
Eye diseases affecting the cornea are a major cause of blindness worldwide. Among different infectious agents, bacteria, fungi, viruses and protozoans may be causes of keratitis. This article is about the keratitis caused by protozoa.
Three amoebic parasites are thought to be significant to human disease, entamoeba which is responsible for amoebic dysenter, naegleria which causes amoebic meningoencephalitis and acanthamoeba which is known for causing keratitis and granulomatous amoebic encephalitis.Acanthamoeba is a ubiquitous, free living protozoa of the subphyla Sarcodina. It is considered as opportunistic pathogen in humans. Acanthamoeba keratitis is a potentially devastating corneal infection which can lead to severe visual loss.
Epidemiology:
Acanthamoeba keratitis (AK), is rare in the general population (estimated incidence: 1.4 per million person- year) but much frequent in contact lens wearers. The incidence of the disease in developed countries is approximately 1-33 cases per million contact lens wearers. In the United States, an estimated 85% of cases occur in contact lens users. However in developed countries it is mainly associated with trauma and exposure to contaminated water. In India, Acanthamoeba accounts for 2% of all cases of culture positive corneal ulcers at tertiary eye care centers.
Risk factors:
Contact lens use is the single most important risk factor for AK in the developed world. AK comprises of <5% of CL related microbial keratitis, but 80–85% cases of AK in the UK, the United States, and other developed Asian countries with high prevalence of CL use are associated with CL use. The incidence is much higher in conventional soft CL users compared to those using daily wear rigid gas permeable lenses or planned replacement soft lenses.
In India, AK is more frequently secondary to trauma and exposure to contaminated water.
Additional risk factors include, use of contaminated water as home water supply, warmer weather and poor socioeconomic conditions. AK has also been reported after surgical trauma including penetrating keratoplasty (PK) and radial keratotomy and laser refractive surgery.
Environmental sources of Acanthamoeba :
Free-living amoebae belonging to Acanthamoeba genus are widely distributed in natural and man-made environments of many parts of the world. The amoebae have been isolated from a wide range of soil and aquatic habitats; they occur in
- Seawater
- Fresh chlorinated and tap water
- Drinking water systems and bottled mineral water
- Thermal recreational waters and swimming pools
- Air-conditioning systems including humidifiers
- Soil , dust and sewage
- Fruits and vegetables
- Healthy, diseased or dead animals
The amoebae have been isolated also from clinical settings and the hospital environment, on surfaces of different equipment and accessories, in water and air-conditioning systems, on surgical instruments, in dental irrigation units, in contact lenses and their cases, and dialyzers.
The developmental forms and life cycle of Acanthamoeba spp.:
Acanthamoeba exists in two morphologic forms:
- Trophozoites (active vegetative form)
- Cyst (dormant form)
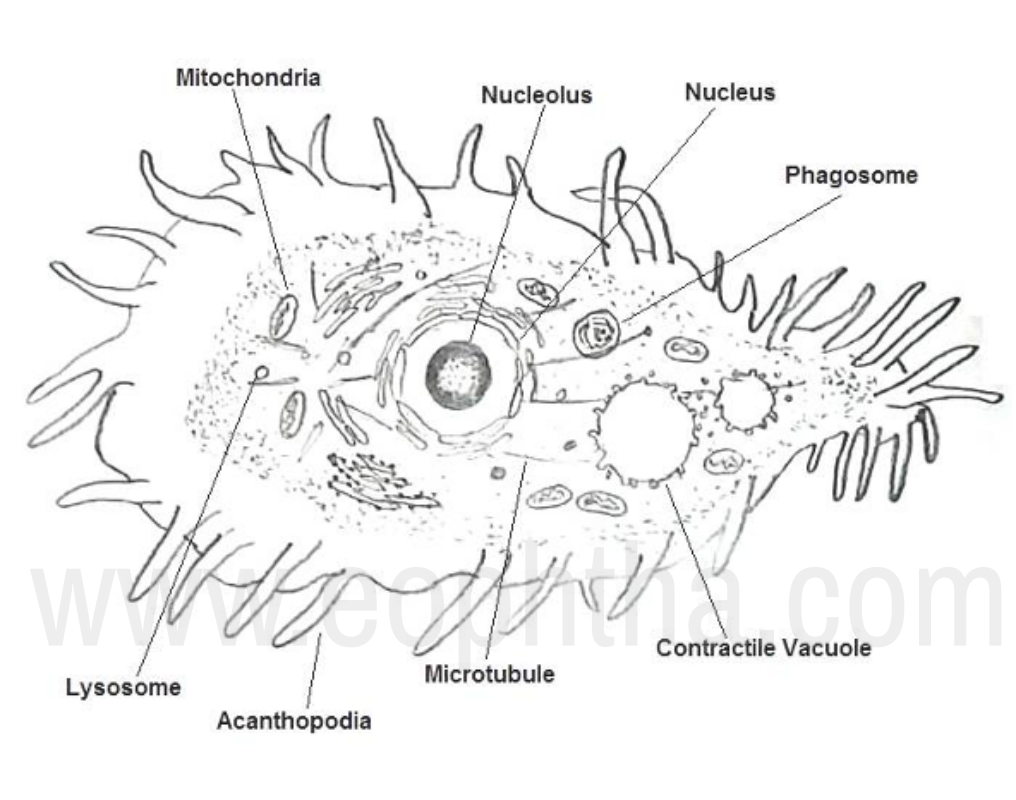

The life cycle of Acanthamoeba is asexual, the reproduction of trophozoite is by binary fission. The trophozoites contain one nucleus with large, central nucleolus (endosome), ectoplasm, and granular endoplasm, with a large contractile vacuole as well as numerous mitochondria and digestive vacuoles. The trophozoite is changing in shape, 15–45μm in size, and moving by cytoplasmic transparent pseudopodia called as acanthopodia.
