT chest score was 3, and spO2 was maintained throughout the quarantine period. She was a known diabetic on Human Insulin injection.
Family History:
Not significant
Review of Systems/Systemic Examination:
Within normal limits and all vitals were normal.
OCULAR EXAMINATION
- Best Corrected Visual Acuity (Snellen):
OD: 6/9
OS: No perception of light (checked in a dark room)
- Hirshberg corneal reflex - Orthophoric
- Face: Left-sided cheek fullness,Palate, teeth: normal
- Extraocular motility:
OD: -4 depression, rest full and free
OS: -4 in all gaze
- Intraocular Pressure (IOP):
OD -14 mm Hg,OS - 12 mmHg
- Pupils:
OD – normal in size reacting to light, inverse RAPD present
OS – mid-dilated, fixed, not reacting to light
- Confrontation visual fields:
OD- within normal limits, OS-deferred
External examination:
|
OD |
OS |
|
|
Lids/Lashes |
Normal |
Complete ptosis Upper lid mild edema |
|
Brow Ptosis |
Absent |
Absent |
|
Frontalis Overaction |
Present |
Absent |
|
Margin reflex distance (MRD) 1 |
3 |
-6 |
|
MRD 2 |
6 |
6 |
|
LPS Action |
14 |
0 |
|
Margin crease distance |
8 |
Absent |
|
Bells |
Good |
Poor |
|
Orbital examination |
Normal |
No palpable orbital mass |
|
Hertels (95) |
15 |
16 |
|
Retrobulbar resistance |
Normal |
Borderline raised |
Slit-lamp examination:
|
Conjunctiva |
Normal |
Grade 1 chemosis |
|
Cornea |
Normal |
Normal |
|
Iris |
Normal |
Normal |
|
AC |
VH 4, Quiet |
VH4, Quiet |
|
Lens |
Pseudophakia |
Pseudophakia |
Dilated Fundus examination
|
Vitreous |
Normal |
Normal |
|
Disc |
Normal |
Pallor |
|
Macula |
Normal |
Cherry red spot |
|
Vessels |
Normal |
Normal |
|
Rena |
Normal |
Pale retina |
|
Periphery |
Normal |
Normal |

Ancillary Investigations:
- Magnetic Resonance Imaging orbit and brain (with gadolinium contrast)
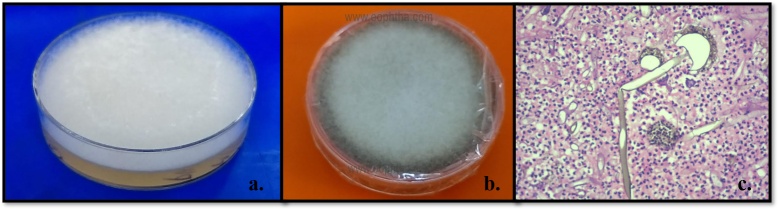
- Diagnostic nasal endoscopic evaluation: Revealed inflamed and edematous nasal mucosa. Necrotic middle turbinate with eschar. Biopsy from the nasal specimen confirmed the presence of aseptate fungi on the KOH mount. Mucor was seen growing on Sabourds dextrose agar medium on day 3.

Clinical Course of the condition:
The patient underwent an immediate left-sided endoscopic nasal debridement and orbital debridement. She received peribulbar amphotericin injection 3.5 mg/ml (1 cc) into the medial orbit daily for 3 days post-op along with intravenous deoxycholate amphotericin 5mg/kg daily over 6 hours duration and was started on oral posaconazole 300mg twice a day. However, the patient developed further cheek numbness, worsening of facial swelling, and persistent left-sided headache. On dental evaluation, the patient had tenderness along with the incisors. Posterior to the incisors, necrosis of the palatal mucosa with eschar was seen.
