Squint is the Ocular Imbalance in which visual axes of both eyes do not meet at the point of regard. It can be regarded as a form of One Eye Blindness since both eyes are not seeing simultaneously, with a squinting eye being suppressed. Hence strabismus must be treated with due care. Squint evaluation can be simplified by the following checklist. Every squint patient must undergo this checklist of 10 commandments so as to plan management.
1. Determine whether True squint or a Pseudosquint
The architecture of face and orbit may give the impression of a person having an apparent deviation. Careful inspection of lids, adnexa, position of globes will reveal no actual squinting of eyes.
Two important parameters to rule out Pseudosquint
- Hirschberg reflex will always be centered
- No redressal movement on cover test
- Epicanthus and broad nasal bridge - extra fold of skin on the medial canthus gives the appearance of esotropia. On pinching the nasal bridge, the squint will disappear.
- Facial asymmetries, craniofacial anomalies, and hypertelorism
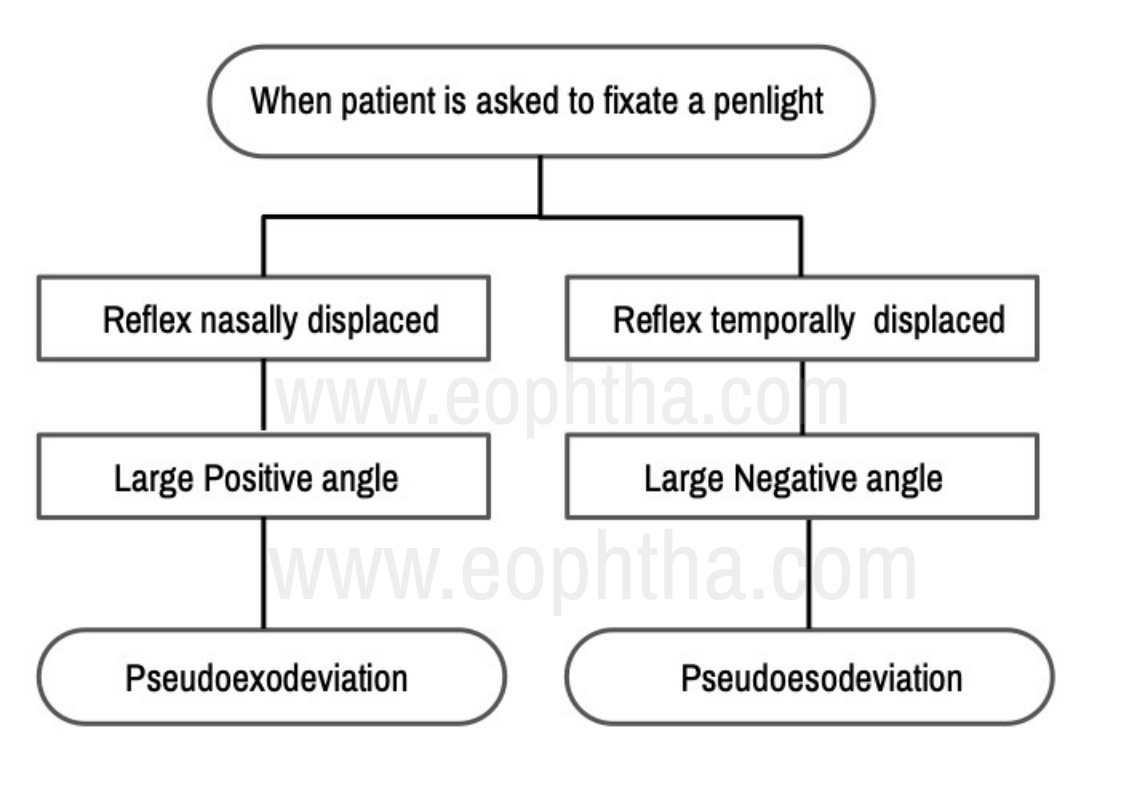
- Angle kappa- visual axis is the line joining fovea and the object of regard. The corneal reflex denotes the visual axis. The pupillary axis is the line passing through the centre of the pupil. Angle kappa is the angle between the pupillary axis and the visual axis.
These Pseudosquint conditions are not treatable since there is no ocular misalignment
2.Determine the Type of squint
Determine the Type of squint- i.e. the exact nature of misalignment. The larger deviations can be noticed mostly by looking at the person but smaller deviations need to be tested.