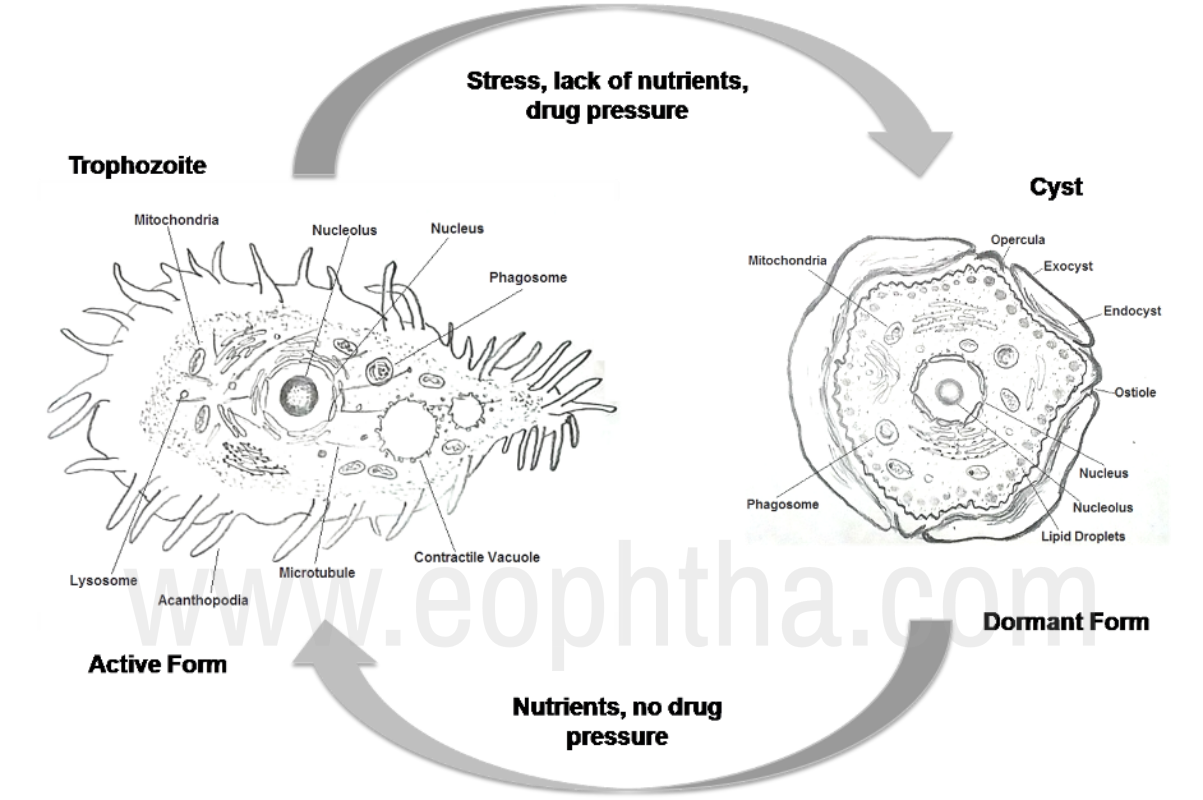
The cyst is smaller, 8-24μm in size, rounded or polygonal in shape, and double-walled, with a rippled outer layer. The outer wall of the cyst, ectocyst, contains lipids and proteins; the inner cyst wall, endocyst contains cellulose that is not present in the trophozoite stage. The two cyst walls contain pores, called ostioles that are covered by plugs, called as opercula. The plugs are removed when trophozoites emerge from cysts during excystation. Trophozoites transform into cyst stages after the growth developmental phase as well as under harmful environmental conditions e.g. extremes in temperature and pH, increased or decreased osmolarity, lack of nutrients, etc.
Classification of Acanthamoeba spp.:
Earlier, the acanthamoeba spp were classified according to morphological criteria. In this classification, the size of cysts and the number of arm-like structures visible within a single cyst in light microscope were mainly taken into consideration. 18 species have been determined and placed in three morphological groups I, II, and III.