A repeat urgent MRI of the brain and orbit contrast revealed loss of contrast enhancement in extraocular muscles suggestive of ischemic necrosis with worsening of the inflammation within the left orbit. Sphenoid sinusitis was present. Frontal and parietal lobe infarcts were seen. Involvement of the left infratemporal fossa, temporalis muscle, and left palate was noted.
The patient was taken up for an urgent left-sided extended radical exenteration, maxillectomy, endoscopic nasal, and left sphenoid sinus debridement. The involved left half of the palate was also removed. Postoperatively patient improved and is receiving intravenous Liposomal Amphotericin B 10mg /ml along with oral Posaconazole 300 mg twice a day.
Differential Diagnosis:
- Bacterial orbital cellulitis
- Cavernous sinus thrombosis
- Orbital apex syndrome
Final diagnosis:
Post COVID-19 Left-sided Rhino-orbital-cerebral mucormycosis (ROCM) with central retinal artery occlusion and cavernous sinus thrombosis.
DISCUSSION:
Mucormycosis, also previously called zygomycosis, is caused by a group of fungi called Mucorales. This includes mainly theRhizopusspecies,Mucor,Cunninghamella,Apophysomyces,Lichtheimia(formerlyknown as Absidia),Saksenaea,Rhizomucor, and other species. Associated secondary fungal infections like mucormycosis have been observed amongst patients with COVID -19 infection. A sudden surge in the number of cases has been recorded in sync with the second wave of COVID-19 in India. Rhino-orbital-cerebral mucormycosis (RCOM) is aggressive, associated with high morbidity and mortality, and requires urgent medical and surgical intervention.
Epidemiology:
Mucormycetes are molds that dwell throughout the environment, in the soil, plants, air, and even harbor within the nasal cavity. Humans are exposed to these molds on daily basis but do not get infected as the fungus has low virulence. The incidence of mucormycosis is higher amongst the immunocompromised group. Diabetes mellitus, malignancy, post-transplantation, patients on long-term steroids or immunosuppressants, and neutropenia are risk factors for mucormycosis. Approximately 60-80% of cases have been reported in diabetics with ketoacidosis, till of late.
The secondary contamination of the medical supplies, oxygen tubing, long duration of ICU stay, mechanical ventilation, pre-existing diabetes mellitus, injudicious use of intravenous steroids, and tocilizumab to reduce inflammation, has increased the risk of mucormycosis amongst patients recovering from COVID 19.
Etiopathogenesis:
- Impaired phagocyte function secondary to neutropenia or higher concentration of serum corticosteroids.
- Serum-rich iron, acidified pH, increased blood glucose levels have been attributed to facilitating the proliferation of the fungus.
- Inhalation of fungal spores or conidia is the most common mode of spread. Traumatic inoculation into the nasal mucosa, skin, or ingestion of spores has also been described to cause mucormycosis.
- These spores directly invade the blood vessels and induce an inflammatory reaction inciting a thrombo-embolic phenomenon that causes tissue infarction, ischemia, necrosis, and bone destruction.
- Iron in the blood stimulates its growth, and deferoxamine acts as a siderophore that delivers iron to the fungi.
- The classical blackening of the tissues or eschar seen in mucormycosis is secondary to ischemic necrosis.
- The angio-invasive nature of the disease and the thrombo-embolic phenomenon can cause vision-threatening complications like central retinal arterial occlusion and cavernous sinus thrombosis.
- Rhino-orbital-cerebral mucormycosis (ROCM) usually originates from the paranasal sinuses and invades into the orbit via the thin lamina papyracea or the inferior orbital fissure. Further on, it may extend posteriorly to involve the orbital apex, superior orbital fissure, the cavernous sinus (can involve V1, V2 affecting corneal and facial sensation), and the brain parenchyma. It can also involve the infratemporal fossa, the cheek, palate, and teeth.
Acute lesions:
- Hemorrhagic infarction
- Coagulation necrosis
- Angioinvasion infiltration by neutrophils (in non-neutropenic hosts)
- Perineural invasion
Chronic lesions:
- Pyogranulomatous inflammation
- Giant cells
Clinical Features:
- Varies based on the extent of involvement.