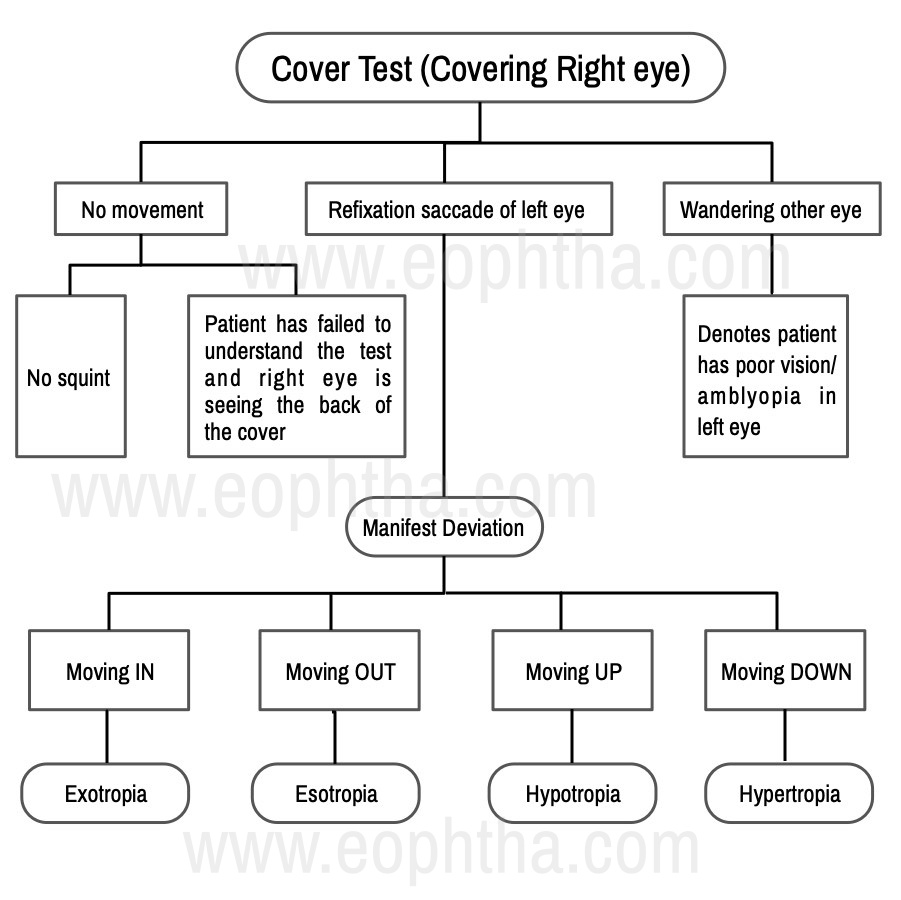
Cover test
The patient is asked to fixate at an object of regard. A cover is placed in front of a seemingly fixating eye and movement of other eye is noted.
For e.g. patient is seemingly fixing with the right eye
3. Determine whether Constant or Intermittent
Parents/ informant should be asked whether the deviation is present at all times or intermittently for e.g. when the child is tired or ill.
|
Fusional vergences |
|
|
Intermittent squints have good fusional vergences and hence the child is able to maintain orthophoria most of the times |
Constant deviations have poor fusional vergences and hence have tendency to squint perpetually |
- In intermittent squints there is no threat to binocularity as they have bifoveal vision in non-squinting phase
- Constant squints have poor binocularity since the deviated eye goes into suppression. Prolonged suppression can lead to sensory adaptation like amblyopia
How not to miss near and distant Intermittent squints
- Deviation may be present only in certain distances. For e.g esotropia for near, exotropias for distance
- In case of intermittent exotropias ask the patients to see as far distant as possible or patch one eye
- In case of intermittent esotropias determine by making patient fix at a near target. Near target should bring about accommodation
Never use a torch for testing near deviations since it fails to bring about accommodation
4. Determine whether Unilateral or Alternating
- Alternating squints are the ones in situations where the person fixes with each eye with equal preference
- Unilateral squints are said to present when under binocular conditions always one eye fixates and other eye deviates
For e.g. On covering the right eye, left eye esodeviation was noted i.e. the left eye moved Out. On uncovering the right eye the following situations can occur
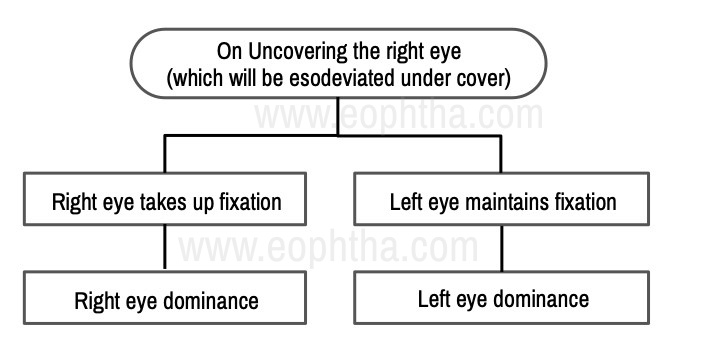
