Disc size
A normal disk can be of small size and a normal disk can be of a larger size; size by itself does not determine glaucoma. It is relevant because the disk size determines the C:D ratio and the neuroretinal rim thereof. In a large discone would expect a large cup and a large neuroretinal rim and in a small disc there is usually no cup. Disc size should be grouped as normal, small or large. Graticule on the slit lamp can be used.

In cases with CDR discrepancies disc size should be compared to determine true discrepancy.
Disc Shape
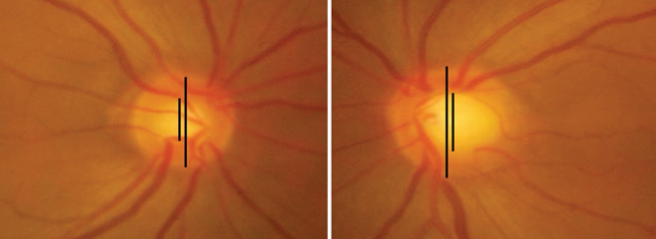
A normal optic disk is vertically oval with the vertical diameter being the maximum diameter and the horizontal being the minimum diameter.
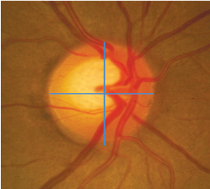
Figure: Vertically oval disc. Note that the vertical diameter is longer than the horizontal diameter
The variations in shape may be accompanied with astigmatism and amblyopia. An optic disk is considered torted when the vertical axis of the optic disk is rotated >15° from the vertical meridian. A tilted optic disk is when there is (three-dimensional) angulation of the (anteroposterior) optic cup axis. It is important to determine unusual shapes and document them as it would help in future comparisons and also the ISNT rule (discussed later) will not always be applicable in disks that are not vertically oval.
The configuration and depth of the cup are best judged by the stereoscopic examination. The contour cup is more important than the color cup. Carefully follow the optic nerve blood vessels and note the kinks in the vessels as they climb on the cup wall. At the cup rim junction, the vessel will kink and bend over the rim. This second kink in the blood vessel determines the cup margin.
The Neuroretinal Rim
The neuroretinal rim is the most important parameter of the optic disk evaluation. The optic disk is vertically oval and the cup is horizontally oval thus the rim has a characteristic configuration where the inferior (I) rim is the widest, followed by the superior (S) and nasal rims (N) and the temporal (T) rim is the thinnest. This is the ‘ISNT rule’ which helps to determine glaucomatous changes in the disk glaucoma.
The cardinal feature of glaucomatous optic neuropathy is the loss of NRR from the inner edge of the rim. The sequence of loss is usually first in the inferotemporal and superotemporal disk regions. So for early diagnosis, these areas should be carefully evaluated for glaucomatous changes. In moderate disease, the temporal part of the horizontal disk is involved and in advanced glaucoma, the rim remnants are located mainly in the nasal sectors.
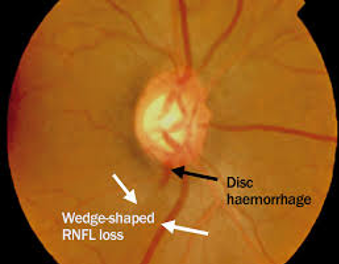
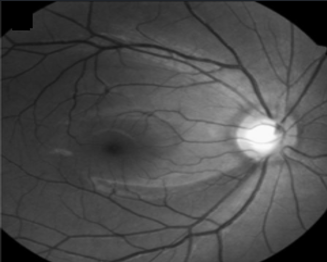
Retinal Nerve Fiber Layer Defect
The retinal nerve fiber layer defect is a very strong indicator of early glaucoma but is not pathognomonic. Most localized RNFL defects were associated with neuroretinal rim thinning, notching, or vertical cup enlargement. They are best viewed in with a Red free filter.
Disc Hemorrhage
One should note the presence of flame-shaped and linear streak hemorrhages around the disc carefully. Most commonly seen in the superotemporal or inferotemporal margin of the disc. Hemorrhages are risk factors for progression of glaucoma and are more common in normal-Tension Glaucoma.