Nowadays it is based on genotype associations - the 18S rRNA gene sequence. The species identification is based on a combination of morphological and molecular characterization. At present, 18 or19 genotypes are distinguished for diagnostics and for the characterization of clinical and environmental Acanthamoeba isolates
Pathogenesis:
Pathogenesis of Acanthamoeba keratitis is a multi-factorial process connected with some factors contributing directly and indirectly in the production of diseases in humans.
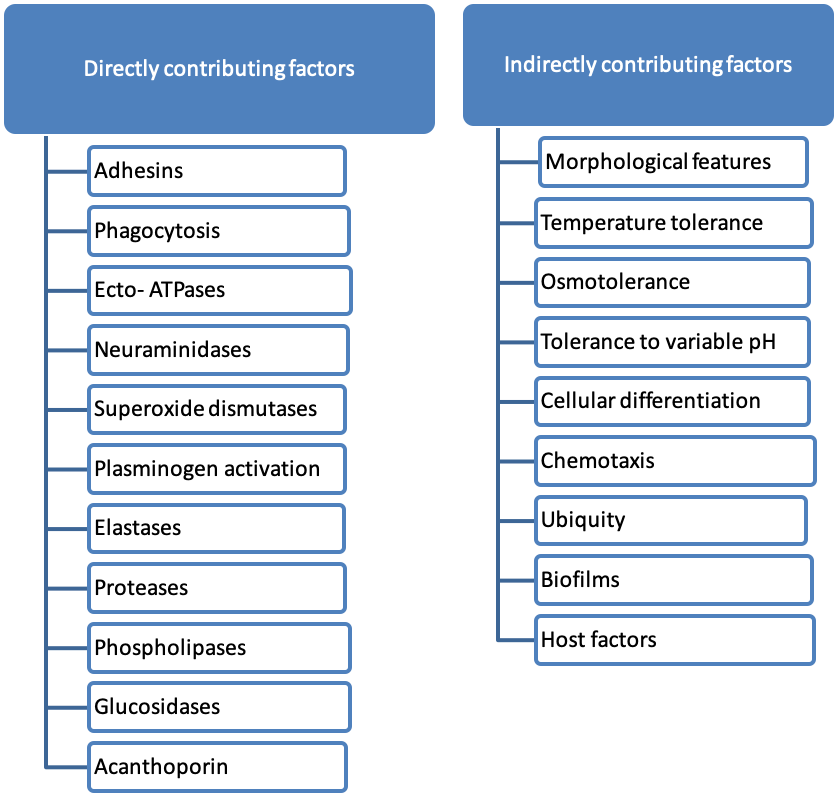
Factors contributing directly to pathogenicity:
Adhesion:Adhesion is an important step in the pathogenic cascades of Acanthamoeba keratitis leading to amoebae crossing the biological barriers.
- Mannose-binding protein
- Laminin-binding protein
are two such adhesins identified in Acanthamoeba. On the host side, parasite binding to specific host cell receptor is not yet fully understood. However Toll-like receptor-4 (TLR-4) contains a docking sitefor Acanthamoeba. The binding of Acanthamoeba to host receptors interferes with the host intracellular signalling pathways and induces cell cycle arrest in the host cells.
Phagocytosis:The primary role of Acanthamoeba phagocytosis is to take up food particles. Several studies have found that Acanthamoeba form food cups or amoebastomes during incubation with the host cells which suggests a role in the pathogenesis.
Ecto-ATPases:Ecto-ATPases are glycoproteins expressed in the plasma membranes. Ecto-ATPases hydrolyze extracellular ATP. The resultant ADP can have toxic effects on the host cells.
Neuraminidase activity:Acanthamoeba exhibits neuraminidase activity which is optimal at pH 5 and at temperatures of 25–30 C. The live amoebae release sialic acid from the host cells and in turn damage the sialic acid-rich corneal epithelium.
Superoxide dismutase:The enzyme superoxide dismutase catalyzes the dismutation of superoxide into oxygen and hydrogen peroxide. Superoxide dismutase plays an important antioxidant role. Two superoxide dismutases have been identified in Acanthamoeba:
- Iron superoxide dismutase
- Copper-zinc superoxide dismutase
They may be potential virulence factors of Acanthamoeba by acting both as anti-oxidants and anti-inflammatory agents.
Acanthamoeba-induced plasminogen activation:Acanthamoeba display plasminogen activator activity to form plasmin, which can activate host proteolytic enzymes, such as pro-matrix metalloproteases which in turn degrade the basement membranes and the extracellular matrix components such as type I and type II collagens, fibronectins and laminin.
Elastase:Acanthamoeba is known to produce elastase which degrade connective tissue proteins such as elastin, fibrinogen, collagen, and proteoglycans. Tissues altered by prior elastase treatment are more susceptible to oxygen radical attack, suggesting their involvement in the pathogenesis and pathophysiology of Acanthamoeba infection.
Proteases:Proteases are degradative enzymes that hydrolyses proteins. Acanthamoeba proteases mainly degrade food substances for feeding purposes. However, pathogenic Acanthamoeba exhibit increased extracellular protease activities to facilitate invasion of the host. Acanthamoeba produce:
- Serine proteases
- Cysteine proteases
- Metalloproteases
Serine proteases facilitate Acanthamoeba invasion of the corneal stroma, leading to secondary reactions such as oedema, necrosis and inflammatory responses.
