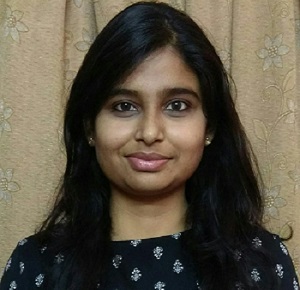
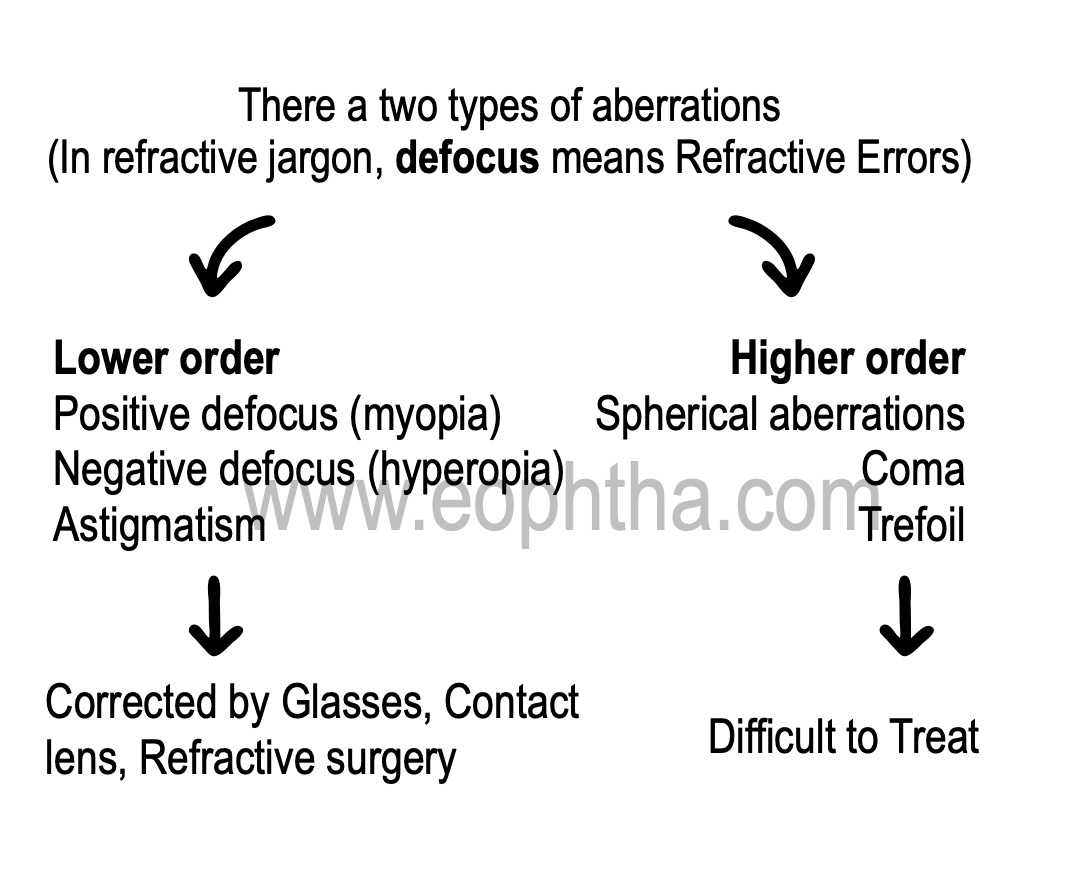
The optics of the eye normally creates a clear image by refracting rays of light to focus on the retina.Imperfections in this optical system create aberrations and thus blurred images. The goal is to analyze them and devise a means to eliminate them.
Lower order aberrations are primarily refractive errors when parallel rays of light after refracting, do not focus on the retina with accommodation at rest.
