
Introduction:
While there are several instruments in ophthalmological practice, lenses form an inseparable part of an ophthalmologist’s arsenal. Available in various sizes and shapes, they are crucial in aiding the visualization of remote areas of the eye and facilitate therapeutic interventions in those areas which would be next to impossible to even imagine without their availability. Harnessing the unlimited potential of optics, it allows an ophthalmologist to play with the most dynamic form of energy, light, provided he behold sound and in-depth knowledge about the lens. This write-up aims at helping one acquire this knowledge and employ them for a successful practice.
Lens: A piece of glass or other transparent material with curved sides for concentrating or dispersing light rays. (Lexico Oxford Dictionary)
Classification of lenses (Based on their utility)
Lens for the anterior segment:
Lens for posterior segment
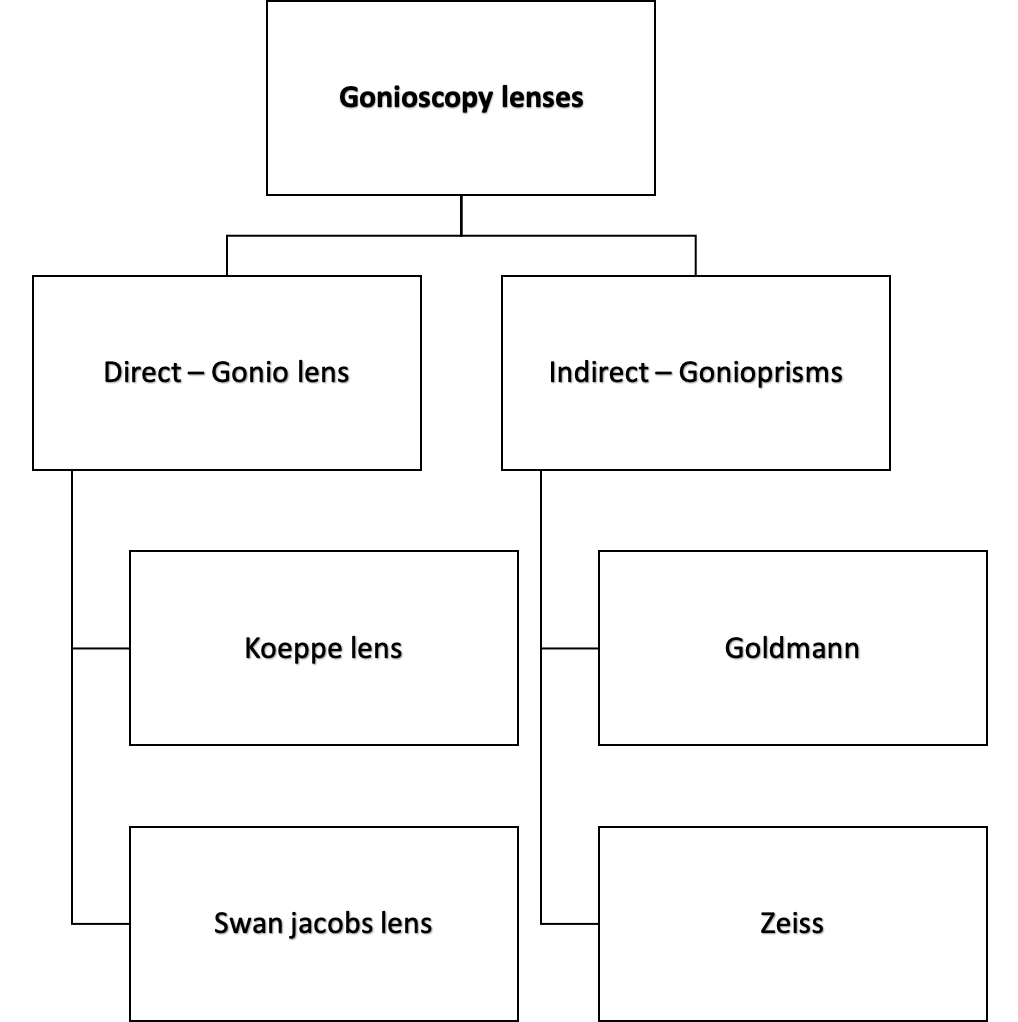
Gonioscopy
Principles and Optics
- The critical angle for the cornea-air interface is approximately 46 degrees.
- Total internal reflection prevents direct visualization of angle in nearly all eyes.
- The incident angle of light- reflected from the angle is greater than the critical angle at the cornea–air interface.
Total internal reflection is overcome by eliminating the cornea-air interface by
- Goniolenses using contact lenses –to examine the anatomy of the angle in the direct method
- Gonioprisms/mirror and viscous coupling solution or tears in the indirect method
As the index of refraction of a contact lens approaches that of the cornea, there is minimal refraction at the interface of these two media, which eliminates the optical effect of the front corneal surface. Thus light rays from the anterior chamber angle enter the contact lens and are then made to pass through the new contact lens-air interface.∠a
METHODS
Two methods:
Indirect gonioscopy: Using mirrors, the angle is examined with reflected light.
Direct gonioscopy: Look directly at the angle with lenses.
|
Table 1: Gonioprisms (Indirect) |
|
|
Required coupling agents |
Not requiring coupling agents |
|
Goldmann single mirror |
Zeiss 4-mirror gonioprism |
|
Goldmann 2 mirror gonioprism |
Posner Gonioprism |
|
Goldmann 3 mirror gonioprism |
Sussman Lens |
|
Allen Thorpe gonioprism |
Ritch Trabeculoplasty laser lens |
|
Token Goniopri |
|
Gonioprisms requiring coupling agents
1. Goldmann single mirror gonioprism
- Prototype diagnostic gonioprism.
- Mirror inclined at 62° from plano front surface.
- It needs to be rotated 3 times to examine the whole angle.
- Mirror Height -12 mm
- Central good diameter -12 mm
- Posterior Radius of curvature -7.38 mm
2. Goldmann two mirror gonioprism
- Both mirrors inclined at 62°
- Needs to be rotated once to examine the whole angle
3. Goldmann three-mirror gonioprism
A. Gonioscopy mirror: Inclination of 59°
- Smallest
- Dome-shaped upper border
- The broad area of contact with cornea (12 mm)
- May artificially close the angle under pressure
B. Equatorial mirror: Inclined at 67°
- Largest
- Oblong shaped
- Examine Pars plana of the ciliary body
- Posterior pole to the equator
C. Peripheral mirror: Inclined at 73 °
- Intermediate-size
- Square shaped
- Examine from equator to ora serrata
D. Allen Thorpe gonioprism
- 4 prisms instead of mirrors
- Allows examination of the whole angle without rotating the prisms
- Suspended by a frame
Advantages of Goldmann gonioprisms
- Easy to use
- Excellent view
- The peripheral retina can be seen
- Stabilizes the globe
- Can be used in Argon Laser trabeculoplasty
Disadvantages of Goldmann gonioprisms
- Only 1 mirror for gonio-lens to be rotated by 360°
- Cannot be used for indentation
- In the case of 3 mirror lens, a broad area of contact with cornea may cause artefactual closure of angle.
