

Unlike in adults , the risk of risk of developing visual axis opacification (VAO) after cataract surgery in children is nearly 100%.[1,2] Hence the need for primary posterior capsulotomy (PPC) and anterior vitrectomy (automated/manual) in pediatric cataract surgeries.Let us answer the few salient features of PPC and AV in following ten questions ,
1. Why PPC is needed?
The anterior hyaloid face in infants and young children is highly reactive and closely linked to the posterior capsule. It serves as a scaffold for the accumulation of lens epithelial cells and other inflammatory cells, resulting in VAO in almost all cases.[3,4] The VAO will continue to have the amblyogenic effect nullifying the purpose of cataract surgery in the child. Further the amblyogenic effect of VAO increases as the age of the child decreases. Therefore, PPC with/without anterior vitrectomy is necessary to determine the ultimate visual outcome of cataract surgery in young children.Further In addition, PPC may also be need in presence of dense, adherent posterior capsular plaques or to convert congenital or traumatic posterior capsular defects into a more stable opening.
2. Until what age will we need to consider PPC and anterior vitrectomy in pediatric cataract cases?
While there are different schools of thought on the ideal age until the surgeon needs to consider a PPC, the common consensus is that the ultimate objective is to keep the visual axis clear. In children aged six years and older, the inflammatory response and the risk of consecutive VAO are less than in younger children.[2] So, any child less than 6 years must get a PPC and AV during the cataract surgery.
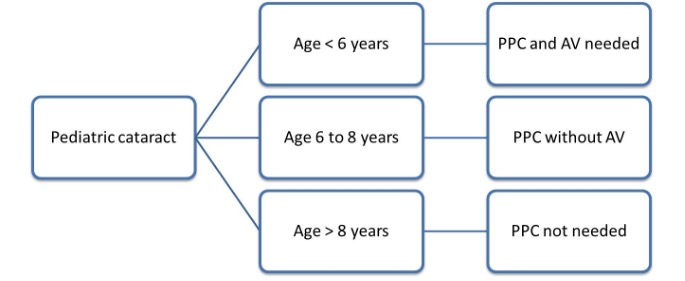
Children between 6-8 years may not need AV and just doing PPC would suffice . These children have higher chances of maintaining a clear visual axis with just doing PPC. However, anterior vitrectomy must be done in any case with an inadvertent vitreous prolapse while doing PPC. However, certain special situations warrant PPC and AV even in older children like ,
- Associated developmental delay and nystagmus.
- General conditions which may interfere with child’s cooperation for yag capsulotomy[2,5]
- Thick adherent post plaque or thick post polar cataract
- Preexisting post capsular rupture
3. What are the different methods of doing a PPC?
Primary posterior capsulorhexis can be performed via anterior ( limbal or posterior (pars plana )approach. Most pediatric surgeons prefer the anterior approach.
The PPC can be performed via ; a) using the manual technique (capsulorhexis) with cystitome and microrhexis/ utrata forceps, b)using vitrector (vitrectorrhexis/capsulectomy). Other available techniques include using the FEMTOLASER, Fugo blade, and diathermy blade.
Manual post capsulorhexis is most commonly performed and preferred technique .Further doing it with micrrhexis forceps via sideport is better as it maintains anterior chamber compared to doing via mainport using utrata forceps.
4. How is a PPC different from an anterior capsulorhexis?
- The posterior capsule (PC) is thinner and more elastic than the anterior capsule; however, there is less risk of runaway and radial tears due to decreased pressure on zonules after the crystalline lens has been removed.
- The anterior chamber (AC) depth has to be maintained throughout, but most surgeons prefer a slightly underfilled AC, which helps bring the PC anteriorly.
- When using the forceps method, the frequent regrasping technique for anterior capsulotomy is essential for PPC.
- The maintaining of anterior hyaloid face during PPC aids in ease of doing it. Disturbance of AHF with vitreous prolapse will increase the difficulty and risk of run away rhexis .
5. What is the adequate size of PPC?
An ideal PPC has to be well-centred, circular and of optimum size viz 1-1.5 mm smaller than anterior rhexis ( which is usually 5 to6mm) in cases where IOL implantation is planned . If IOL implantation is not planned ( in cases of infants < 6 months, microcornea or microphthalmos) then size of PPC should be made equivalent to size of anterior rhexis. This will help fusion of anterior and post flaps and entrap equatorial cell proliferation within preventing visual axis opacification.
Further if IOL implantation planned with posterior optic capture( i.e., haptics in bag with optic through PPC in AHF) , then the size of PPC has to be slightly larger than routine and planned according to the optic size of IOL.
A very small PPC may result in spontaneous closure and eventual VAO, while a very large one will lead to difficulties stabilising the intraocular lens (IOL).
