

1. Basic structure of phaco probe
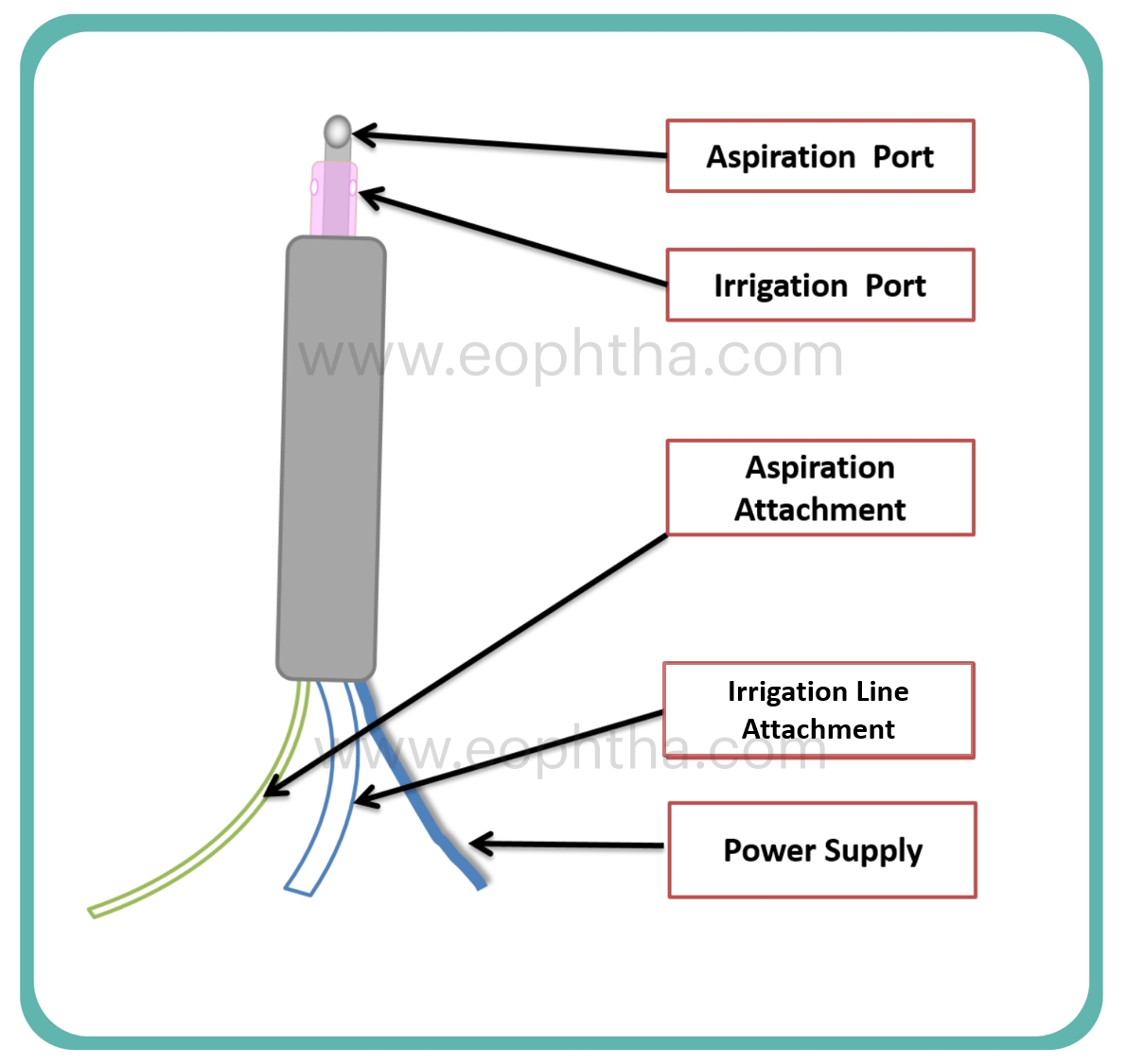
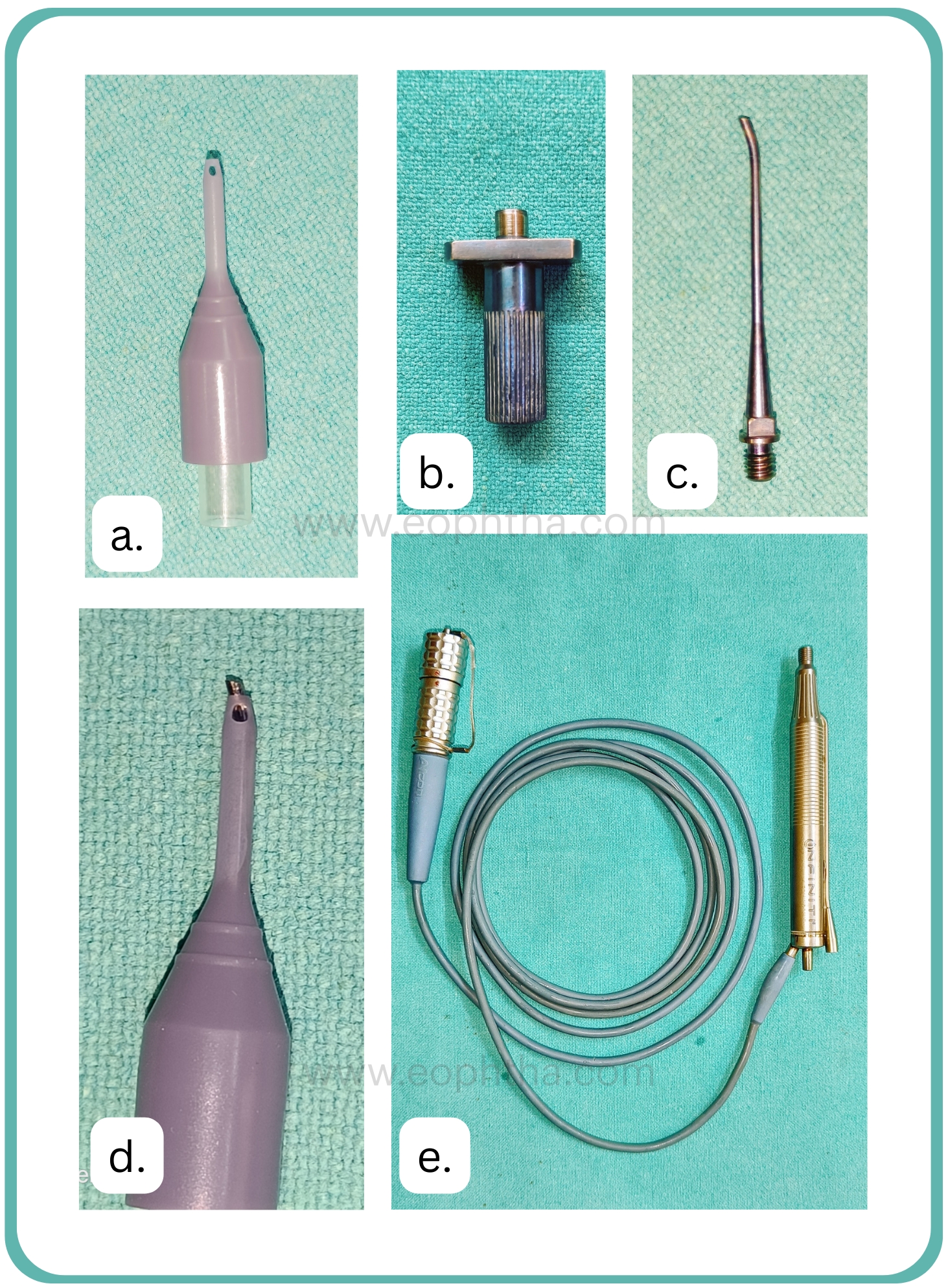
Phaco Probe has two attachments (For aspiration & Irrigation) and one wire coming out of back end for power supply and sensors. In the front there is the tip attached to the hand piece, which