Gonioprismsnot requiring coupling agents
1. Zeiss 4- mirror Gonioprism
- 4 identical mirrors angled at 64°
- On a UNGER HOLDER
- A small area of contact with the cornea (9mm)
- Indentation gonioscopy can be performed
|
Table 3: Advantages of Zeiss 4 mirror prisms |
|
|
Advantages |
Disadvantages |
|
Easy to perform |
|
|
All 4 quadrants visible at same time |
Difficult to master |
|
Rotation of 11 degrees covers the area between the mirrors |
Does not stabilize the globe |
|
Indentation gonioscopy |
May open the angle artefactually if pressure is applied |
|
Coupling material not required, thus fundus viewing and photography possible |
|
2. Posner Gonioprism
- Similar to Zeiss
- Made of plastic instead of glass
- Has a fixed handle
3.Sussman lens
- Similar to Zeiss but has no handle
4. Tokel Gonioprism
- Single mirror lens
- Broader viewing area than Goldmann single mirror lens
- A convex anterior face that provides slight magnification
- For delivery of Laser to angle
5. Ritch Trabeculoplasty laser lens
- 2 mirrors tilted at 59° to see theinferior angle
- 2 mirrors at 64° to view the superior angle
- A convex button in front of a 59° mirror and a 64° mirror for extra magnification and laser treatment
Goniolenses
Koeppe lens
- Prototype diagnostic lens
- Available in several sizes
- Most commonly used lens
- for diagnostic direct gonio.
Huskins Barkan lens
- Prototype surgical goniolens
- Used for Goniotomy
Thorpe Goniolens
- Surgical and diagnostic lens for operating rooms.
Swan jacobs lens
- Surgical goniolens
- Used in children
Richardson Shaffer’s lens
- Small lens for use in infants
Worth goniolens
- It anchors to the cornea by the partial vacuum
Sieback goniolens
- Tiny goniolens which floats on the cornea
Gonioscopy Assisted Laser Delivery
Two types of laser lenses are available to assist in slit lamp delivery of photocoagulation:
1. Plano-concave lenses
- An erect image
- High resolution of small retinal area.
- Mirrors angulated at 59°, 69° and 73°
2. High plus power lenses(indirect lens)
- An inverted image
- Mild loss of fine resolution
- A wide field of view - very suitable for PRP
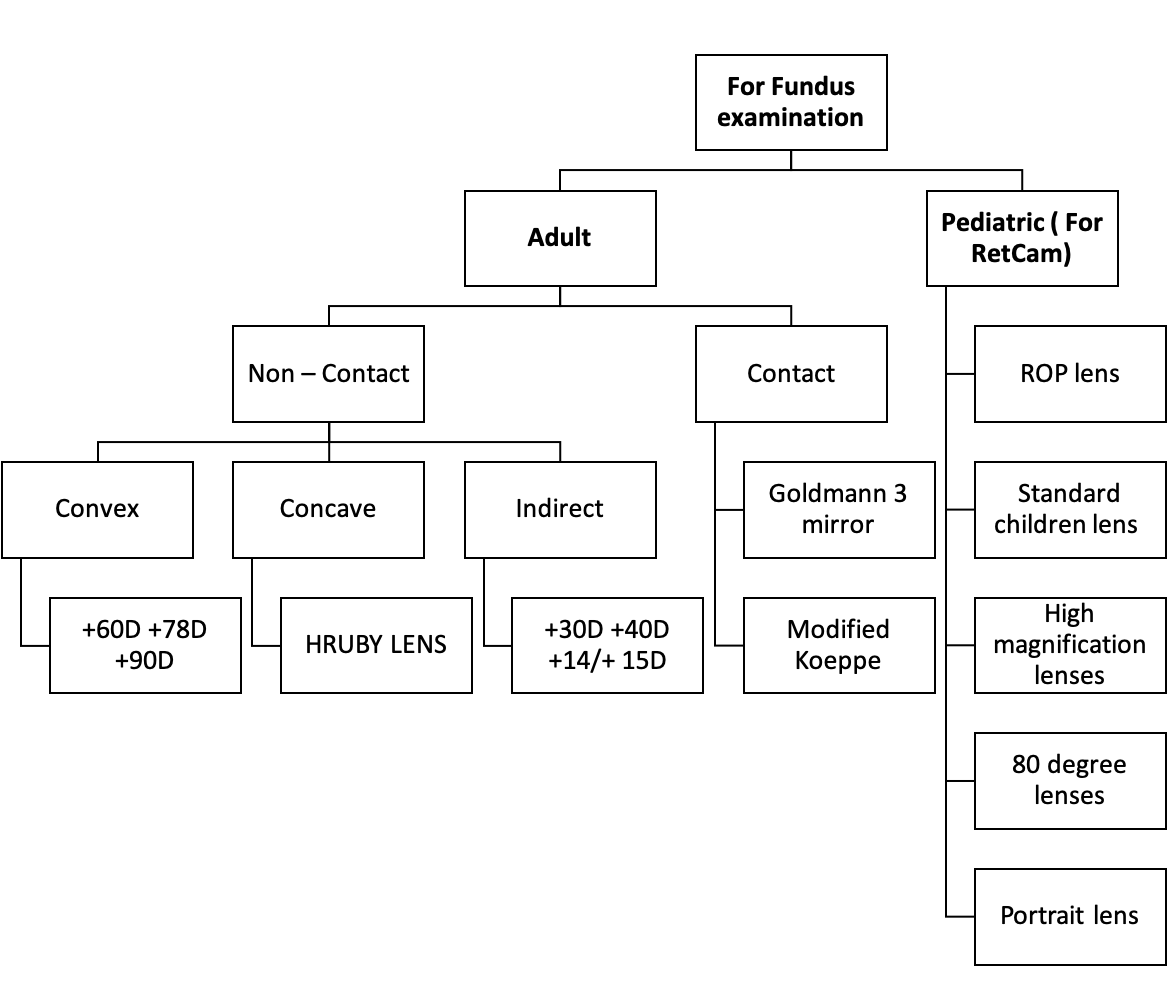
Lenses for Fundus examination:
- Examination of the retina by Slit lamp and Volk double aspheric lenses is called indirect fundus biomicroscopy
- Volk's 60D,78D, and 90D fundus lenses with slit lamp indirect ophthalmoscopy as a standard diagnostic procedure for comprehensive fundus evaluation.
- Double aspheric lenses
- Optics of indirect fundus biomicroscopy is similar to that of indirect ophthalmoscopy.The imageformed is real, inverted, laterally reversed.
Advantages
- Larger field of retina visible
- Lesser distortion of the image of the retina
- Easier to examine, if the patient ‘s eye movements are present and with high spherical or astigmatic refractive errors.
- Easy visualization of retina anterior to equator, where most retinal holes and degenerations exist.
- It gives a 3D stereoscopic view of the retina with considerable depth of focus
- Useful in hazy media because of its bright light and optical property
Disadvantages
- Magnification in indirect ophthalmoscopy is 5 times
- Visualization difficult with very small pupils
- Patient usually more uncomfortable with intense light and scleral indentation
- Reflex sneezing on exposure to bright light
- Requires extensive practice in technique
Technique
- The patient’s pupil may be dilated and background lights dimmed as for direct ophthalmoscopy.
- The patient is positioned comfortably at the slit lamp.
- The slit lamp viewing the piece and the light column are kept at an angle of 90°.
- Set illumination angle coaxial with the slit lamp-viewing system
- The illumination is kept low, the slit beam at a width of 1-2 mm and length of 5-10mm
- Magnification preferably set at 10× initially or 16x.