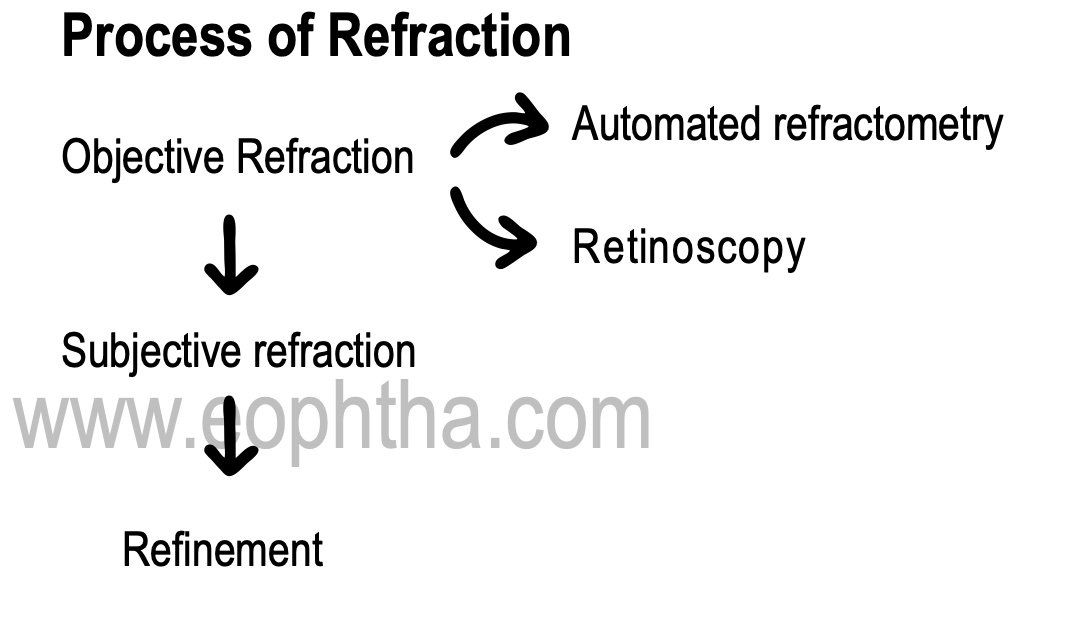
1. Retinoscopy
It is the objective method of detecting refractive errors by a method of neutralization.
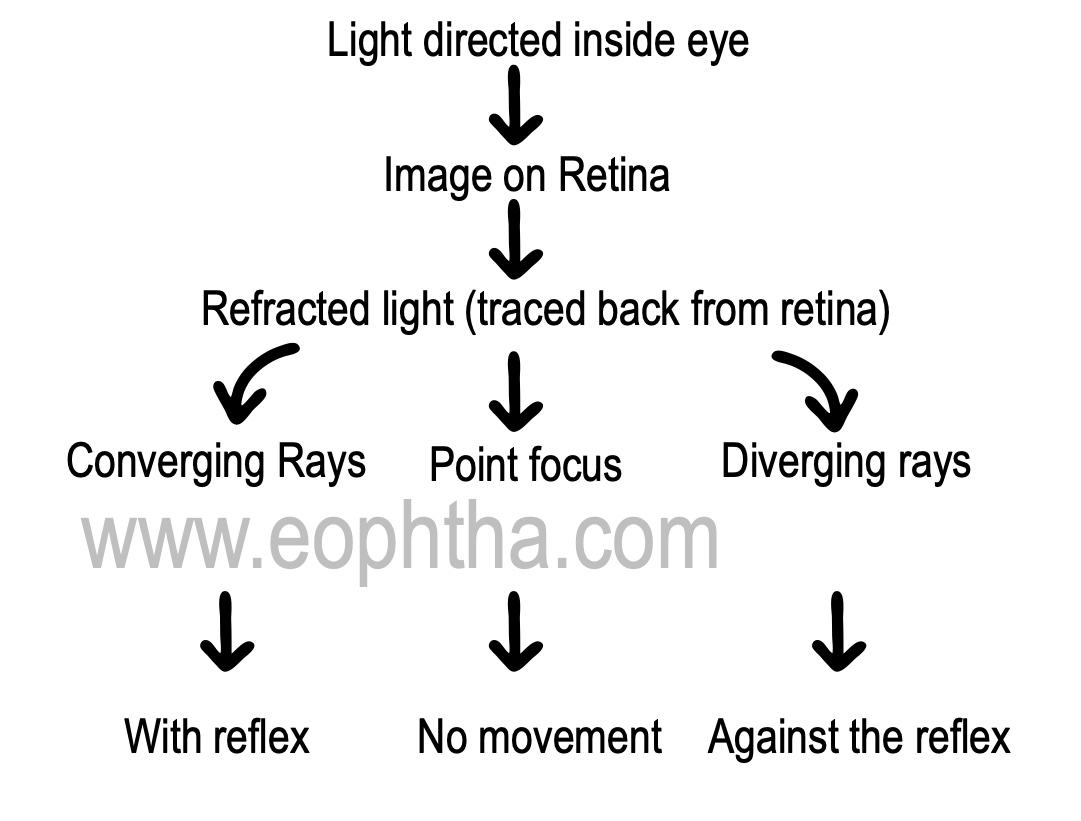
Point focusformed at a far point of the eye according to its refractive status. For e.g. In a patient with 1 dioptre of myopia, the far point is at 1 meter.