- On repeated testing on both eyes, if both eyes are seen to have equal tendency to deviate then the squint is said to be alternating
- If either one eye is found to have more tencency to squint then it is called unilateral squint
- Alternating squints have no binocular vision but usually have equal vision in both eyes (not necessarily normal vision)
- Unilateral squints will also have no binocularity and also there will be active central inhibition of the deviated eye leading to suppression and amblyopia
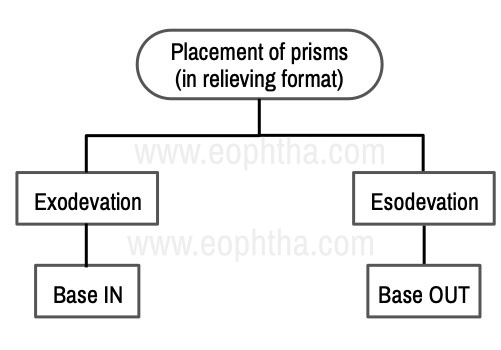
5. Measure the amount of squint
How prism bar cover tests work
On alternating cover tests, the deviating eye takes up fixation by redressal movement. On placing the prism, the object is shifted towards the deviated eye and no redressal movement will be seen. On placing the prisms in front of the eye the object will be seen shifted towards the apex and the image will be shifted towards the base.
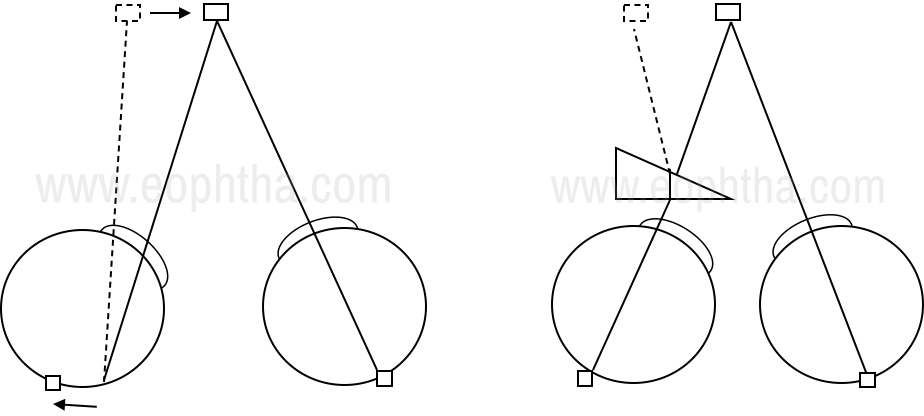
The alternate cover test is performed and the redressal movement is noted, increasing prisms are placed until no movement is seen.Alternate cover tests bring out the latent deviation by breaking the fusional vergences and tropias and phorias are measured
Krimsky test
It is used in patients with poor vision, small children, uncooperative patients
In patients with poor vision, the patient is asked to fixate on the penlight and increasing prisms are placed in front of deviating eye until the reflex is centered
But it is difficult to see the centration under the prism hence modified krimsky is used wherein prisms are placed in front of a fixating eye till reflex is seen centered on the deviated eye
Maddox rod
It is a stack of cylindrical lenses and image of point source of light is seen as line perpendicular to the cylinders
Dissociation will bring out latent deviation and since the images are different manifest deviation is measured
Hirschberg reflex
It gives a gross idea of measurement.