Phospholipases:Phospholipases cleave phospholipids and thus play a role in membrane disruptions, penetration of host cells, and cell lysis. They also interfere with intracellular signaling pathways. Acanthamoeba phospholipases and lysophospholipases produce host cell damage and affect other cellular functions such as induction of inflammatory responses.
Glycosidases:Glycoside hydrolases catalyze the hydrolysis of glycosides to generate smaller sugars. Glycoside hydrolases are ubiquitous in nature and involved in the degradation of cellulose and in a variety of cellular functions.
Acanthaporin:Acanthaporin, the first pore-forming toxin was described in recent studies. Acanthaporin is cytotoxic for human neuronal cells.
Factors contributing indirectly to pathogenicity:
Morphological features:Acanthamoeba possess spine-like structures known as acanthopodia, which allow them to bind to biological and inert surfaces.
Temperature tolerance, osmotolerance and growth at different pH:Being free-living, Acanthamoeba can withstand various temperatures, osmolarity and pH. Similarly contact with tear film exposes Acanthamoeba to high osmolarity (due to salinity in tears), high temperatures as well as alterations in pH. Acanthamoeba have high levels of heat shock proteins (i.e. HSP60 and HSP70) compared with weaker pathogens. The higher levels of heat shock proteins in Acanthamoeba indicate their involvement in
- Tolerance to hosts stressors
- Virulence
Cellular differentiation:It is the ability of Acanthamoeba to differentiate into a morphologically distinct dormant cyst form or a vegetative trophozoite form. This differentiation depends on environmental conditions. Cysts are resistant to antimicrobial agents as well as extremes in temperatures, pH, osmolarity, desiccation. Acanthamoeba cysts can survive several years while maintaining their pathogenicity. Cellular differentiation represents a major factor in the transmission of Acanthamoeba and recurrence of its infection.
Chemotaxis:Chemotaxis directs amoeba movement according to their environment. This is important as Acanthamoeba moves towards the highest concentration of food molecules, or to flee from poisons. Acanthamoeba exhibits chemosensory responses by moving actively towards the attractant.
Ubiquity:Acanthamoeba has been found in diverse environments. These are one of the most ubiquitous protists and often come into contact with human beings, and given the opportunity (e.g. contact lens wear), can cause serious infections.
Biofilms:Biofilms are microbially-derived sessile communities, which can be formed in aqueous environments as well as on any materials and medical devices including intravenous catheters, contact lenses, scleral buckles, suture material, and intraocular lenses. Biofilms provide niches for Acanthamoeba by providing nutritional requirements as well as resistance to disinfectants.
Host factors:The factors that enable Acanthamoeba to produce disease involve host determinants factors such as host susceptibility, tissue specificity, tear factors, IgA, corneal trauma, as well as environmental factors such as osmolarity.
The above factors are responsible for these three stages:
- Epithelial adhesion and desquamation
- Stromal invasion
- Neuritis
Epithelial Adhesion and Desquamation Ancanthamoeba adheres to healthy epithelium, without a traumatic entry point. The amoebae are able to burrow under epithelial cells, where they cause rapid desquamation.
Stromal Invasion Trophozoites invade the extracellular matrix of stromal cells, gain access to stromal tissue, and induce the classic ring infiltrate.
Neuritis. Trophozoites follow a chemotactic response to corneal neurones and causes apoptosis causing the clinical sign of radial neuritis.
Clinical features:
|
Symptoms: |
Signs: |
|
Redness |
Early: Epithelial irregularities and defect |
|
Grittiness |
Epithelial and anterior stromal infiltrates |
|
Blurring of vision |
Pseudo-dendrites |
|
Photophobia |
Late: Deep stromal infiltrates (Ring infiltrates) |
|
Discharge |
Persistent epithelial defects |
|
Pain which is disproportaionately high |
Radial keratoneuritis |
|
Waxing and waning of symptoms |
Hypopyon |
|
Stromal thinning and perforation |

Figure:Ring infiltrate in a case ofAcanthamoeba Keratitis

Figure:Hypopyon ulcer in a case ofAcanthamoeba Keratitis

Figure:Persistent non-healing ulcer
Complications:
AK can be associated with various extra-corneal complications such as:
Cataract
Cataract is seen in patients with severe and prolonged keratitis. Cataract may form because of
- Toxicity from topical anti Acanthamoeba drugs
- Chronic inflammation
- Corticosteroids
- Vascular thrombosis
Iris atrophy and persistent dilated fixed pupil
This can be attributed to severe inflammation and vascular thrombosis.
Scleral involvement
Scleritis in patients with AK is a painful complication that generally occurs in immunocompetent individuals.