6. When should the PPC and anterior vitrectomy be done intraoperatively- before/after the IOL implantation?
|
Before IOL implantation |
After IOL implantation |
|
|
Advantages |
Visibility of post capsule to do ppc is better Can titrate the size of PPC better Can be done via sideport Completion of anterior vitrectomy can be achieved and ascertained better Can opt to change to three piece iol into sulcus if PPC extension |
IOL is placed in the bag so stability of IOL ascertained |
|
Disadvantages |
Cons : IOL implantation slightly challenging soft, vitrectomised eyes. |
Cons : Difficulty in lifting IOL to do PPC and AV( poor visibility and difficult maneuvering) Completion of anterior Vitrectomy difficult to ascertain Since IOL is already placed , extension of PPC can be messy to explant and replace with 3 piece IOL |
The technique chosen largely depends on the training received and comfort of operating surgeon
7. How to do PPC and anterior vitrectomy?
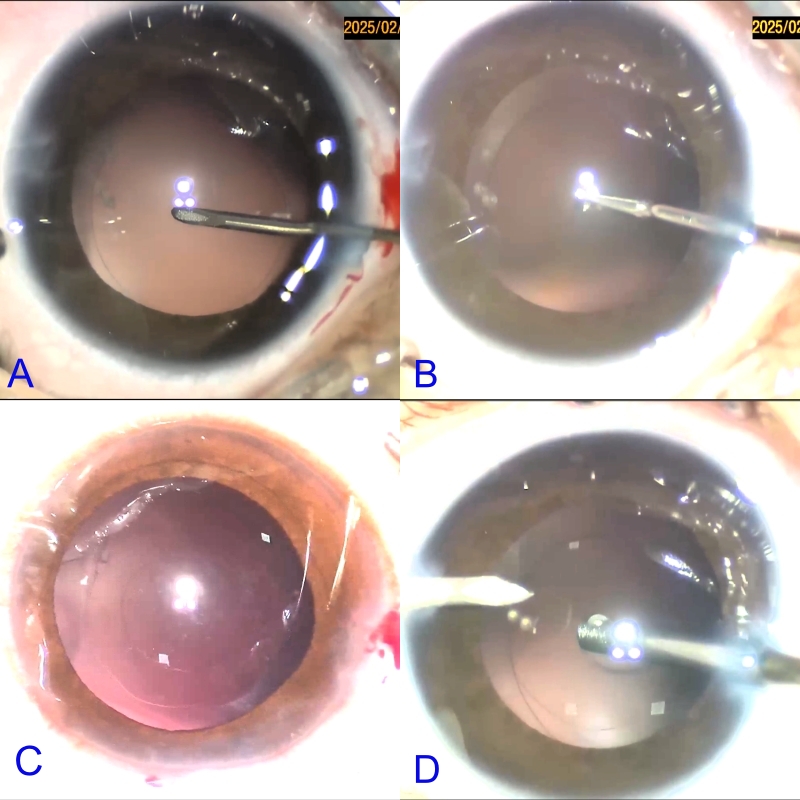
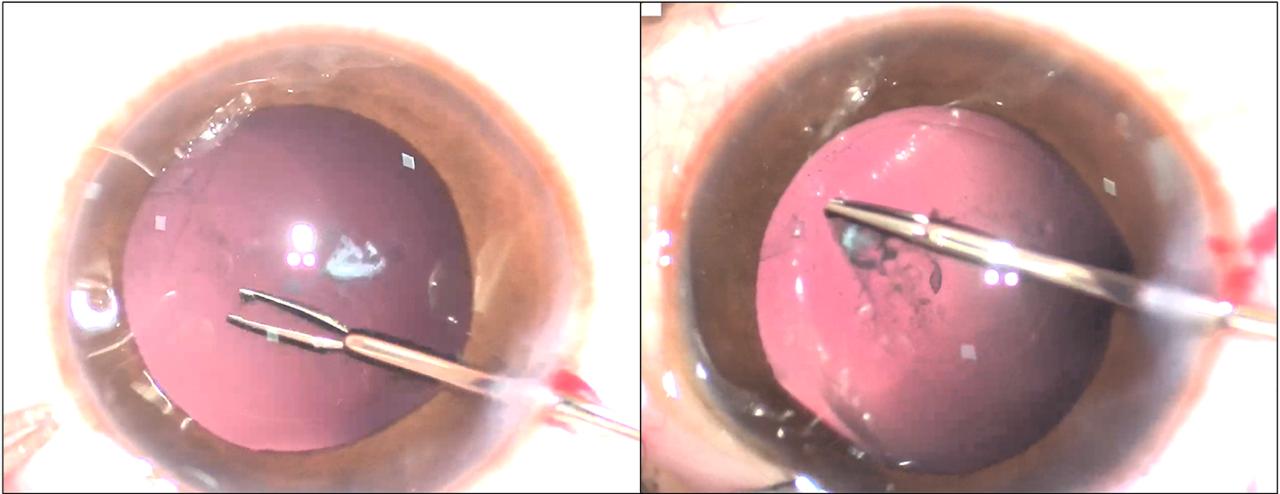
After making a central nick, it is crucial to inject viscoelastic substance into the Berger’s space to push the anterior hyaloid face posteriorly to avoid untimely vitreous disturbance, especially in cases where vitrectomy is not planned . The viscoelastic agent should not push the flap posteriorly, as this makes it difficult to grasp the posterior capsule tag. The PPC is then completed using microrhexis forceps with multiple grasps as shown.