- The beam is focused on the patient’s pupil and the +78 or +90 D condensing lens aligned at around 5-10 mm from the patient’s cornea.
- The slit lamp is then pulled backwards gradually towards the examiner until the fundal glow is visualized.
- Reflections can be reduced by slightly tilting the lens
- As with indirect ophthalmoscopy, the image from a non-contact Volk Lens slit-lamp biomicroscopic examination is inverted and laterally reversed.
- To view the peripheral retina, ask the patient to look into appropriate positions of gaze as with standard indirect ophthalmoscopy
- Magnification = Power of eye x magnification of slit lamp/ Power of the lens
- Thus, magnification is inversely proportional while, the field of view is directly proportional to the power of the lens.
Stereopsis = Magnification / 4 .
Field of view = (D.P. of the lens x 2 )
Principle of Indirect Ophthalmoscopy
To make the eye highly myopic by placing a strong convex lens in front of it.
|
Table 4: Various lenses for fundus biomicroscopy and their features |
|||
|
Lens |
Image Magnification |
Field of View (static/dynamic/degrees) |
Working Distance(mm) |
|
90D |
0.76 |
74/89 |
7 |
|
60D |
1.15 |
68/81 |
13 |
|
Super66 |
1.0 |
89/96 |
11 |
|
78D |
0.93 |
81/97 |
8 |
90 D lens
- The original Volk 90D lens started the slit lamp examination.
- Relatively wide field of view with a good resolution
- Real inverted image
- Salient features
- General diagnosis and small pupil examinations.
- It features a small 26mm diameter ring that is ideal for dynamic fundoscopy.
- The Volk 90D has very good small pupil capabilities, making it ideal for a quick look at the posterior pole.
- The working distance from the cornea is 6.5mm.

Figure: Lens used in Fundus Biomicroscopy A. + 60 D lens, B. +30D lens, C. +90D; Lens used in indirect ophthalmoscopy D. + 30D and E. + 20D
+ 60D
- High Magnification Views of the Posterior Pole.
- High magnification lens for detailed optic disc and macula imaging.
- Ideal diameter for use in the orbital area. (Its 31mm diameter allows a wide field of view and facilitates easy handling within the orbital area.)
- The working distance from the cornea is 11mm.
+78D
- The Double Aspheric 78D is excellent for viewing optic discs.
- The ideal balance of magnification and field of view.
- The working distance from the cornea is 7mm.
Advantages:
-
Stereoscopic, three-dimensional view of the retina- Binocular viewing through the slit-lamp.
-
Better image achieved when viewing through media opacities - Cataract.
-
Allows for manipulation of image- Slit-lamp magnification& filters.
-
Image size less affected by patient refractive error.
Hruby lens
- Plano-concave lens with dioptric power of -58.6D, which neutralizes the optical power of the eye (+ 60 D)
- To be placed 10-12 mm in front of the patient’s cornea.
- The image formed: virtual, erect image 18mm in front of the patient’s retina
Disadvantages
- Low magnification 5-8° (just about 1 disc diameter)
- A small field, cannot visualize beyond the equator
- Precise patient fixation required
- Hence it is not ideal for screening posterior fundus
Indirect Ophthalmoscope Lenses
- BIO condensing lenses (Handheld lenses )
- Biconvex, aspheric designs with one surface more curved than the other.
- The less curved surface toward the patient’s eye (silver).
- The hand-held lens acts both as:-
- 1.A condensing lens for the illuminating system.
- 2. A lens for forming an inverted image of the retina in space
- The technique is called Indirect because the fundus is seen through a condensing lens.
- The image is formed close to the principal focus of the lens, between the lens and the observer.
- The condensing lens is a powerful convex lens (the usual power used is +14, + 20,and + 33 D )
- The power of the condensing lens determines:-
- Retinal Magnification
- Field of view
- Stereopsis.
+30 D lens
- The high dioptric power lens (30D) has the highest magnification
- Least magnification of the retina, 60/30 = 2.
- Stereopsis is half that of the normal, 2/4= 1/2
- The field of view is generally the largest = (60°, 30° x 2 ).
- Used to obtain a panoramic view when detail and stereopsis are not as important and used with a small pupil.
+20 D lens
- The middle dioptric power lens of (20D).
- The retinal magnification = 60/20 = X3
- The stereopsis is 3/4 that of the normal.
- The field of view is 40° (20x 2 ).
- 20D lens most widely used, since it provides an adequate field of view, stereopsis, and magnification.
|
Table 5: Various lenses for IDO and their features |
||||
|
Lens power(D) |
Magnification |
Field of view |
Stereopsis |
Working distance from the cornea |
|
+30 |
2x |
60 degree |
½ |
26mm |
|
+20 |
3.25x |
40 degree |
¾ |
47mm |
|
+14/+15 |
4.17x |
30 degree |
1 |
72mm |
+15 D lens
- The low dioptric power lens of 14 or 15D.
- The retinal magnification = 60/15 = X4.
- The stereopsis is full ( 4/4 ).
- The field of view is 30° (15x2 ).
- Most useful for a detailed view of the macula or optic disc or for determining the elevation of the retina in shallow retinal detachment.
Contact lens biomicroscopy of the fundus
Combines stereopsis, high illumination, and high magnification with advantages of the slit beam
- Modified Koeppe’s lens.