Pathogenesis of scleritis:
- Inflammatory response elicited by dying organisms and degenerating amoebic cyst walls
- AK induced autoimmunity through molecular mimicry
- T cell response from corneal antigen-presenting cells
The clinical picture of scleritis is characterized by:
- Severe deep pain
- Globe tenderness
- Engorgement of episcleral and scleral vessels
- Nodular or diffuse thickening of sclera
The pain of scleritis is usually very severe and was one of the indications of enucleation before the advent of immunosuppressants. For mild scleritis, topical steroids and oral NSAIDs and for severe disease oral steroids and steroid-sparing agents are recommended. The treatment is started with intravenous methyl prednisolone 1 gram daily for 2–3 days along with oral prednisolone 0.5–1 mg/kg/day. Steroid sparing agents such as cyclosporine (3–7.5 mg/kg/day), mycophenolate (usually 1 g twice per day), or azathioprine (usually 100 mg oral daily) are added if not controlled by steroids alone. Patients on systemic corticosteroid or immunosuppressive therapy are given oral antifungal therapy as prophylaxis against scleral invasion by trophozoites
Intraocular spread
In most cases, the parasite remains restricted to the cornea and it is rare to see extra corneal spread. The mechanism of extra-corneal spread in the absence of perforation is unknown.
Diagnosis:
Clinical suspicion is the first and most vital step in the diagnosis of AK. A detailed clinical history reveals risk factors—either contact lens wear in western countries or trauma and contaminated water exposure in developing countries.
Culture remains the gold standard of AK diagnosis, but today several PCR-based techniques are also well established and usually increase sensitivity significantly. Acanthamoeba trophozoites or cysts are easily seen in phase-contrast microscopy. Cysts also exhibit auto-fluorescence
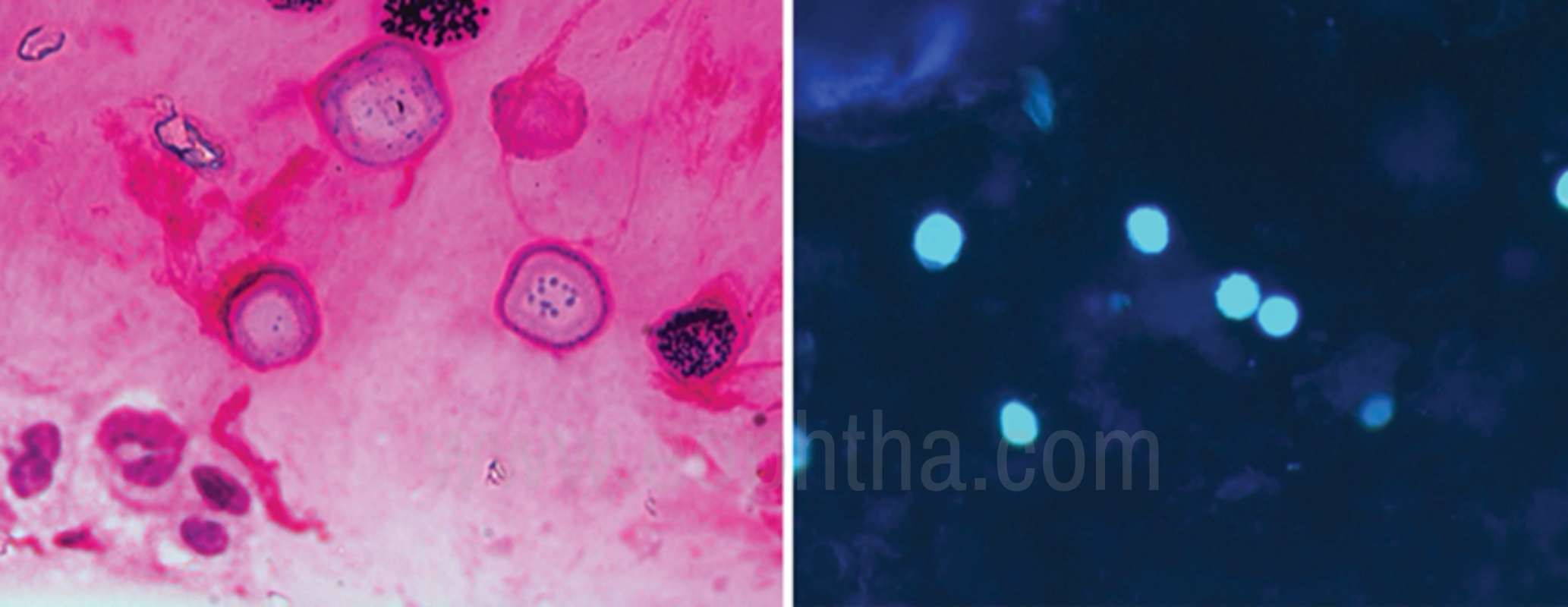
Figure: Gram stain (Right) andCalcoflour white stain (Left) showing Acanthoemoba cysts
Conventional laboratory procedures:Swab samples, tear samples and superficial corneal scrapings are often negative, as the acanthamoeba penetrates deep in the cornea. Contact lens containers, even those of healthy CL wearers, are almost always positive for acanthamoebae. So the detection of acanthamoeba in CL case does not always mean AK. But if the case culture is negative then AK is unlikely.