- Duration of symptoms may be as early as within 3-7 days of being detected with COVID-19.
Rhino-facial |
|
|
Symptoms |
Signs |
|
|
Orbital |
|
|
Symptoms |
Signs |
|
|
Fundus Involvement:
- Normal
- Cotton wool spots
- Congested tortuous retinal blood vessels
- Optic disc edema/ pallor
- Central retinal vein occlusion
- Central retinal artery occlusion
- Choroidal folds
Cerebral |
|
|
Symptoms |
Signs |
|
|
Ancillary Investigations:
Magnetic resonance imaging (MRI brain, orbit and paranasal sinuses) with contrast – is the imaging of choice and is superior compared to Computed Tomography (CT) scan.
- Better delineation of soft tissue changes
- Helps differentiate between normal and necrotic tissues
- Early detection of cavernous sinus thrombosis and orbital ischemic changes, hence aids in the planning of the surgical intervention.
CT scan can be done when MRI is not available or contraindicated.
Nasal and paranasal sinus |
|
|
Early |
Low signal, T2 hypo-intense soft tissue Commonly seen in the ethmoid, sphenoid sinus Altered, patchy contrast enhancement Nasal mucosal thickening |
|
Black turbinate sign |
Ischemic necrosis and non-enhancement of the turbinates |
|
Advanced |
The fluid level in the sinus Complete opacification of the sinuses Pan sinusitis |
Orbit |
|
|
Early |
Thickening of the extraocular muscles; commonly medial rectus or inferior rectus Fat stranding Optic nerve thickening or peri-optic fat stranding |
|
Advanced |
Orbital lesion – hypointense in T2 weighted imaging. Patchy enhancement of the lesion, orbital fat around the orbital apex, superior and inferior orbital fissure. Bony erosion Perineuritis Reduced or loss of contrast enhancement in extraocular muscles suggestive of necrosis Diffusion-weighted Imaging – for optic nerve – suggestive of ischemia |
Cerebral |
|
|
Filling defects and non-enhancement of the cavernous sinus Infratemporal fossa- necrotic non enhancing soft tissue Brain abscess |
|
Nasal endoscopic evaluation
- Assess the nasal cavity
- Looks for nasal mucosal edema, ulceration, necrosis, eschar
- The preferred site to take an initial biopsy to confirm the diagnosis under topical/ local anesthesia
Investigations
- Complete blood count – rule out neutropenia
- Serum electrolytes and blood glucose – look for ketoacidosis
- Liver function test
- Renal function test
- Ig M and Ig G antibodies – COVID
- Primary biopsy to confirm the diagnosis
Mucor may have a patchy invasion – may require repeat biopsy if there is further progression of clinical disease.
Microbiology |
|
|
KOH mount (quick, 90% sensitivity) |
|
Fungal culture |
|
|
- Rapid growth - Initial 24-48 hours: fluffy white, - >72 hours: gray or brown cotton candy-like colonies. - Coarse and dotted hyphae with brown or black sporangia |
|
|
Histopathology |
|
|
Fungal granulomas Angioinvasion Perineural spread Tissue infarction Necrosis Inflammation Fungal filaments |
|
Confirms the presence of broad, aseptate , branched hyphae |
|
|
|
|
Treatment:
COVID-19 associated mucormycosis is highly fatal and should be treated as an emergency. It needs a multidisciplinary approach. The team should involve an ENT surgeon, neurosurgeon, oculoplastic surgeon, maxillofacial surgeon, and an infectious disease specialist.
Principles of management:
- Aggressive debridement to reduce the fungal load and for better penetration of systemic antifungals
- The strict control of diabetes mellitus
- Close monitoring to look for clinical progression or resolution of the disease
Surgical:
- Early and aggressive debridement of the necrotic tissues and sinus must be done to decrease the fungal burden.
- Debridement of tissues until bleeding occurs is a good indicator of the extent of surgical resection.