- Goldmann’ s three-mirror contact lens
- Widefield (panfundoscopic) indirect contact lenses
1. Modified Koeppe’s lens
- Posterior fundus contact lens
- Used to examine the posterior segment
- Virtual and erect image
2. Goldmann’ S Three Mirror Contact Lens
A central contact lens with 3 mirrors placed in the cone, each with different angles of inclination
1. The central contact lens for posterior pole and vitreous
2. Mirror inclined at 73 ° - the area around the posterior pole
3. Mirror inclined at 67 ° - equatorial fundus
4. Mirror inclined at 59 ° - anterior peripheral fundus including ora serrata and pars plana
Technique
1. Dilate pupils
2. Instill topical anesthetic drops
3. Insert coupling fluid into a cup of contact lens but do not overfill
4. Ask the patient to look up, insert the inferior rim of the lens into lower fornix and press it quickly against the cornea
5. Always tilt illumination column except when viewing 12 o'clock position in the fundus (i.e., with the mirror at 6 o’clock)
6. When viewing different positions of the peripheral retina, rotate the axis of the beam so that it is always at right angles to the mirror
7. To visualize entire fundus, rotate lens for 360 degrees using the 59°, 67°, and 73° tilted mirrors to give views of the peripheral retina, the equatorial fundus and the area around the posterior pole, respectively
8. To obtain a more peripheral view of the retina, tilt the lens to the opposite side, and ask the patient to move the eyes to the same side. e.g-to obtain a more peripheral view of 12 o’clock position (with the mirror at 6 o’clock), tilt the lens down and ask the patient to lookup
9. Examine the vitreous cavity with a central lens, using a horizontal and a vertical slit – beam and then examine the posterior pole
3. Widefield (Panfundoscopic) indirect contact lenses
- Field view up to 130 degrees
- For fundus examination and laser photocoagulation
- Inverted image
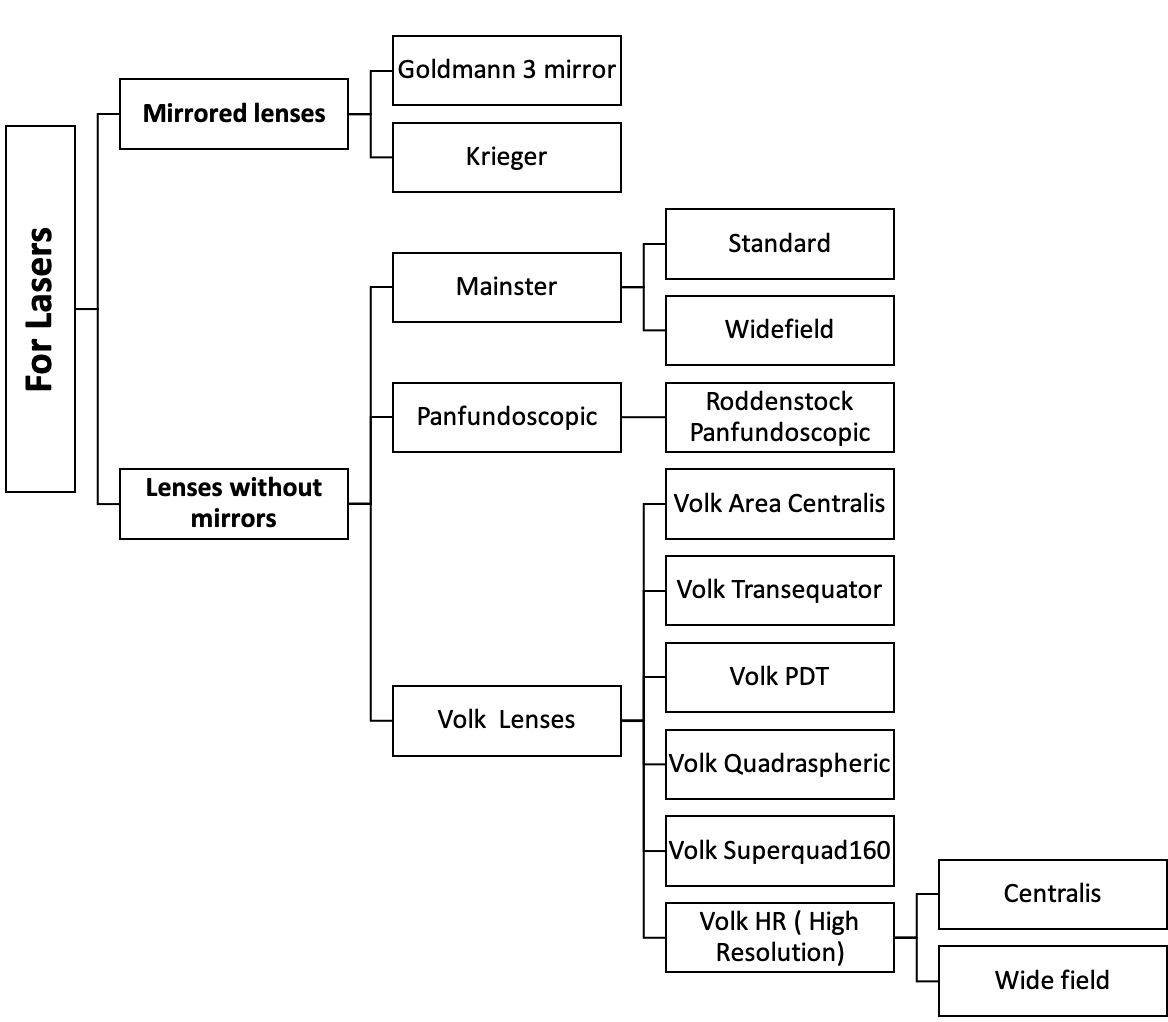
LENS FOR LASERS
Common characteristics of laser lenses
- Concave posterior surface conforming to the corneal curvature and a
- The flat or convex anterior surface
- Planar mirrors allowing observation of the anterior chamber angle or peripheral retina.
- A prism to allow visualization of the mid-periphery of the retina.
- A flange to stabilize the lens and prevent blinking
- Knurled edge to facilitate lens manipulation.
- Laser lenses generally consist of a conical PMMA or aluminum shell
- Glass anterior surface, lenticular elements, and mirrors.
Antireflection coatings
- Usually applied to each optical surface in a laser lens that reduces reflected white light (from the slit lamp source) that could decrease contrast or the slit lamp image, and laser light (from the treatment beam) that could pose a potential hazard to an observer standing behind the laser operator.
- The hazard distance is 7 meters for an uncoated lens and 1.6 meters for a coated lens.
- Most laser lenses use broad-spectrum, multilayer, antireflection coatings that reduce reflected light between 400 nm and 700 nm from approx 4 % to < 1%.
Mirror lenses
- High magnification and high resolution
- Only a small part of the fundus or chamber angle can be viewed at any one time.
- Therefore, the mirrors at various degrees of inclinations are necessary.E.g. Goldmann 3 mirror lenses.The image formed in the Goldmann 3 mirror lens is the mirror image of the area focused.
Lenses without Mirrors
- The field of view may be increased to a variable extent by the use of biconcave contact lenses based on the simple Goldman lens (without mirrors).
- Another different way of increasing the field of view involves using contact lenses based on the EL Bayadi lens. Eg- Rodenstock Panfundoscope and Mainster lens
- All wide-angle systems of this category are derived from the principle of indirect ophthalmoscopy.
- Large and inverted field of view.
- Both the panfundoscope and the Mainster lenses produce inverted real images.
|
Table 6 : Characteristic of focal laser and PRP lenses |
|||
|
Parameter |
Goldman |
Panfundoscopic |
Mainster |
|
Anterior surface |
Flat |
Convex spherical |
Convex aspherical |
|
Image type |
Virtual erect |
Real inverted |
Real inverted |
|
Power |
-67 |
+85 |
+61 |
|
Lateral magnification |
+0.93 |
-0.71 |
-0.96 |
|
Relative magnification |
1.00 |
0.76 |
1.03 |
|
Axial magnification |
0.86 |
0.51 |
0.92 |
|
Field of view |
+/-180 |
+/-600 |
+/-450 |
|
Working field of view(with 150 tilting) |
+/-380 |
+/-700 |
+/-600 |
|
Spot size setting(microns) |
|||
|
100 |
108 |
141 |
105 |
|
200 |
216 |
282 |
210 |
|
500 |
541 |
704 |
524 |
|
1000 |
1081 |
1409 |
1048 |
Goldmann Lens
- Single mirror inclined at 62 degrees or 3 mirrors with gonio mirror at 59o
- Rotated 360 degrees to view angles structures
- Flat anterior surface
- Erect virtual image near the posterior surface of the lens
- Limited field of view without rotation
Yannuzzi fundus lens (Krieger lens )
- Modification of an earlier model developed by Krieger in 1966
- Designed to facilitate macular photocoagulation
- The concave corneal surface which is steeper and of greater diameter,
- Has better optics than a simple Goldmann fundus lens.
- Allows posterior lens pressure to be transmitted to the sclera without distorting the cornea.
- Erect, virtually located in the anterior vitreous humor.
Volk Area Centralis Lens
- Indirect contact lens
- A good field of view 70/84 degrees
- Excellent magnification 1.06x.
- Laser spot magnification is 0.94x.