Sample material preparation:The optimal material for AK diagnosis is a deep corneal scraping or a corneal biopsy stored in 200 lL of sterile saline (amoeba saline* or PBS or 0.9% NaCl) in order to prevent desiccation.
Direct microscopy:In severe infections, amoebae can be detected by direct microscopy (200·–400· magnification) of the original sample. For detailed analysis, phase contrast or interference contrast are particularly useful.
Culture:The material (corneal biopsies or transport medium/contact lenses/swabs) is applied centrally onto a 90 mm 1.5% non-nutrient (NN) agar covered with an overlay (100 lL) of a 24 hours old culture of non-mucous bacteria (e.g. Escherichia coli). Plates are sealed and incubated at 30 C. Amoebae are usually already visible after 24–48 hours. But samples should be observed for up to 2 weeks before giving a negative report. In the absence of NN agar, amoebae can be cultured in a suspension of bacteria in PBS. The culture isolates can be stained with different methods for identification.
Stains:Amoebae have to be cultured prior to staining. The stains commonly used are:
|
Stain |
Staining characteristics |
|
Lactophenol cotton blue (LPCB) |
Cyst walls and nucleus appear intense blue in a light blue stained cytoplasm |
|
Acridine orange |
Cyst appear bright orange on fluorescence microscopy |
|
Calcoflour white |
Cysts appear turquoise green to bluish-white, trophozoite appears reddish-brown |
|
Gomori methanamine silver |
Cysts appear as shining double-walled structures on a dark background |
|
Haematoxyline & eosin (H&E) |
Cysts are visible as double-walled structure on a variably stained background |
|
Modified Trichrome blue (Ryan blue) |
Cysts appear bright pink on a blue background |
|
Gimenez stain |
Cysts appear red-magenta on a greenish-blue background |
|
Giemsa |
Cysts appear blue with a clear halo on a violet background |
|
Immunostains ( Immuno-peroxidase technique IP or indirect fluorescent antibody) |
These are the most sensitive and specific of all stains but are not readily available. Cysts appear blue and trophozoites appear brown |
Confocal microscopy:
In vivo Confocal microscopy (IVCM) is a noninvasive imaging technique that allows direct
visualization of pathogens including Acanthamoeba cysts within the patient’s corneal tissue. Two machines currently in clinical use are scanning slit IVCM (Confoscan, Nidek, Fremont, USA) and laser scanning IVCM (HRT3/RCM, Heidelberg, Germany). The reported sensitivity and specificity of the technique varies between 80% and 100%. IVCM is particularly useful for detecting organisms in deep corneal infiltrates which are not accessible for scraping. IVCM findings can also be correlated to prognosis – the presence of clusters or chains of cysts has been found to be associated with a poor prognosis.
The Acanthamoeba cysts appear as hyper-reflective, spherical structures, well defined because of their double wall; the trophozoites are difficult to distinguish from leukocytes and keratocytes.
Recent advances include tandem scanning confocal microscopy (TCSM), which is considered as more sensitive than either culture or biopsy analysis in Acanthamoeba. This is due to the increased resolution of 1-2 μm laterally and 5–10 μm axially by filtering out reflected light. It can be considered as a first-line method in Acanthamoeba diagnosis where facilities exist.
Molecular methods of diagnosis
Most of the molecular methods for diagnosis of AK are based on amplification of 18S rDNA. Molecular methods have sensitivity similar to conventional microbiology. These are more commonly used for identification of the parasite to subspecies level for understanding pathobiology and epidemiology.
Real-time polymerase chain reaction (rtPCR): PCR amplification has been used since 1996 in detecting Acanthamoeba. It has a similar sensitivity (89.3%) to smear histology, but specificity is a little less. PCR works by amplifying a fragment of the 18S rRNA gene using the JDP1 and JDP2 primers. Amplicons thus formed are visualized by agarose- gel electrophoresis.
Loop-mediated isothermal amplification: A highly specific DNA amplification technique which amplifies target DNA sequences under isothermal conditions. 18S rDNA gene is used for specific detection of Acanthamoeba from corneal scraping samples.
H1 nuclearmagnetic resonance (NMR) spectroscopy :
It is one of the recent advances in diagnosis of Acanthamoeba in vitro. It works by profiling the biochemical signature of different strains of the organism. Some studies predict that this method could yield a high level of sensitivity and specificity. Its application would be similar to PCR
testing, so further study is needed to see how it compares to PCR in terms of diagnostic accuracy and time efficiency.