has a silicon sleeve around it with two apertures. The irrigation tubing are wider in diameter than aspiration and both tubings are colour coded
2. Fluid Inflow and Outflow pathway:
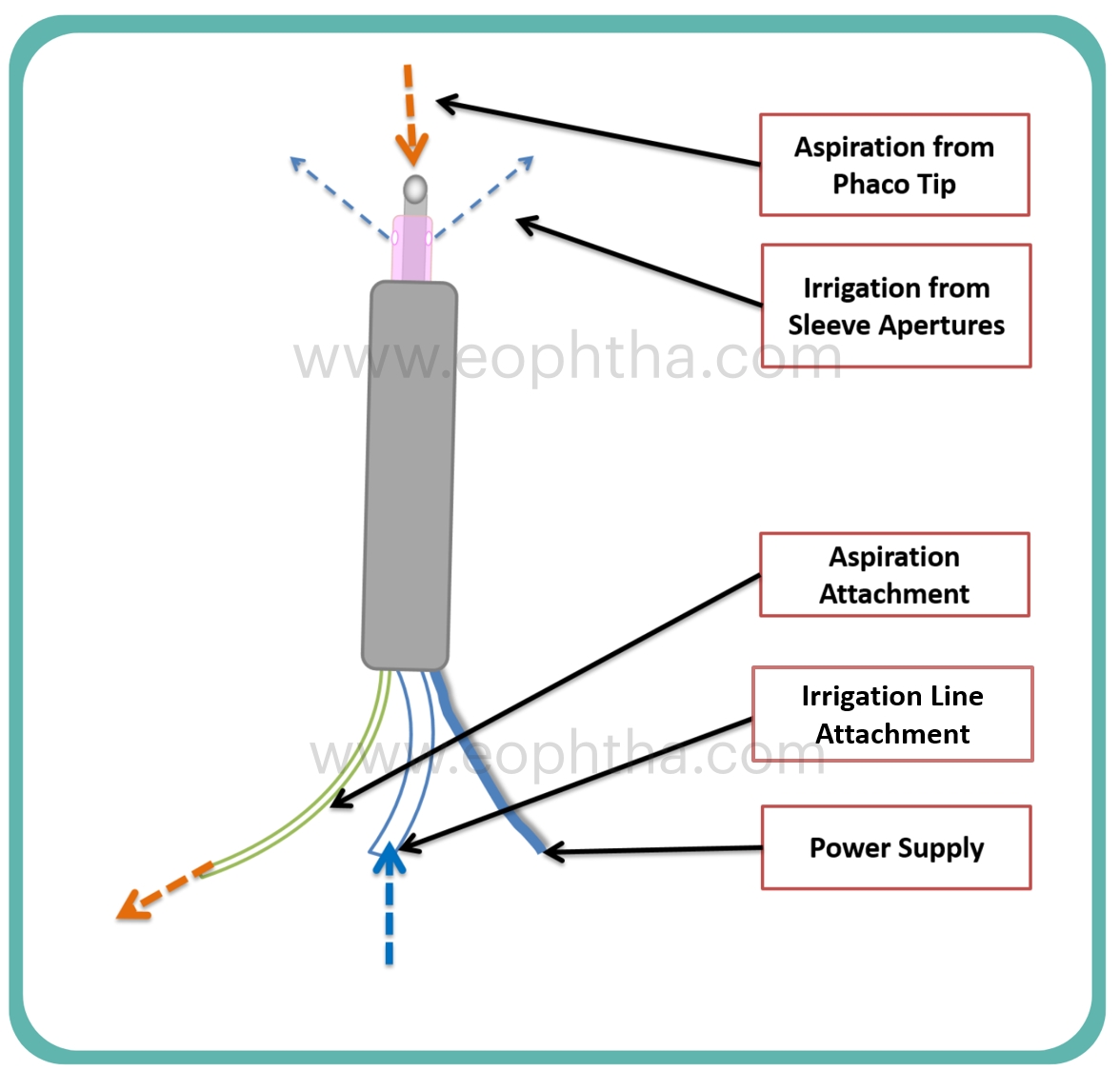
The fluid flows from the irrigation tube to the handpiece and comes out via two apertures in the silicon sleeve cooling the tip. It then traverses in the AC and is aspirated back via phaco tip and comes out via aspiration tube. Irrigation is gravity based in traditional machines and Active in newer generation machines. Aspiration is always active can be via either peristaltic and venturi pump based.