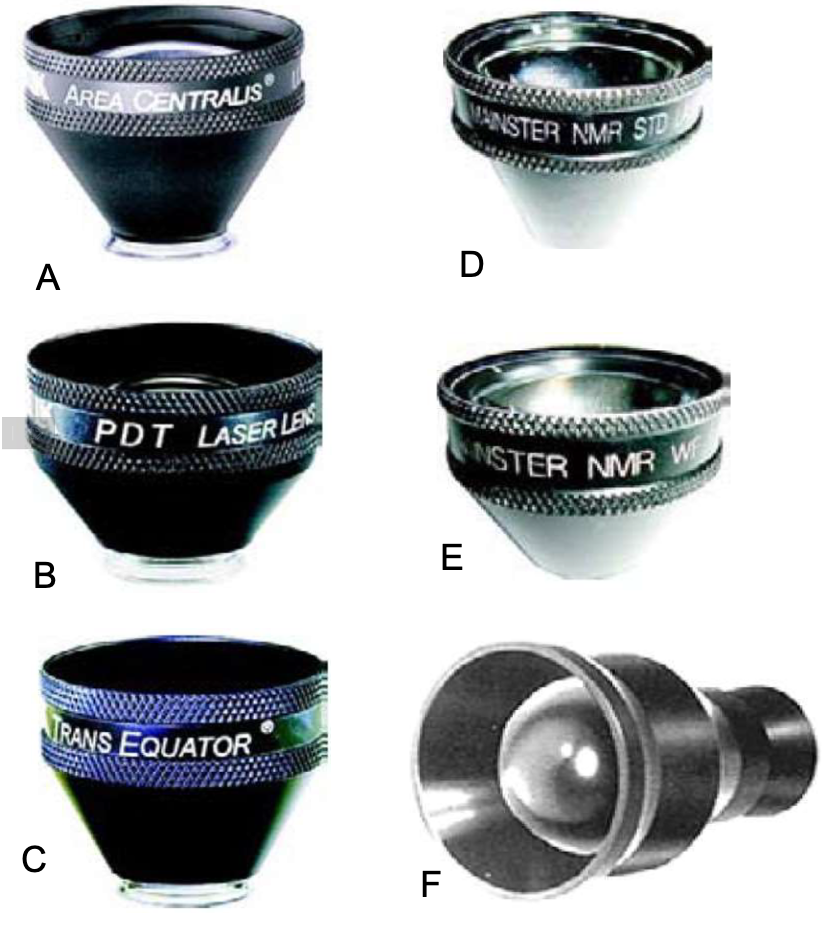
Lens for lasers A. Volk Area Centralis Lens; B. Volk PDT Lens; C. Volk Transequator Lens; D. Mainster standard lens; E. Mainster widefield lens; F. Rodenstock Panfundoscopic lens
Volk PDT lens
- The field of view is 115/137 degrees
- Image magnification is 0.67x.
- Laser spot magnification is 1.5x
- Allows treatment of neovascularization up to maximum spot size of 6400um providing excellent visualization
- Comes standard with supracoat which covers the 689nm (Laser wavelength indicated in this type of procedure.)
Volk Transequator lens
- Designed for focal laser therapy and mid-to-far peripheral fundus diagnosis.
- The unique optical design presents a realistic contour of the retinal concavity, offering an impressive wide-field of view of the entire posterior pole extending to the equator.
- superior optics allow dynamic movement on the globe, therefore increasing its functional field of view.
- The field of view is 110/132 degrees.
- Image magnification is 0.70x.
- Laser spot magnification is 1.44x.
Mainster Lens
- Introduced in 1986
- More field of view (58% greater than Goldman) and greater magnification.
- Although the field of view is 14% less than the
- Panfundoscope, but the lateral andaxial magnification are better which makes it useful for detecting retinal thickening.
- It has a biconvex, aspherical anterior lens element and a concave lens element to fit the corneal curvature.
- Inverted, real image located in front of its biconvex aspheric anterior lens element
Common Features of Mainster and Panfundoscopic lens
Large areas of the fundus may be treated in PRP without lens rotation.
Visualization of the optic disc and macula during peripheral treatment prevents disorientation.
The experienced laser surgeon can achieve a more peripheral view by tilting the lens off-axis.
The field of view is increased in myopes and decrease in hyperopes and will lead to differences in how far peripherally laser photocoagulation can be applied.
The working distance on these lenses is greater.
Anterior segment irradiance becomes excessive with large spot sizes (1000μm) but should be acceptable at a spot size of 500μm.
Mainster Standard lens
- For focal and grid laser treatment from the posterior pole to the mid periphery.
- The field of view is 90/121 degrees.
- Image magnification is 0.96 x.
- Laser spot magnification is 1.05x.
- High resolution, high magnification of image allows appreciation of subtle intraretinal details and retinalthickening.
- So, it is excellent for the diagnosis and treatment of macular edema, BRVO, CNVM in ARMD, and presumed ocular histoplasmosis.
PRP Lenses
Mainster wide-field lens
- This allows a very wide range of slit lamp magnification to be used.
- It has excellent ophthalmic resolution and images binocularity is maintained across the entire field of view.
- Used for PRP in PDR
- The field of view is 118/127 degrees.
- Image magnification is 0.68x.
- Laser spot magnification is 1.50 x.
Mainster Ultrafield PRP lens:
- Widest field of view available for PRP
- It has a unique optical design to provide a clear, bright image across the entire field.
- Lightweight has a secure fit flange for easy manipulation besides having a high-efficiency laser light anti-reflective coating.
- The field of view is 165/180 degrees.
- Image magnification is 0.51 x.
- Laser spot magnification is 1.96x.
Rodenstock Panfundoscopic lens
- Introduced in 1969 by Schlegel
- Used for PRP from the posterior pole to beyond the equator without the use of mirrors.
- Gives a panoramic view
- Inverted, real image located in its spherical biconvex anterior lens element.
- Thus, the biomicroscope must be located further from the patient's eye than using a Goldman lens
- This low biomicroscopic magnification produces adequate magnification with a large field and acceptable depth of focus.
- The working field is 84% greater than a Goldman
- Lateral magnification is 24% lesser than a Goldman.
- The spot size is 40% larger than the photocoagulator setting or twice large than the conventional contact lens.
Disadvantage
- It produces peripheral distortion.
- It can produce marked laser beam astigmatism while treating the peripheral retina.
- reflexes compromise retinal image thereby causing oblong burns when treating through the periphery of the lens.
Volk Quadraspheric lens
- The original 13 degrees Quadraspheric introduced in 1989
- Preferred wide-field fundus laser lens for diagnosis and treatment of the retina.
- The 4 aspheric surfaces also employ high-efficiency antireflection coatings thereby improving lens performance by reducing astigmatism across the entire field of view.
- It also enhances visualization through a small pupil.
- Inverted and reversed image.
- Its sleek 28.6mm diameter housing provides a definite advantage over competitive wide-field lenses for peripheral retinal viewing, reflection displacement, and ease of use.
- The laser spot magnification is 1.97x
- The image magnification is 0.51x.
Volk Super Quad 160 lens
- offers the widest field of view.
- ideal 0.5x image magnification
- simultaneous visualization of the posterior pole to the peripheral retina providing a greater margin of safety even during extreme wide-angle panretinal photocoagulation.
- field of view is 160/ 165 degrees
- Image magnification is 1.97x
- laser spot magnification is 2.0x.
- he ideal lens for visualization and treatment of PDR, ischaemic
- RVO and peripheral retinal holes and tears.