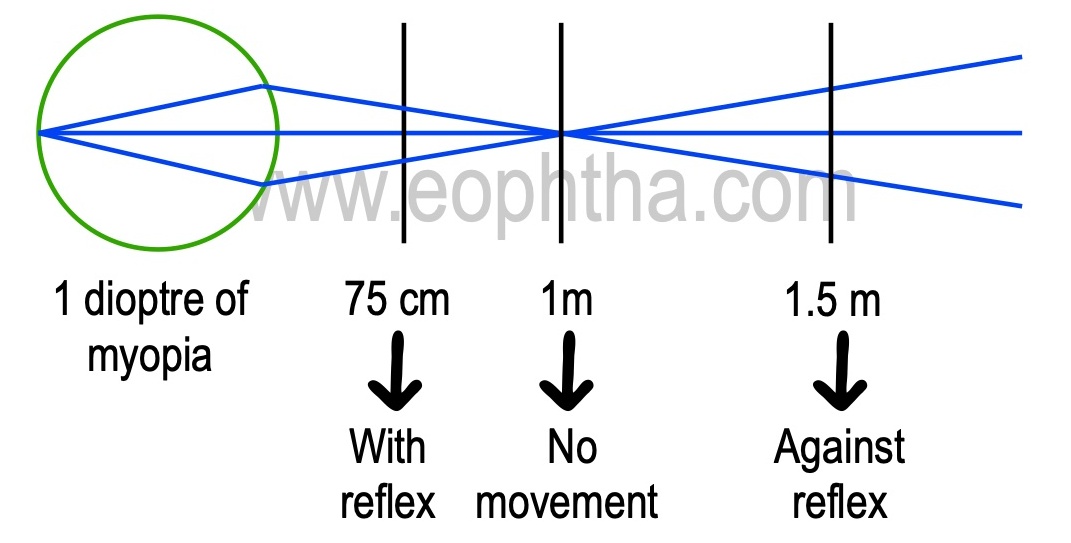 For easy mathematical calculations, 1metre is used for retinoscopy. But practically, 66cm is preferred as it is easier to perform retinoscopy at an arm’s length (which is 66cm). The two principal meridia are recognized and power is determined by neutralization. Usually the two meridia are 90 degrees and 180 deg. In cases of oblique astigmatism, rotate the streak accordingly.
For easy mathematical calculations, 1metre is used for retinoscopy. But practically, 66cm is preferred as it is easier to perform retinoscopy at an arm’s length (which is 66cm). The two principal meridia are recognized and power is determined by neutralization. Usually the two meridia are 90 degrees and 180 deg. In cases of oblique astigmatism, rotate the streak accordingly.