- At pupillary margin- 15 deg
- At the limbus- 45 deg
- In between- 30 deg
Quantifying the squint helps in planning the surgical treatment and follow-up
6. Check Motility
Motility is checked by ductions which are monocular movements and versions which are binocular movements in the same direction
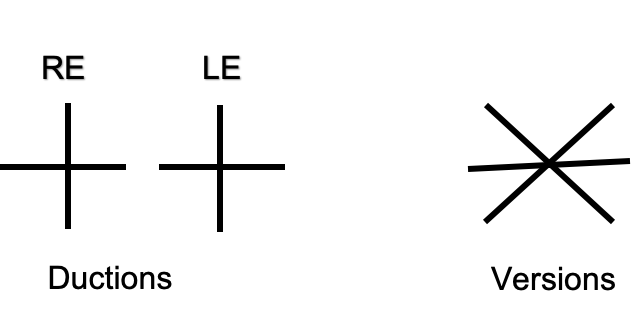
Version testing is important especially in case of early-onset nerve palsy. For e.g. In early-onset right 6th nerve palsy, on abduction, no deficit might be seen. This occurs because on abduction(monocular movement), right lateral rectus will receive more innervation and hence normal movement might be noted. But on dextroversion(binocular movement) with left eye fixing, equal innervation will be received by left medial rectus and right lateral rectus according to the herings law and hence the deficit will become evident.
Ductions testing becomes important to rule out pseudodeficiency.For e.g. In cases of infantile esotropia, an apparent abduction deficit is seen. Patching one eye and noting the abduction will rule out 6th nerve paresis. Another way is to perform dolls head manuvre.
Motility testing differentiates comitant from incomitant squints
7. Look for Pattern deviations
They are vertically incomitant horizontal squints
There is a difference in deviation from upgaze to downgaze
For e.g. in V Esotropia
- In primary gaze 50 PD of ET
- Upgaze – 10 PD of ET
- Downgaze – 80PD of ET
They are usually accompanied with abnormal head postures usually chin elevation or depression depending upon the gaze which is least affected
A esotropia and V exotropia -chin elevation
A exotropia and V esotropia – chin depression
Inferior oblique overactions and superior oblique palsy- V pattern
Superior oblique overaction and inferior oblique palsy- A pattern
Failure to recognize them can lead to under and overcorrections in vertical gazes
8. Assess Fixation pattern
It gives an idea about the visual acuity differences between the two eyes.
If a child resists occlusion of nondeviated eye or has nystagmoid movements of the deviated eye, then the vision in the strabismic eye is concluded to be grossly reduced
The vision should be checked whether it is centered, steady and maintained in each eye
- Centered- centrally fixating when another eye is covered
- Steady – follows the target when moved
- Maintained- continues fixating even after removing the cover from the other eye
In some cases, the amblyopic eye remains deviated when a fellow eye is covered.
Fixation preference is the only guide in preverbal children to monitor occlusion therapy
9. Look for the presence of Amblyopia
In children with strabismus, treatment depends on visual acuity in one eye with respect to others rather than absolute levels in each eye
In cases of unilateral squints, amblyopia should be treated by occlusion therapy or penalization and bring the visual acuity levels at par with that of the other eye
Alternating squints are the endpoint of amblyopia treatment and child can be taken for surgery
Always perform surgery in freely alternating squints
10.Sensory evaluation
It is the most important part of the evaluation of squint since it gives the idea of what the patient perceives. It is not important to have 6/6 in each eye. The endpoint of squint management is giving best quality stereoacuity and binocularity
Binocular fusion
The visually immature system develops adaptive sensory mechanisms by which sensory system adapts to abnormal motor situation
Suppression
- Active inhibition of image from the deviated eye
- This happens to eliminate disparate and confusing images which cause diplopia
- Tested with Worth 4- dot test
- The patient is asked to look at the box with 4 lights, 2 green, 1 red, and 1 white
- Red-green glasses with red in front of the right eye is placed
- The possible response could be
- 1 red, 2 green, 1 red/green- normal
- 2 red- left eye suppression
- 3 green- right suppression
- Alternately seeing 2 red and 3 green- alternating suppression
- Binocular perimetry and haploscopy
- Four prism diopter base-out prism
Abnormal Retinal Correspondence
- A non-foveal point corresponds to the fovea of the fixing eye giving rise to subnormal binocularity
- There is a binocular response despite having manifest deviation
- Tested with bagolinis striated glasses, major amblyoscope, after image tests
Stereopsis
- It is the indicator of the highest grade of binocularity and useful in directing treatment and prognosis
- Measured with titmus, TNO, synaptophore, lang, frisby
- Distant stereopsis is measured with Mentor B-VAT
- In strabismus, it is an important therapeutic goal to establish binocularity
- Testing for stereopsis is important in planning treatment and also post-surgery for followup.
It is the need of the hour for young ophthalmologists to realize that strabismus is One Eye Blindness and every attempt should be done to eliminate this needless blindness by befriending squint evaluation and management techniques.