- Laser beam transmission and fundus image quality are sharp and undistorted to the full extent of the viewing field.
- Volk has introduced two new high resolution (HR) lenses for laser photocoagulation
- The HR Wide Field for Pan Retinal Photocoagulation (PRP)
- The HR Centralis for focal and grid laser therapy
- Both lenses feature double aspheric designs and high grade, low dispersion glass which gives superior imaging quality.
- Both lenses may also be used as diagnostic lenses as well.
- The lenses improve upon and replace the previous generation
- Superquad 160 and Area Centralis lenses.
- Primary conditions diagnosed and treated are diabetic retinopathy and maculopathy.
- Lenses can also be used to diagnose and treat other conditions such as retinal tears, breaks, and holes.
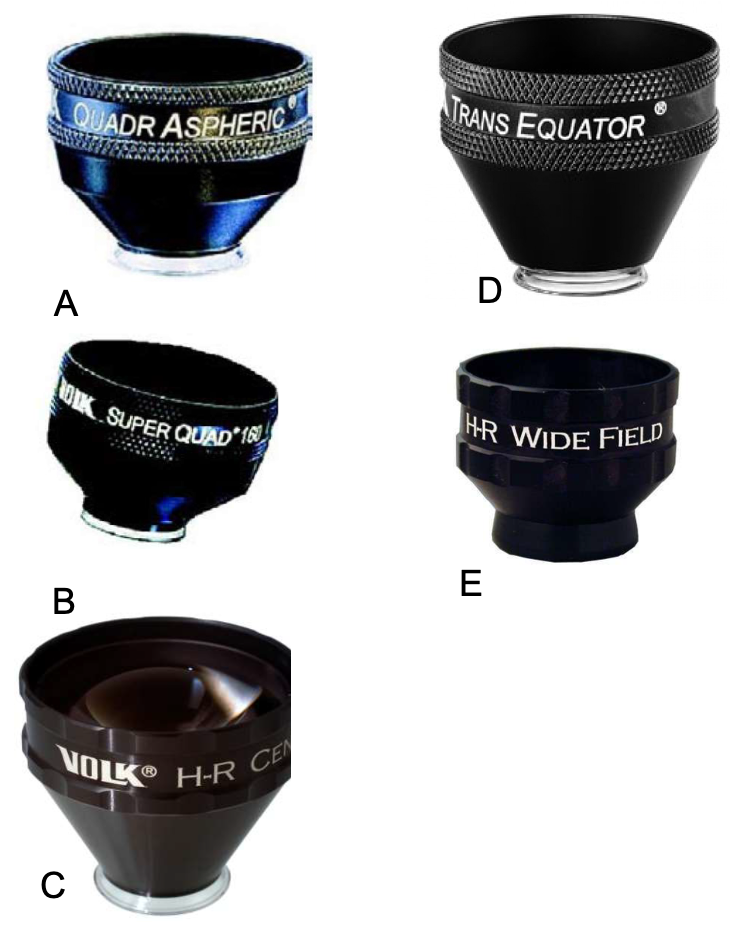
Lens for lasers A. Volk Quadraspheric lens; B. 33 Volk Super Quad 160 lens; C. Volk HR Centralis Lens; D. Volk HR Centralis Transequator; E. Volk HR Widefield
HR Centralis Lens
- Lens for detailed posterior pole examination and laser focal/grid treatment
- The lens is an upgrade or replacement for:
- Volk Optical Area Centralis
- Ocular Mainster 1X Retina
- Ocular Mainster Focal/Grid
- Better image quality and stereopsis at the extreme of the lens view
- Specifications: FOV 74º, magnification 1.08x, laser spot 0.92x
- The enhanced double aspheric design eliminates distortion and improves stereopsis to the periphery of the view
- Superior, high grade, low dispersion glass delivers unsurpassed resolution
- Improved capability with pupils as small as 4mm
- Reduced sized housing helps manipulation within the orbit.
|
Table 8: Magnification And Field Of View Of Different Types Of Laser Contact Lenses |
||||||
|
Types Of Lenses |
Image Magnification |
Laser Spot Magnification |
Contact Diameter |
Lens Height |
Static FOV |
Dynamic FOV |
|
Volk Area Centralis |
1.06x |
0.94x |
- |
- |
700 |
840 |
|
Volk PDT Lens |
0.67x |
1.5x |
- |
- |
1150 |
1370 |
|
Volk Transequator |
0.70x |
1.44x |
- |
- |
1100 |
1320 |
|
Mainster Standard |
0.96x |
1.05x |
16mm |
31.8mm |
900 |
1210 |
|
Mainster Ultrafield |
0.68x |
1.50x |
15mm |
27.8mm |
1180 |
1320 |
|
Ultrafield PRP |
0.51x |
1.96x |
17mm |
28.11mm |
1650 |
1800 |
|
Volk Quadraspheric |
0.51x |
1.97x |
- |
- |
1200 |
1440 |
|
Volk Super Quad 160 |
0.50x |
2.00x |
- |
- |
1600 |
1650 |
HR Wide Field Lens
- Lens for extreme widefield examination and laser PRP treatment
- The lens is an upgrade or replacement for:
- Rodenstock pan fundus lens
- Volk Optical Superquad 160
- Ocular Instruments Mainster PRP 165
- Better image quality at the extreme periphery of the lens view
- Specifications: FOV 160º, magnification 0.5x,laser spot 2.0x
- Widest field of view and treatment area to the ora serrata
- Superior, high grade, low dispersion glass design eliminates distortion at the extreme periphery
- Much smaller and easier to manipulate within the patient’s orbit
- Short length of the lens helps manipulate in front of laser
|
Table 7: Comparing the parameters of ophthalmic laser contact lens |
||||
|
Parameters |
Goldman |
Kreiger |
Panfundoscope |