- Repeated surgical debridement may be necessary in many cases.
- If the orbit is involved, depending on the severity and involvement
- Extensive orbital tissue debridement
- Exenteration (advanced orbital involvement, involvement of orbital apex)
Local therapy
- Retrobulbar injection deoxycholate amphotericin B (1ml of 3.5 mg/dl)
- Amphotericin irrigation (1-2.5 mg/dl)
- Can cause further inflammation and
Medical Management
Amphotericin B was the first antifungal to be discovered in 1953 and is obtained from Streptomyces Nodus. It is the first-line medical treatment for mucormycosis and should be initiated as soon as the diagnosis is suspected. It acts by destroying the fungal cell wall.
Commercially available forms are :
- Conventional Amphotericin-B
- Amphotericin-B Colloidal Dispersion
- Liposomal Amphotericin-B
- Amphotericin-B Lipid complex
Liposomal amphotericin B has a higher plasma concentration and is safer in terms of therapeutic efficacy and safety compared to the other forms. It crosses the blood brain barrier and hence, is very effective for cerebral mucormycosis.
Dose: 5-10 mg/kg for 4 weeks
Induction dose for 2 weeks, and then add an oral second line of drugs like poscaconzole, Isavuconazole.
Drug-related Adverse Effects:
|
|
|
Second-line drugs:
Posaconazoleis a triazole that inhibits the growth of the fungus and is a promising adjunctive drug for the treatment of mucormycosis.It is advocated as a first-line drug in patients with pre-existing renal compromise.
Dose: Posaconazole 300mg i.v or oral twice a day (day 1), and then 300mg once a day
Isavuconazoleis a broad-spectrum antifungal with a good safety profile.
Dose: intravenous 200mg i.v or oral thrice a day (day 1,2) 200mg i.v or oral from day 3
Prevention
- Strict monitoring and control of diabetes mellitus
- Judicious and supervised use of systemic steroids and tocilizumab in patients infected with COVID19
- Monitor for early symptoms or signs of mucormycosis even after recovery from COVID
- Maintain good personal hygiene and wear a barrier mask
- Sterile water for the humidifier and frequent change of the sterilized humidifier and the tubes
Rhino-orbital Mucormycosis |
|
Etiology
|
Signs
|
Symptoms
|
Differentials :
|
Investigations :
|
Treatment:
|
References:
- Riley TT, Muzny CA, Swiatlo E, Legendre DP. Breaking the Mold: A Review of Mucormycosis and Current Pharmacological Treatment Options.Ann Pharmacother. 2016;50(9):747-757.
- Amanati A, Barzegar H, Pouladfar G, et al. Orbital mucormycosis in immunocompetent children; review of risk factors, diagnosis, and treatment approach.BMC Infect Dis. 2020;20(1):770.
- Honavar SG. Code Mucor: Guidelines for the Diagnosis, Staging and Management of Rhino-Orbito-Cerebral Mucormycosis in the Setting of COVID-19. Indian J Ophthalmol 2021;69:1361-5.
- Mukherjee B, Raichura ND, Alam MS. Fungal infections of the orbit. Indian J Ophthalmol 2016;64:337-45.
- Sen M, Lahane S, Lahane TP, Parekh R, Honavar SG. Mucor in a viral land: A tale of two pathogens. Indian J Ophthalmol 2021;69:244-52.
- Sarkar S, Gokhale T, Choudhury SS, Deb AK. COVID-19 and orbital mucormycosis. Indian J Ophthalmol 2021;69:1002-4.
- Sen M, Honavar SG, Sharma N, Sachdev MS. COVID-19 and eye: A review of ophthalmic manifestations of COVID-19. Indian J Ophthalmol 2021;69:488-509.
- Rao R, Shetty AP, Nagesh CP. Orbital infarction syndrome secondary to rhino‑orbital mucormycosis in a case of COVID‑19: Clinico‑radiological features. Indian J Ophthalmol 2019;69:1627-30.