3. Phaco Tip design:
- Phaco tip is made of titanium alloy. The end of the tip has a bevel, which can be of varying degree of angulation ranging from 0–60°. As the angulation increases the cutting power increases, holding power decreases, and vice versa. Therefore, 0°tip has highest holding capacity and lowest cutting ability, Similarly 60° has lowest holding capacity and highest cutting ability.
4. Phaco energy
Phaco handpiece has piezoelectric crystals, which vibrate when electricity passes through it. They are in contact with phaco tip and generated movement of tip ( phaco power). The amount the phaco power depends on the stroke length. Amount of stroke length can be adjusted using machine console. There are two basic mechanisms for phacoemulsification
- Jack Hammer Effect The rapid back and forth movement of the tip causes mechanical hammering effect and disintegrates the tissues.
- Cavitation phenomenon: On the backward, motion of the tip, causes cavitation and it causes implosion in the surrounding tissues.
5. Phaco Tip functionality:
For novice surgeons, there is no awareness of the extent of tip exposure. It is recommended that the phaco tip exposure be just adequate; it should be less in the case of soft cataracts and more in the case of harder cataracts. For proper holding, the tip must be buried deep within the hard nucleus. Or in case of soft nucleus efficient use of vacuum is done to hold the nucleus. All the phaco manoeuvres should be done keeping the bevel of the tip facing up. Tip should be inspected daily for damage and should be replaced if visible damage is seen or if the cutting power is compromised.
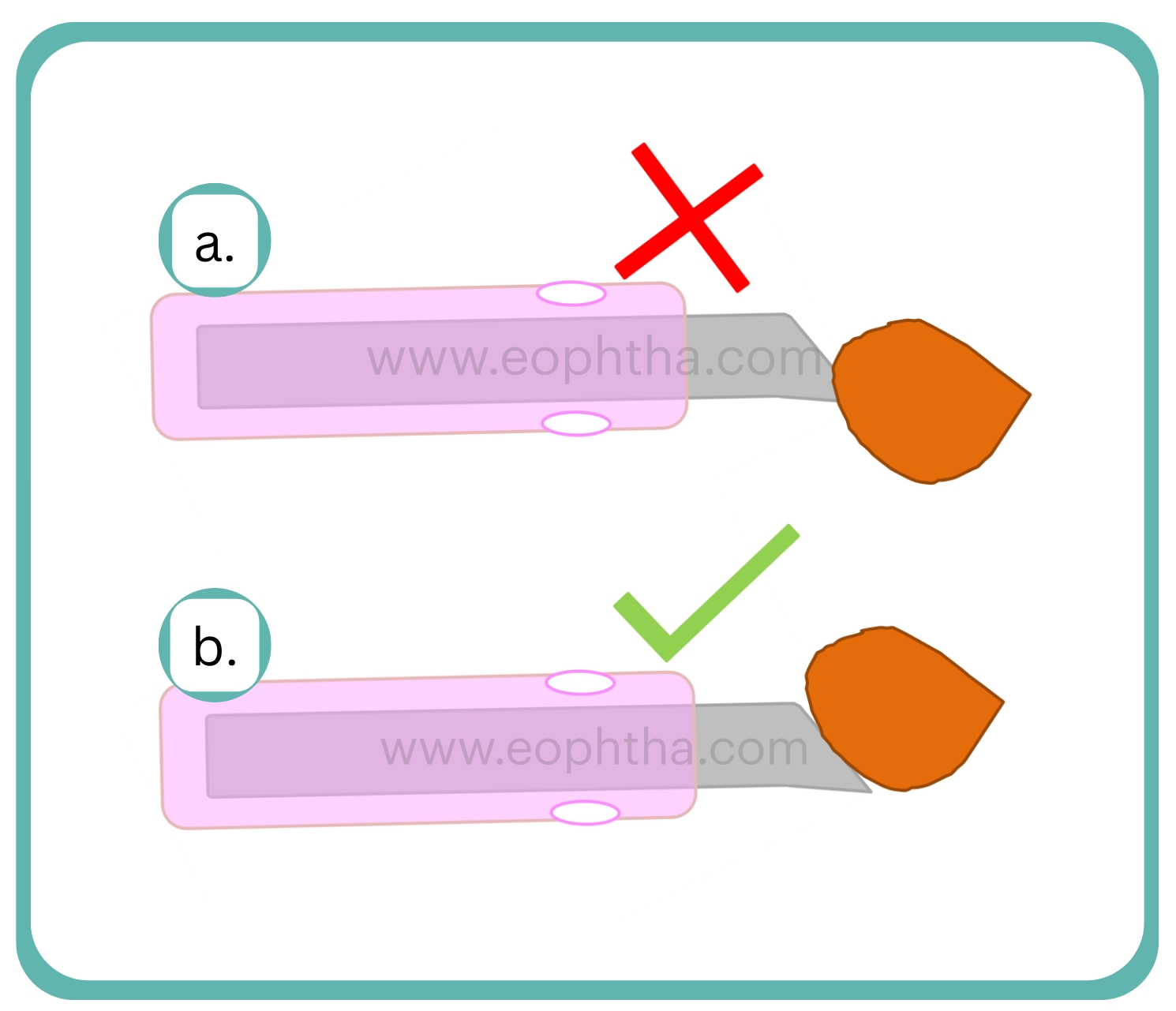
6. Phaco Sleeve:
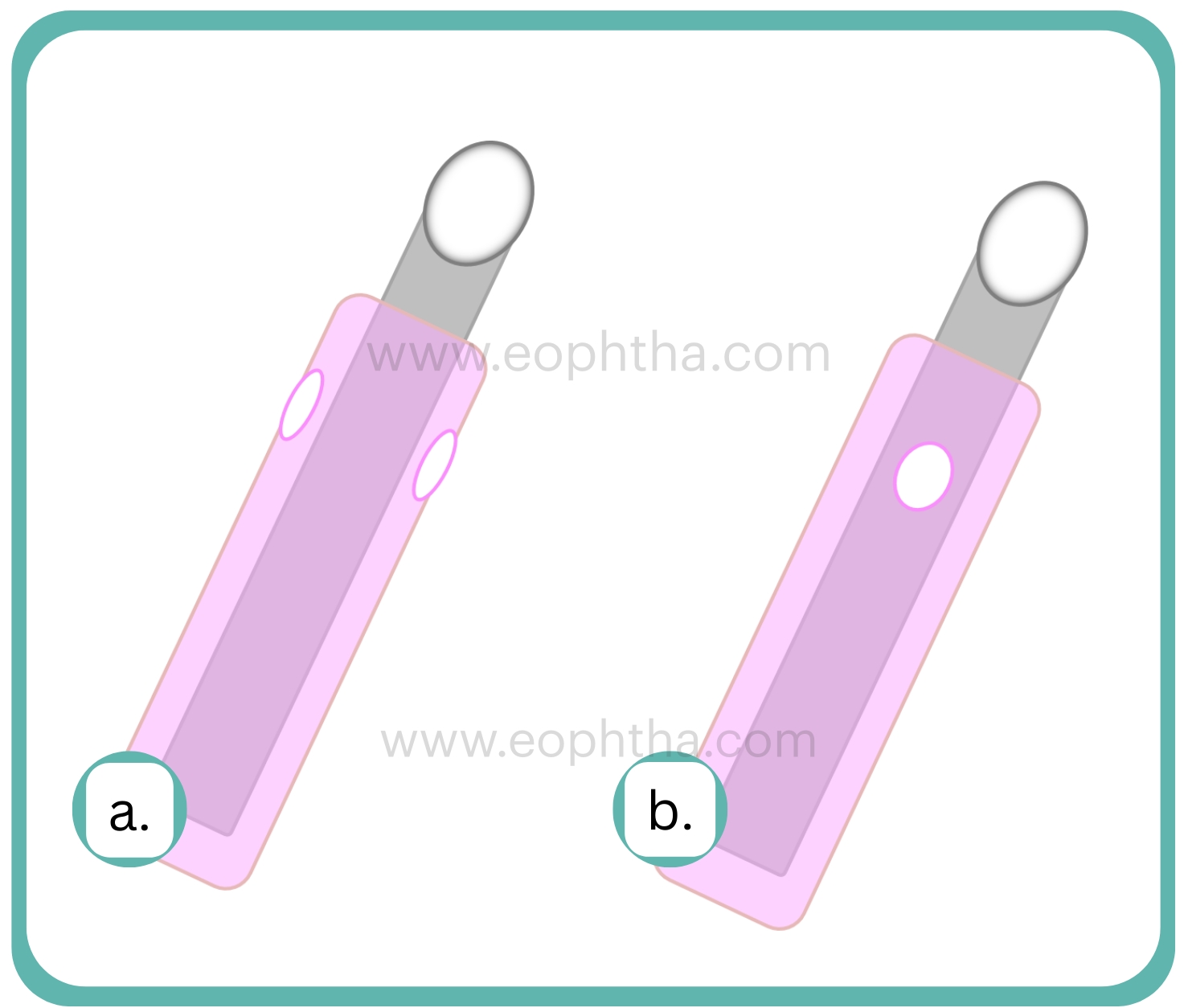
Always inspect the sleeve for position with respect to irrigation ports and tip exposure. Always make sure that the irrigation ports are facing to the side of the probe. Sometimes the sleeves are damaged or torn which should be discarded, as they will not function effcetively.
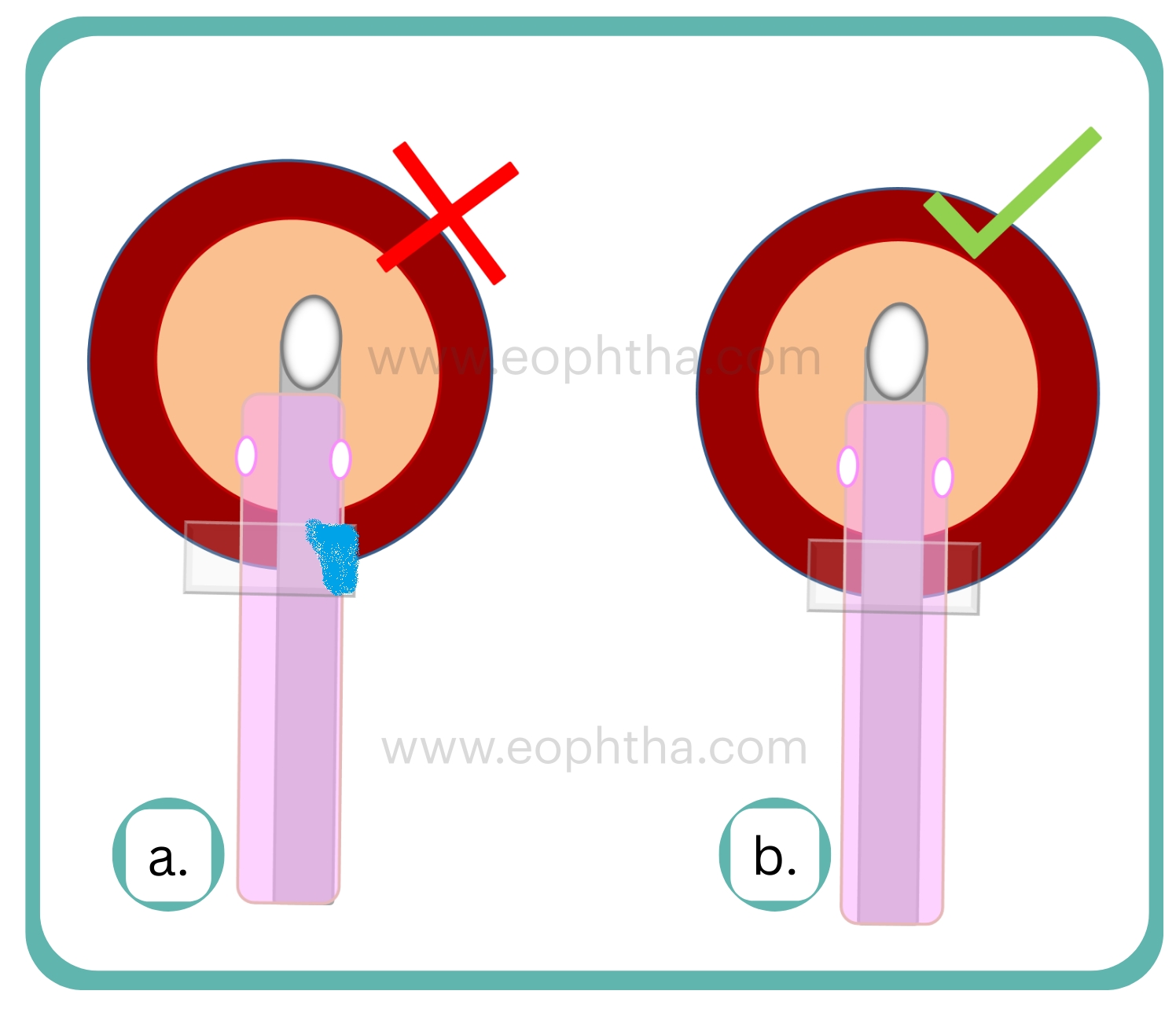