Management of acanthamoeba keratitis:
Treatment of acanthamoeba keratitis can be divided into:
- Medical management
- Surgical management
Medical management:
The goals of medical therapy include the eradication of viable cysts and trophozoites and rapid resolution of the associated inflammatory response. Various drugs used for AK are-
|
Group |
Drugs |
Dose |
|
Biguanides |
Chlorhexidine Polyhexamethylenebuiguinide |
0.02%-0.2% 0.02%-0.06% |
|
Diamidines |
Propamindine isethionate Hexamidine |
0.1% 0.1% |
|
Azoles |
Voriconazole |
100 mg/day orally |
|
Aminoglycoside |
Neomycin |
1% |
The mainstay agents that are used as a first-line treatment for Acanthamoeba keratitis are diamidines (propamidine, hexamidine) and biguanides (polyhexamethylene biguanide (PHMB), chlorhexidine), which have the most cysticidal effect. Chlorhexidine and PHMB both contain highly charged positive molecules that bind to the mucopolysaccharide plug of the ostiole resulting in penetration of the amoeba. The drug then binds to the phospholipid bilayer of the cell membrane which is negatively charged resulting in damage, cell lysis, and death.
PHMB is the most preferred agent in monotherapy or in combination with other drugs. Chlorhexidine can also be used in monotherapy, but it is much more effective in combined treatment. Propamidine is used in combination with one of biguanides. Neomycin is ineffective against cysts so never used as monotherapy.
The drops are administered every hour, day, and night, for 48 h initially, followed by hourly drops by day till the clinical signs of resolution are observed. Typical regimes need to be tapered around 6 months. Recent studies have found triazoles effective as an adjunct to biguanide and diamidine therapy in refractory cases. They have been used empirically in AK either as topical voriconazole 1% or as oral 100mg as an adjuvant to standard therapy.
Role of corticosteroids:
Topical steroids may be added once a sterilization period of antimicrobial therapy has been completed. Corticosteroids help control inflammation, but they lead to the transformation of cyst forms into trophozoites with the consequent risk of worsening or recurrence of clinical disease.
Indications of steroid use in AK are:
- Occurrence and progressive increase in deep vascularization of cornea
- Inflammatory complications of AK – scleritis, anterior chamber inflammation, persistent chronic keratitis
- Severe out of proportion pain
Antiamoebic therapy is maintained throughout and continued after the steroids have withdrawn.
Surgical management:
If the topical pharmacotherapy fails, surgical interventions are indicated such as :
- Collagen cross-linking
- Laser phototherapeutic keratectomy (PTK)
- Bi-pedicle conjunctival flap surgery
- Cryopreserved amniotic membrane graft (AMG)
- Cyanoacrylate glue with bandage contact lens
- Corneal transplantation
- Therapeutic keratoplasty
- Optical keratoplasty
Collagen cross-linking:
Cross-linking procedure using riboflavin and UV-A (ultraviolet light A, 365nm wavelength) is useful for stabilization of corneal melting. The collagen stabilising effect prevents further tissue damage and isolates and prevents reproduction of the amoebae. It has also a direct antimicrobial effect that is due to the effect of UV light interacting with riboflavin as the chromophore. It damages both the DNA and RNA of pathogens. Photoactivated chromophore for infectious keratitis (PACK)-CXL is an excellant alternative to standard antibiotic therapy in treating AK where available.
Laser phototherapeutic keratectomy (PTK):
Corneal abscesses upto anterior to mid stroma can be removed using PTK. Its application to deeper or more widespread infiltration may be limited.
Bipedicle conjunctival flap (CF) and cryopreserved amniotic membrane graft (AMG):
These procedures have been reported to be effective in AK. They restore ocular surface integrity and provide metabolic and mechanical support for corneal healing in early cases with mild to moderate corneal thinning.
Cyanoacrylate glue with bandage contact lens:
This is done in cases of small perforations. Cyanoacrylate glue acts as anti-microbial as well as provide mechanical support to the underlying corneal stroma. Limitation is that it can only be used for small perforations upto 2mm in size.
Therapeutic keratoplasty:
-
- Full thickness penetrating keratoplasty (PK)
- Deep anterior lamellar keratoplasty (DALK)
Indicated in cases of:
- Large infiltrate extending or threatening to involve limbus
- Worsening on medical treatment
- Gross thinning or actual perforation
Full thickness penetrating keratoplasty is done in cases with impending or frank corneal perforation. DALK is preferred nowadays as it has a high cure rate along with less chances of rejection. All patients undergoing surgery should be started on anti-amoeba therapy which should be continued for 3 weeks to 3 months post op.
Optical keratoplasty:
It is performed after resolution of active keratitis for visual rehabilitation in cases with remnant scarring of cornea. Studies shows an excellent prognosis for both graft survival and visual outcome.

Figure:Status post cyanoacrylate glue + BCL

Figure:Status post-therapeutic keratoplasty
Differential diagnosis:
AK is most commonly confused with:
- HSV keratitis (in early stages of disease)
- Pseudomonas keratitis
- Fungal keratitis (in later stage)
AK can be differentiated from these entities by:
|
Others |
AK |
|
HSV- Dendrites, endothelium involvement in some cases |
Pseudo-dendritiform epitheliopathy, epithelium defects without terminal knots, endothelium is not involved |
|
Bacterial – Single large abscess, anterior chamber reaction present |
Usually restricted to cornea, absence of anterior chamber activity, stromal infiltrates are usually multifocal (ring infiltrate) |
|
Fungal – satellite lesions, feathery margins, dry-looking infiltrate |
Usually restricted to cornea, clear epithelium defects, perineural stromal infiltrates, |
To conclude, Acanthamoeba is a rare cause of keratitis. The outcome of medical management is good if the disease is diagnosed early and definitive treatment is initiated. If misdiagnosed or mistreated can lead to blinding complications.