Mainster |
|
Anterior surface |
Flat |
Concave, Spherical |
Convex, Spherical |
Convex, Aspherical |
|
Power |
-67D |
-92D |
-82D |
+61D |
|
Image type |
Virtual erect |
Virtual erect |
Real inverted |
Real inverted |
|
Image location |
Posterior capsule |
Vitreous humor |
Biconvex lens |
Air |
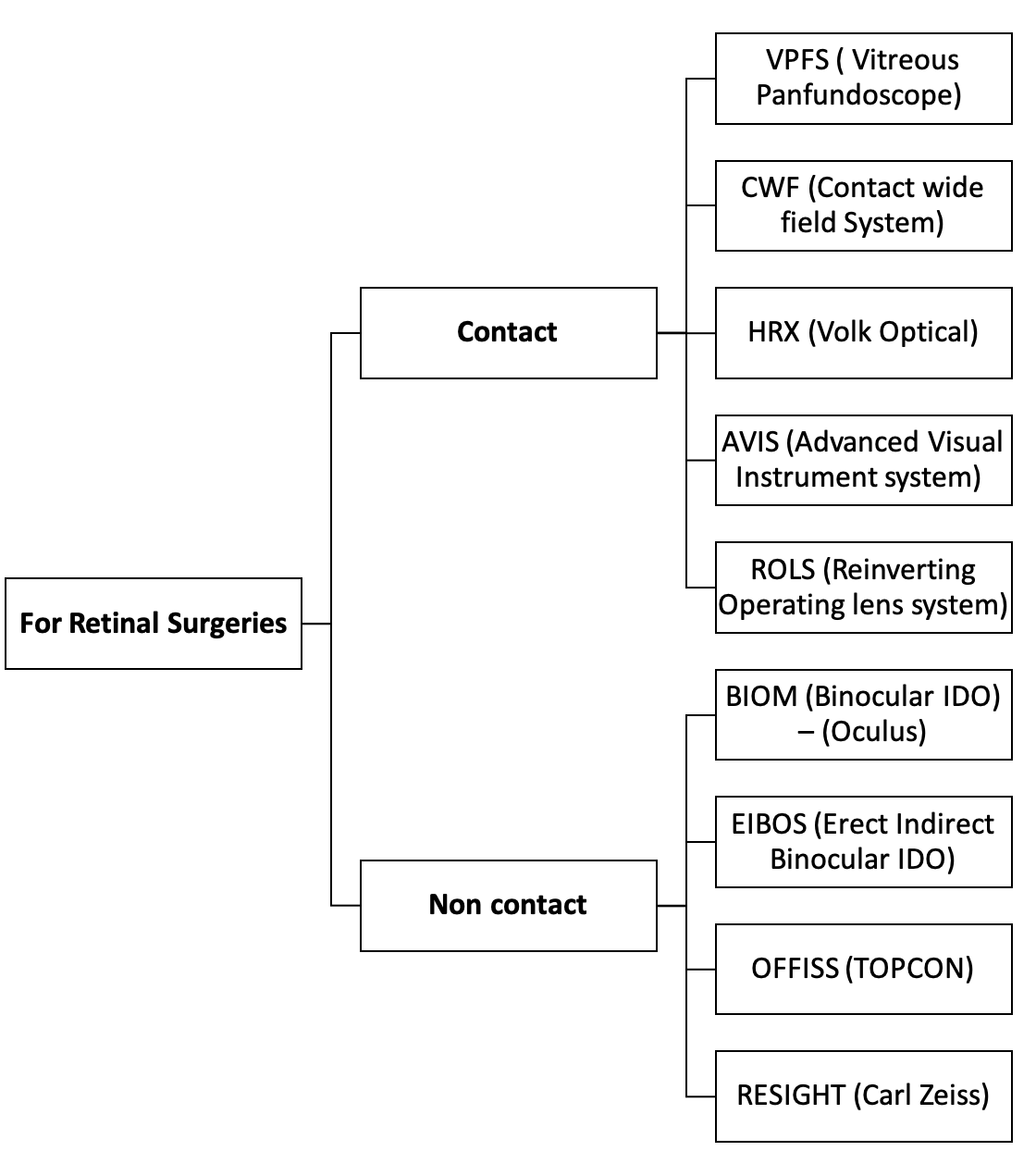
LENS FOR RETINAL SURGERIES
Contact Type :
- VPFS ( Vitreous Panfundoscope)
- CWF (Contact wide field System)
- AVIS (Advanced Visual Instrument system)
- ROLS (Reinverting Operating lens system)
- Clarivit
- HRX (Volk Optical)
Non Contact Type :
- BIOM (Binocular IDO) – (Oculus)
- MERLIN –(Volk Optical )
- EIBOS (Erect Indirect Binocular IDO)-
- OFFISS (TOPCON)
- RESIGHT (Carl Zeiss) - Peyman –Wessels-Landers
|
Table 9: Advantages and disadvantages of contact and non-contact systems |
|
|
Contact |
Non-contact |
|
Advantages |
|
|
Image resolution and stereopsis |
No intraoperative corneal trauma |
|
Eliminates corneal aberrations & limits the number of reflecting surfaces |
Good view during Fluid air exchange |
|
Wider field of view- Less need of rotation |
Good view- small pupils and irregular corneas |
|
Disadvantages |
|
|
Poor view in case of corneal or lens opacity/haze |
Poorer image resolution and depth perception |
|
Chance of corneal deformation |
Learning curve- more |
Hand-Held Irrigating Contact Lenses
- Neutralize High Convergence of Corneal Curvature to focus on Retina, Vitreous.
- 3 types of Lenses:
- Plano concave lenses with a view of 20 degrees
- Biconcave lenses with the view of 30 degrees
- Prism lenses with meridional view of 60 degrees
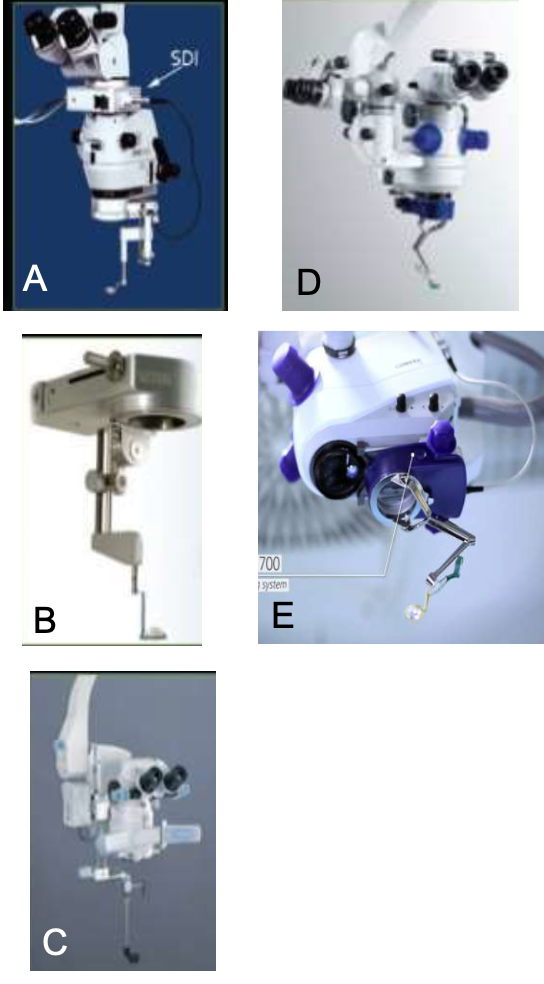
Figure:Operating systems: A. BIOM (Binocular IDO) – (Oculus); B. MERLIN –(Volk Optical ); C. OFFISS (TOPCON); D. RESIGHT (Carl Zeiss); E. Resight 700
Hands-Free Contact Lens (Landers System) OLIV-WF
- Hands-free contact lenses were introduced by Landers and coworkers which were stabilized onto the cornea with the help of a sewn-on limbal ring (stainless steel )
- Too tight – corneal folds, break suture midway of surgery
- Too loose- decentration of lens
- Bleeding can obscure the view of a surgeon.
- Plano concave lens – core vitrectomy
- Landers biconcave lens – visualization in air-filled eye
- (90 D Lens – 25 deg angle field)
- Machemer's magnifying lens – surface details on a posterior pole (28-30 deg
- angle field)
- Peyman wide-field lens –equatorial portion
- Tolentino 20 degree prism – periphery
- Tolentino 30 degree prism – extreme periphery
Disadvantages:
- Limited field of view
- Peripheral Retina is seen only with Indentation
- Lens alignment problems
- Air Bubble/ Blood film coming beneath Lens System
- Poor visualization in Small pupils and Fluid –gas exchange
OPTICS OF CONVENTIONAL VITREOUS SURGERY
- A Plano-concave contact lens made of PMMA
- Refractive index of 1.488 and a concave posterior surface radius of curvature of 7.7 mm is
- Refractive power of the anterior surface 48.8 D to -14.5 D and the fundus is easily visualized
Optics of Conventional Contact Lenses
- The first component (inferior lens) –acrylic contact lens concave posterior surface. Power of 4 D.