7. Centration of Probe and Tip:
While performing phacoemulsification, it is very critical to keep the tip of the probe in the centre of the sleeve in order to avoid causing burns to the wound, which can happen if it is tilted to one side during the procedure. Due to the fact that the tip gets heated up and needs fluid flow all around it to keep t cool, it is crucial that the tip stays in the centre of the sleeve at all times.
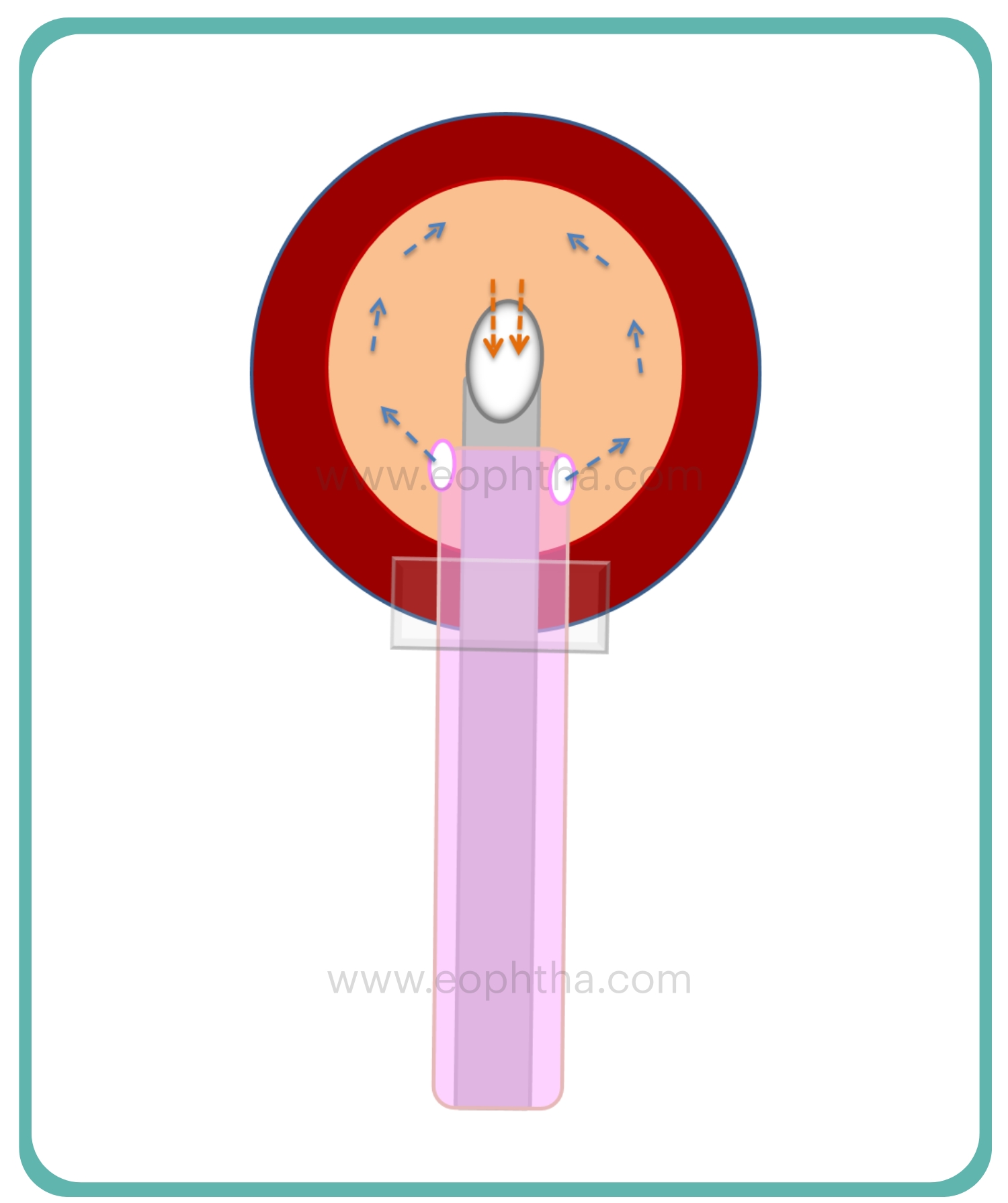
8. Maximise utility of probe using phaco dynamics
It is very essential to keep irrigation ports on side for maintaining good followability. As the fluid flow through the irrigation ports travels across the AC and going in the phaco tip due to this fluid flow nuclear fragments move towards the phaco tip, this is called "followability". If the ports are directed up and down, the fluid will hit the endothelium and lead to endothelial cell loss.