8. What are the alternative techniques for making a PPC?
Gimbel’s technique- Gimbel described a method involving PPC and a posterior optic capture of the IOL placed in the capsular bag.[2,6-8] It involves placing the optic through the anterior and posterior capsulorhexis openings to capture and stabilise the IOL in the posterior chamber while the haptics are in the capsular bag. This helps to attain a 360-degree apposition of the anterior and posterior capsule leaflets, except at the optic-haptic junction, providing a barrier between the aqueous and vitreous without needing anterior vitrectomy. This will lead to the deposition of inflammatory debris and lens epithelial cells anterior to the IOL, where they will be removed by the aqueous. The continuous turnover of aqueous will help disperse any epithelial proliferation.
Bag in the lens (BIL) fixation technique- This technique was introduced by Tassignon et al in 2007.[9] Anterior and posterior capsulorhexes of equal diameter are performed and then captured into the groove of the specially designed IOL. Thus, BIL blocks the two capsulorhexes in its groove, merging the two capsules all around, forming a new barrier to epithelial cells. The perfect 360° overlap of the two capsulorhexes decreases the risk of VAO.
9. How much anterior vitrectomy is adequate, and what is the endpoint?
Sufficient vitrectomy must be done so the lens epithelial cells cannot use the anterior hyaloid face as a scaffold to cause VAO. The usual goal is to clear the central anterior vitreous. Any vitreous that tracks anterior to the plane of the PPC has to be removed.(figure)
10. What are the techniques to tackle cases with posterior capsule abnormalities?
Posterior capsule plaque- If the plaque is small and central, it is easily removed along with the usual PPC or peeling with cystitome. However, in other cases with adherent and irregular plaques, incomplete PPC and untimely vitrectomy may result. In such cases, intraocular scissors and forceps is used to convert the tears into posterior rhexis as far as possible.
Posterior lenticonus- PPC becomes difficult in these cases due to relaxation of the posterior capsule. In many cases, it also leads to a posterior capsule rupture during the surgery. The loose posterior capsule can be handled by frequently adjusting the point of hold of the PPC flap and the direction of pull.moreoften than not may require placement of IOL in sulcus with optic captured through anterior rhexis.
Pre-existing posterior capsular defect- The defect can be converted into a PPC using the intraocular scissors and forceps, followed by a posterior optic capture depending on the condition of the defect. Vitrector can also convert the defect into PPC along with the anterior vitrectomy.
Persistent fetal vasculature (PFV)- Vitrector is used to remove the retrolental fibrovascular plaque and the prolapsed vitreous.The intraocular cautery may be required in presence of vessels in the stalk.The parsplana approach may be needed in presence of PFV stalk connected to disc. If the posterior capsule defect is significant, the IOL is implanted in the ciliary sulcus. If the defect is small with minimal vitrectomy done, the IOL can be placed in the capsular bag itself with or without a posterior optic capture.
REFERENCES
- Parks MM. Posterior lens capsulectomy during primary cataract surgery in children.Ophthalmology. 1983;90(4):344-345. doi:10.1016/s0161-6420(83)34549-8
- Gimbel HV, DeBroff BM. Posterior capsulorhexis with optic capture: maintaining a clear visual axis after pediatric cataract surgery.J Cataract Refract Surg. 1994;20(6):658-664. doi:10.1016/s0886-3350(13)80659-1
- Cobo LM, Ohsawa E, Chandler D, Arguello R, George G. Pathogenesis of capsular opacification after extracapsular cataract extraction. An animal model.Ophthalmology. 1984;91(7):857-863. doi:10.1016/s0161-6420(84)34225-7
- Nishi O. Fibrinous membrane formation on the posterior chamber lens during the early post-operative period.J Cataract Refract Surg. 1988;14(1):73-77. doi:10.1016/s0886-3350(88)80068-3
- Hiles DA, Hered RW. Modem intraocular lens implants in children with new age limitations. J Cataract Refract Surg 1987; 13:493-497
- Arbisser, Lisa B.. Review of primary posterior capsulorhexis in cataract surgery. Saudi Journal of Ophthalmology 36(2):p 149-156, Apr–Jun 2022. | DOI: 10.4103/sjopt.sjopt_183_21
- Gimbel HV. Posterior continuous curvilinear capsulorhexis and optic capture of the intraocular lens to prevent secondary opacification in pediatric cataract surgery.J Cataract Refract Surg. 1997;23 Suppl 1:652-656. doi:10.1016/s0886-3350(97)80049-1
- Gimbel HV. Posterior capsulorhexis with optic capture in pediatric cataract and intraocular lens surgery.Ophthalmology. 1996;103(11):1871-1875. doi:10.1016/s0161-6420(96)30414-4
- Tassignon MJ, De Veuster I, Godts D, Kosec D, Van den Dooren K, Gobin L. Bag-in-the-lens intraocular lens implantation in the pediatric eye.J Cataract Refract Surg. 2007;33(4):611-617. doi:10.1016/j.jcrs.2006.12.016