- The second component (superior lens) –biconvex aspherical image-forming, high refractive index glass lens 0.5 mm anterior of the contact lens element and effective power of 150 D in air.
- Real, inverted, aerial retinal image anterior to the image forming lens system.
Optics in Air-Filled Eye
- The posterior surface of the lens becomes strongly refractive(64 D)
- The total refractive power of the eye increases from 59 to 102 D
- Field of View is 1300.
- The microscope eyepiece should be moved closer to the patient's eyes.
Peyman-Wessels-Landers 132 D Upright Vitrectomy Lens
- Widefield Upright images without invertor(Internalised prisms).
- Operating Table mounted system
- Can be attached to any microscope
- When The OSVS-U132-2 used with the Ocular Peyman-Wessels-Landers 132 Dioptre Upright
- Vitrectomy Lens (OUV-132-2), the system allows the surgeon to work in the vitreous with an upright, non-reversed image under panoramic viewing conditions

Figure: Peyman-Wessels-Landers Lens in situ
Resight 700 from Carl Zeiss
- Can hold two lenses simultaneously
- 1270 lens for Wide Angle field
- 600 lens for High-resolution Macular lens
Contact Types
- VPFS ( Vitreous Panfundoscope)
- CWF (Contact wide field System)
- AVIS (Advanced Visual Instrument system)
- OLS (Reinverting Operating lens system)
Contact Widefield lenses
- Inverted image, Need of SDI
- Field of View = 120-1300
- Held by handle or Standard lens ring
Reinverting Operating Lens System
- Single element reinverter prism design to correct the inverted image.
- Mini Quad lenses -1270
- Mini Quad XL lenses – 1340
- Super Macula lens -600
- Dyna lens – 1560
High index corneal contact lenses
- Form an essential part of image capturing unit
- Allow capturing of oblique rays emerging from peripheral retina
- The changeable lenses (nose pieces) available to be attached to the image – capturing unit of Retcam II are as follows

Figure Lenses used In re inverting systems A. Mini Quad lenses B. Mini Quad XL lenses C. Super Macula lens D. Dyna
|
Table 10 - High index corneal contact lenses |
||
|
Lens |
Field of View |
|
|
ROP lens |
Premature infants |
130 degrees |
|
Standard children |
Pediatric to young adult |
120 degrees |
|
High magnification lenses |
Fine details |
30 degrees |
|
80-degree lens |
Higher contrast Pediatric and Adult imaging |
80 degrees |
|
Portrait lens |
For external imaging |
|
Care of optical devices with special reference to COVID era
General care
- Keep eye care equipment in an environment that is not humid; this will prevent the growth of fungus on optical components.
- Repeated cleaning will wear out the surface coating described earlier and the property of the surface may change.
- It is better to protect optical components from dust, stain, and fungus.
- Laser optics should only be cleaned by trained, qualified specialists.
What you will need
- Dust Blower
- Lens Brush
- Lint-Free Lens Tissue (Available In Photography Shops)
- Optical Cleaning Solutions
- Lint-Free Cotton Gloves
- Bamboo Tweezers
- Cotton Swabs
Method: Use non-sterile, medical-grade cotton swabs, with degreased fibers that will not release lint.
If these are not available, fresh cotton swabs can be prepared with wooden sticks and medical-grade cotton.
Optical cleaning solutions
1 Distilled water
2 A water-based solution: 1 part mild, neutral detergent to 19 parts distilled water
3 A mixture of 60% acetone and 40% methanol (not for use on plastic lenses)
4 Isopropyl alcohol (90% purity).
Tips for cleaning
- Do not touch optical surfaces with your bare fingers, since they leave behind grease and moisture marks that are hard to remove. Wear cotton, lint-free gloves if available and hold loose optical components by their edge.
- Be careful of sharp instruments, including your fingernails, near optical surfaces. Use wooden, bamboo, or plastic implements instead.
- Do not apply optical cleaning solutions directly onto the optical components. Instead, apply the cleaning solution to the lens paper or swab first.
- When removing stains, avoid excess pressure since this can remove the delicate surface coating.
Steps
1 Always remove dust first. Use a dust blower to remove dust. Use a camel hair brush, sometimes included as part of the blower to remove any dust that sticks to the surface.
2 To remove stains, use a lint-free cotton swab or a lens-cleaning tissue dipped in the optical cleaning solution. For round surfaces, move the swab or tissue in a circular path, starting from the center and going in a widening spiral towards the edge (Figure 3). For rectangular surfaces, use repeated strokes parallel to each other and in the same direction until you have covered the surface. Repeat this step, using a fresh swab every time, until the stain is no longer visible at any angle under a bright light. If cotton lint is left on the component, remove it using the blower or a clean lens brush.
3 To remove stains on plastic components, use optical cleaning solution number 2 (the water-based solution). Do not use other cleaning solutions on plastic, unless indicated by the manufacturer, because they can permanently cloud the surface.
4 To remove fungus, use an optical fungicide. If unavailable, use surgical scrub soap.
Specific instructions during COVID era
- Disinfect (using standard protocols) all instruments, and probes used in direct contact to the patient's tear film and ocular surface before re-use.
- The retinal examination should be done in patients who need it, strictly with an indirect ophthalmoscope. Avoid direct ophthalmoscopy and contact lens-based fundus examination
- Infants undergoing ROP screening must be placed on a designated crib with a plastic or polythene sheet, by the mother who uncovers the face of the infant and steps away more than 2 meters. The screener walks to the baby and screens (using indirect ophthalmoscopy or a retinal camera). The barrier sheet is replaced or sanitized between successive infants.
- Slit-lamp barriers or breath shields. These can be designed indigenously by cutting out a transparent plastic sheet of an appropriate thickness. The slit lamp touch-contact parts should be cleaned by alcohol wipes after examining every patient and the barriers should be changed for each patient. Barriers can be washed with soap water, dried, and reused.
- Alcohol-based hand sanitizer before and after examining each patient.
Further Reading:
- Mukherjee PK. Clinical Examination in Ophthalmology-E-Book. Elsevier Health Sciences; 2016 May 17.
- 2019-2020 Basic And Clinical Science Course, Section 03: Clinical Optics
- Khurana AK, Khurana AK, Khurana B. Theory and practice of optics and refraction. Elsevier India; 2014.
- Elkington AR, Frank HJ, Greaney MJ. Clinical optics. Wiley-blackwell; 1999 Aug 25.
- Dada T, Sidhu T. Gonioscopy: A Text and Atlas. JP Medical Ltd; 2017 Nov 30.
- Wiguna DY, Widjaja SA, Sasono W, Firmansjah M, Yustiarini I, Prakosa AD, Moestidjab M, Suhendro G. Condensing Lens on Binocular Indirect Ophthalmoscopy and Slit-Lamp Biomicroscopy. International Journal of Retina. 2019 Sep 18;2(2).
- Das T. Retinal laser optical aids. Indian journal of ophthalmology. 1991 Jul 1;39(3):115.
- Thomas R, Thomas S, Chandrashekar G. Gonioscopy. Indian journal of ophthalmology. 1998 Oct 1;46(4):255.
- Cordero I. How to care for and clean optical surfaces. Community eye health. 2010 Dec;23(74):57.