Proper orientation of phaco tip to nuclear fragments: the phaco tip should be in contact with maximum nuclear surface area before giving bursts of energy to hold. As to generate the vacuum and good hold in peristaltic pump based phaco machines, occlusion has to be there. Therefore, for good occlusion, good orientation of phaco tip and nucleus is mandatory.
9. Nuclear Fragments Stuck:
While operating hard cataracts, sometime nuclear fragments are stuck in the probe or tubing and you get constant occlusion sounds and you cannot emulsify. In that case follow the following steps
- Step 1 Remove the probe from eye and try to give power in water bath
- Step 2 If not successful, then try flushing the probe after removing the tubing
- Step 3 If not successful then you need prime the cassette and probe.
10. Phaco Handpiece and Tip Sterilization:
Perform the following steps to thoroughly clean the handpiece.
- Step 1: Remove the irrigation and aspiration tubing from the handpiece.
- Step 2: Unplug the handpiece connector from the console and install protective cap.
- Step 3: Remove the infusion sleeve and tip from the handpiece using a tip wrench and discard according to surgical facility guidelines.
- Step 4: Wipe any residue from the handpiece with a soft, clean, lint free non-abrasive cloth and rinse the handpiece with room temperature sterile deionized water to remove any remaining debris. If necessary, wash the exterior of the handpiece using a soft bristled cleaning brush.
- Step 5: Using a syringe, push a minimum of 120cc of room temperature sterile, deionized water through both the irrigation and aspiration paths.
- Step 6: Using the same syringe, flush both ports with a minimum of 60cc of air.
- Step 7: Dry the exterior surfaces of the handpiece and cable with a soft, dean, lint free non-abrasive cloth.
- Step 8: Visually inspect to ensure the Handpiece is clean and dry. Repeat the process as needed.
- Step 9: Place the cleaned handpiece and cable in the sterilization tray to prevent damage to connector and handpiece during storage and autoclave or wrap to prevent damage in preparation for autoclaving.