Steps to determine objective refraction
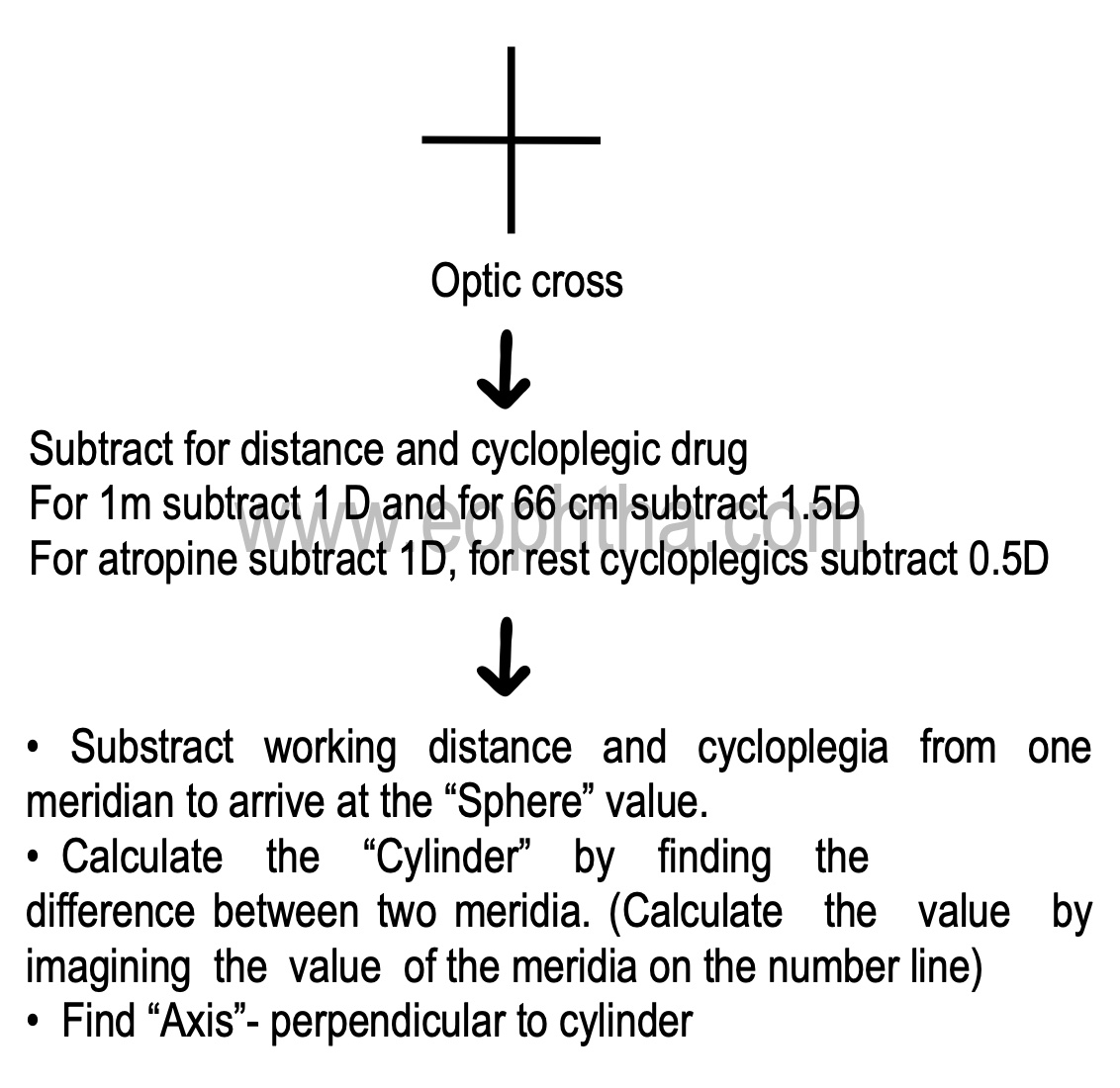
Transposition
It is a myth that a minus cylinder is better accepted by the patient than a plus cylinder. Both being optically similar, it does not make any difference to the patient’s vision. It is the machine that is used for grinding glasses that takes cylinder only in the negative form hence transposition becomes necessary in some cases.
2. Subjective refraction
The patient may not necessarily accept the calculated number deduced from objective refraction. Since it is a dynamic process, accommodation plays a role and distance correction might change. Trial and error with a combination of lenses should be used subjectively to finally prescribe glasses.However,objective refraction may be the only way to find out the refractive errors in certain situations for e.g. in small children, mentally unstable patients.
3. Refinement
After subjective correction, refinement is done to verify the sphere, cylinder, and axis.