References:
1.Jones DB, Visvesvara GS, Robinson NM. Acanthamoeba polyphaga keratitis and Acenthamoeba uveitis associated with fatal meningoencephalitis. Trans Ophthalmol Soc U K 1975;95:22132. 2. Sharma S, Srinivasan M, George C. Acanthamoeba keratitis in non contact lens wearers. Arch Ophthalmol 1990;108:6768. 3. Sharma S, Srinivasan M, George C. Diagnosis of Acanthamoeba keratitis – A report of four cases and review of literature. Indian J Ophthalmol 1990;38:506. 4. Illingworth CD, Cook SD. Acanthamoeba keratitis. Surv Ophthalmol 1998;42:493 508. 5. Hammersmith KM. Diagnosis and management of Acanthamoeba keratitis. Curr Opin Ophthalmol 2006;17:32731. 6. Awwad ST, Petroll WM, McCulley JP, Cavanagh HD. Updates in Acanthamoeba keratitis. Eye Contact Lens 2007;33:18. 7. Dart JK, Saw VP, Kilvington S. Acanthamoeba keratitis: Diagnosis and treatment update 2009. Am J Ophthalmol 2009;148:4879900. 8. Maycock NJ, Jayaswal R. Update on Acanthamoeba keratitis: Diagnosis, treatment, and outcomes. Cornea 2016;35:71320. 9. Chin J, Young AL, Hui M, Jhanji V. Acanthamoeba keratitis: 10year study at a tertiary eye care center in Hong Kong. Cont Lens Anterior Eye 2015;38:99103. 10. Qian Y, Meisler DM, Langston RH, Jeng BH. Clinical experience with Acanthamoeba keratitis at the cole eye institute, 1999 2008. Cornea 2010;29:101621. 11. Tanhehco T, Colby K. The clinical experience of Acanthamoeba keratitis at a tertiary care eye hospital. Cornea 2010;29:100510. 12. Gopinathan U, Sharma S, Garg P, Rao GN. Review of epidemiological features, microbiological diagnosis and treatment outcome of microbial keratitis: Experience of over a decade. Indian J Ophthalmol 2009;57:2739. 13. Basak SK, Basak S, Mohanta A, Bhowmick A. Epidemiological and microbiological diagnosis of suppurative keratitis in Gangetic West Bengal, Eastern India. Indian J Ophthalmol 2005;53:17 22. 14. Lalitha P, Lin CC, Srinivasan M, Mascarenhas J, Prajna NV, Keenan JD, et al. Acanthamoeba keratitis in South India: A longitudinal analysis of epidemics. Ophthalmic Epidemiol 2012;19:1115. 15. Mascarenhas J, Lalitha P, Prajna NV, Srinivasan M, Das M, D’Silva SS, et al. Acanthamoeba, fungal, and bacterial keratitis: A comparison of risk factors and clinical features. Am J Ophthalmol 2014;157:5662. 16. Sharma S, Garg P, Rao GN. Patient characteristics, diagnosis, and treatment of noncontact lens related Acanthamoeba keratitis. Br J Ophthalmol 2000;84:11038. 17. Manikandan P, Bhaskar M, Revathy R, John RK, Narendran V, Panneerselvam K, et al. Acanthamoeba keratitis –A six year epidemiological review from a tertiary care eye hospital in South India. Indian J Med Microbiol 2004;22:22630. 18. Bashir G, Rizwi A, Shah A, Shakeel S, Fazili T. Acanthamoeba keratitis in Kashmir. Indian J Pathol Microbiol 2005;48:417. 19. Kilvington S, Gray T, Dart J, Morlet N, Beeching JR, Frazer DG, et al. Acanthamoeba keratitis: The role of domestic tap water contamination in the United Kingdom. Invest Ophthalmol Vis Sci 2004;45:165 9. 20. Houang E, Lam D, Fan D, Seal D. Microbial keratitis in Hong Kong: Relationship to climate, environment and contact lens disinfection. Trans R Soc Trop Med Hyg 2001;95:361 7. 21. Jacob Lorenzo-Morales, Naveed A. Khan, and Julia Walochnik An update on Acanthamoeba keratitis: diagnosis, pathogenesis and treatment. Parasite 2015, 22, 10 22. Benjamin Clarke, Arti Sinha, Dipak N. Parmar, and Evripidis Sykakis. Advances in the Diagnosis and Treatment of Acanthamoeba Keratitis Journal of Ophthalmology Volume 2012: 484892. 23. Garg P, Kalra P, Joseph J. Non-contact lens related Acanthamoeba keratitis. Indian J Ophthalmol 2017;65:1079-86.