Spherical lenses
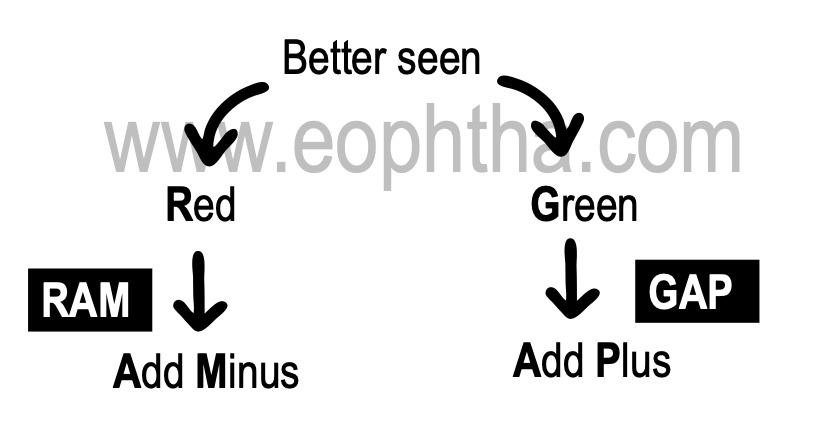
Duochrome test
The vision should be > 6/9
Can be done in colour blind person- since it depends on saturation and not colour per say
Cylinder lens
Jackson's cross-cylinderspherocylinder in which cylindrical power is double the spherical power
e.g +0.25D sphere with -0.5D cylinder at 180 deg
1. Fog with +1 D-
- Relaxes accommodation
- Fogging decreases visual acuity to 6/12 - 6/18 which helps in a better appreciation of any small change in vision
2. Straddle across test cylindrical axis - 45 deg on either side
3. Flip
4. Note the position of clearer vision
5. Move the test cylinder 5-7 degree towards the cross-cylinder of the same sign
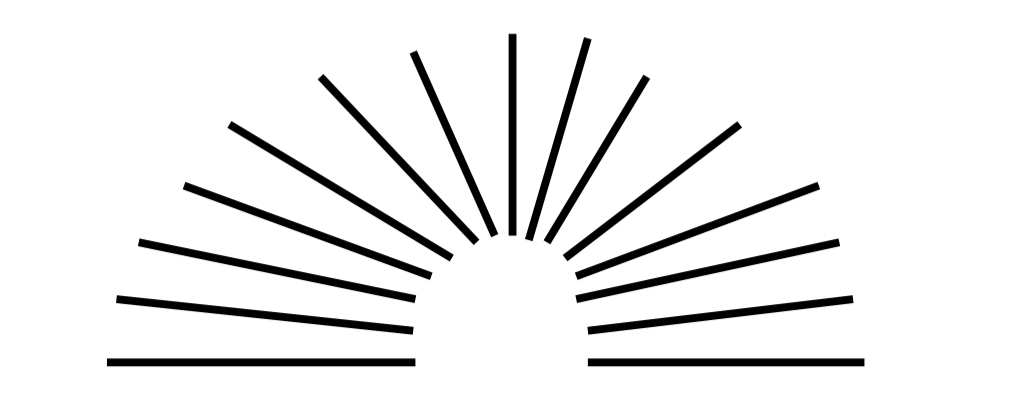
Astigmatic dial - radiating lines 180 deg used to look for uncorrected cylinder or to refine cylinder
1. Fog with +1D
2. Ask to report clearer/ darker lines and note the axis
3. Insert negative cylinder along this axis till all lines appear equally blurred
4. Remove fog and ascertain vision
Binocular balance
When subjectively checking vision monocularly, patients may accommodate unequally and high minus or low plus would be measured. The patient will not accept these glasses since on binocular viewing the accommodation will be symmetric and vision would be blurred in one eye. So, to eliminate this unequal accommodation, patients should be tested binocularly in the end.
• In cases of myopia and patients not accepting correction.
• To ensure equal relaxation of accommodation in both eyes.
1. Fog with +1 D.
2. Dissociate with a vertical prism of 12 PD in front of one eye.
- With both eyes open two Snellen charts one seen by each eye, will be seen vertically separated.
- Adjust the lenses in the trail frame so that both Snellens images would be equally blurred or equally clearer.
3. Remove the fog and reassess accordingly.
Presbyopia
Age should not be a criterion for presbyopic corrections. Every patient is different in terms of ciliary body physiology and occupational requirement. Presbyopia can occur earlier or later than 40 years. The correction should be individualized.
|
Near correction |
|
|
Classical method |
Practical method |
|
Minimum subjective correction + 1/4th amplitude of accommodation The amplitude of accommodation is calculated by measuring the near point of accommodation NPA (the point closest to the eye which can be seen clearly by maximum accommodation). 100 divided by NPA in cm gives the amplitude of accommodation. e.g. NPA of 25cm means 4D of accommodation |
Correction at a working distance should be enough to focus: 3 inches near and away from it. This is to ensure that there is no overcorrection or under correction of presbyopia. Ability to see 3 inches away avoids overcorrection and ability to see 3 inches closer avoids under correction |
• Never prescribe high reading glasses- give according to patients working distance requirements. Today's indulgence in smartphones and tablets with high contrast has drastically reduced the need for higher near corrections
• Reassess the need for bifocals in myopes- since patients having 1.5-2 D of myopia may not require glasses for near and maybe happy seeing for near without glasses.
Tips for refraction
1. Strongest plus and weakest minus which gives maximum visual acuity should be given- since accommodation will always be active while testing.
2. Never change well-adjusted glasses needlessly.
3. In high myopes use near vision as a guide to prescribe glasses especially in children.
Children with high myopia would have never used their accommodation in the past. By prescribing high minus glasses they will not be able to accommodate enough for the near-vision which then will be blurred and the child will not accept the prescribed glasses. Start the glasses by balancing both near and distance vision and over a period of time increase the minus lenses, this will bring inactive accommodation to the required strength.
4. Never prescribe a high minus cylinder for the first time (least cylinder compatible with BCVA)- better accepted by patients.
5. Use fogging to relax accommodation, cycloplegics can be used in cases such as pseudomyopia.
6. Over refraction can be used to confirm the correct number of the glasses- at 66cm with patient wearing glasses, retinoscopy will show ‘with reflex’ which will be neutralized by +1.5 D lens.
7. Vertex distance The trial frame should be checked at the same distance where the patient's glasses would be placed. The more the distance between the trial frame and eyes, the lesser will be the power measured for correction.
8. In cases of scarred corneas wherein, objective refraction may be difficult to find, Stenopaeic Slit is used. It is an elongated pinhole used to determine the principal axis of refraction.
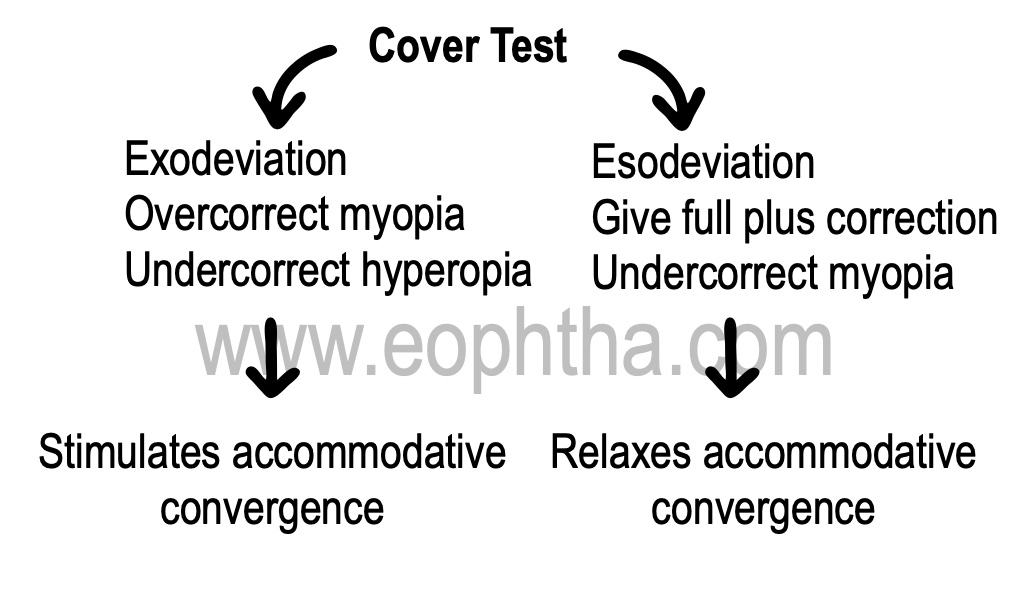
9. Perform cover test (CT)small corrections in refraction can help in balancing ocular deviations by stimulating or relaxing accommodative convergence.