

A slit-lamp is a binocular microscope used for eye examination using a slit-like light beam. In 1911, Allvar Gullstranda Swedish Ophthalmologist designed table-mounted binocular eyepiece for 3-dimensional visualization of optically clear eye structures. Later Otto Henker, combined Gullstrand slit lamp with Czapski’s binocular microscope resulting in first slit lamp biomicroscope, allowing hand-free examination of an eye.1
The optical design of the Slit-Lamp Biomicroscope (SLB).
Due to the miniature size of the anterior segment of the eye, we need high magnification and clarity to appreciate finer details. This can be achieved by having 2 convex lenses at the observer end (eyepiece) separated at its focal distance (astronomical telescope type alignment) and, a concave-convex combination (Galilean telescope type alignment) at the examinee’s end for further magnification of the image. Telescopic arrangements of lenses need to be focused at near, hence a plus power objective lens is fixed at the examinee’s end. The eyepiece lenses invert image by default hence a porro-abbe prism is placed in front of it for erect image visualization. Lastly, one eyepiece for each eye aids in binocular visualization and depth perception. 2 (Figure-1)
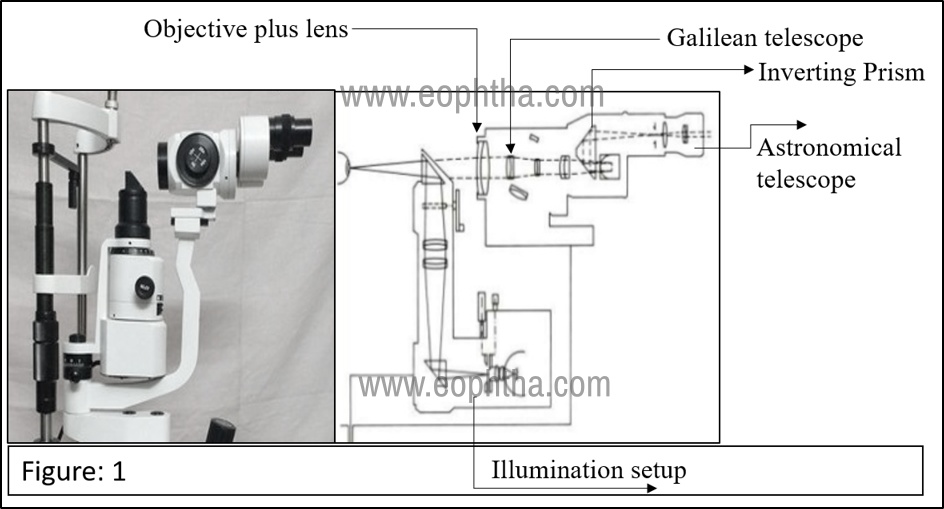
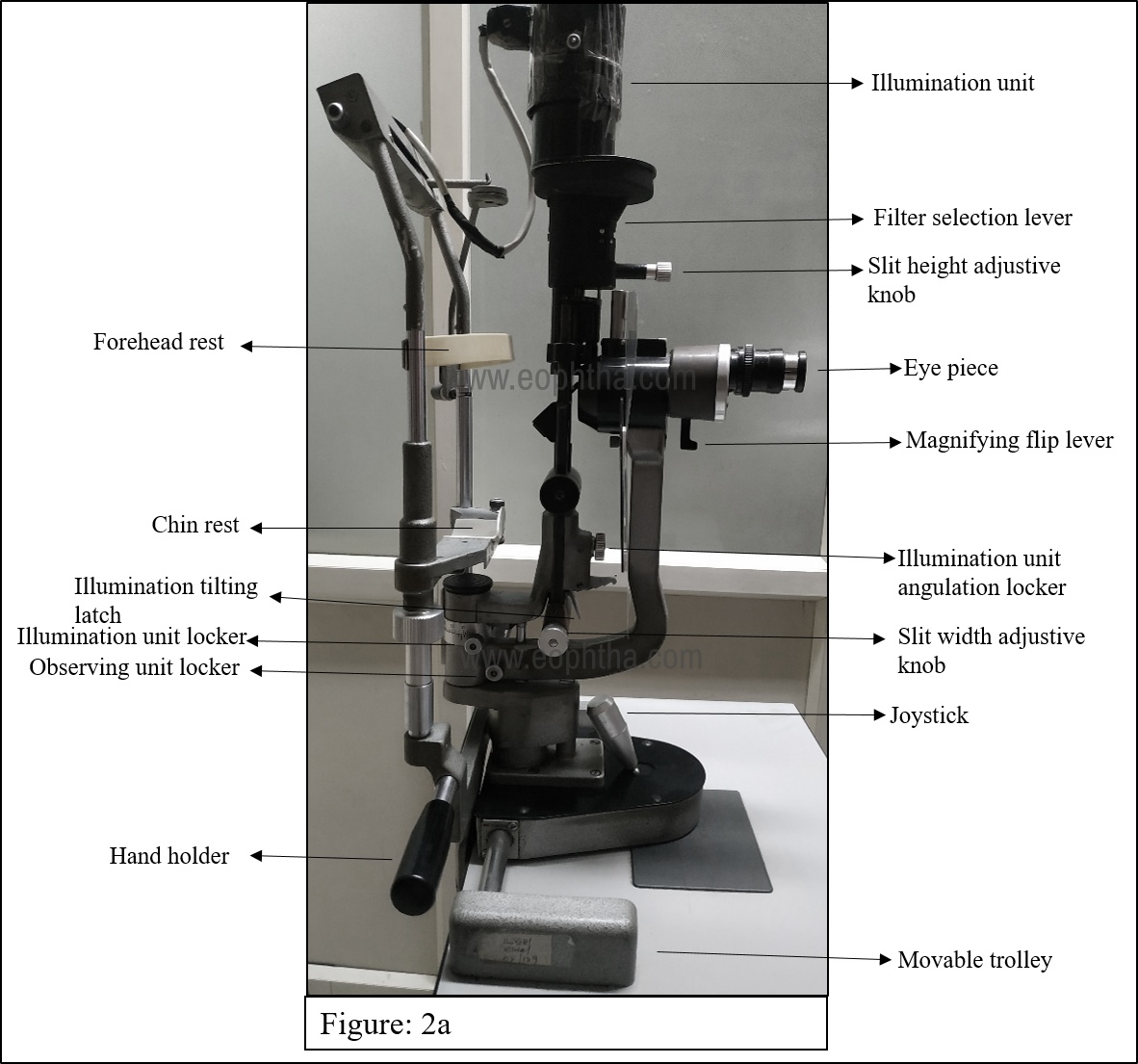
The illumination system is either a halogen or xenon lamp. Light passes through a slit diaphragm converting diffuse light into a slit beam. Both the observing system and illumination units are fixed around the same center of rotation for para focal movement to ensure slit beam and observing focus fall on the same point of interest. Both the illuminating system and the observing unit are fixed over the mechanical stand. A joystick allows the to-fro, side-to-side, and up & down moments of both units. Chinrest and fixation targets allow the examinee to rest and fixate. (Figure-2a).
Models and accessories:
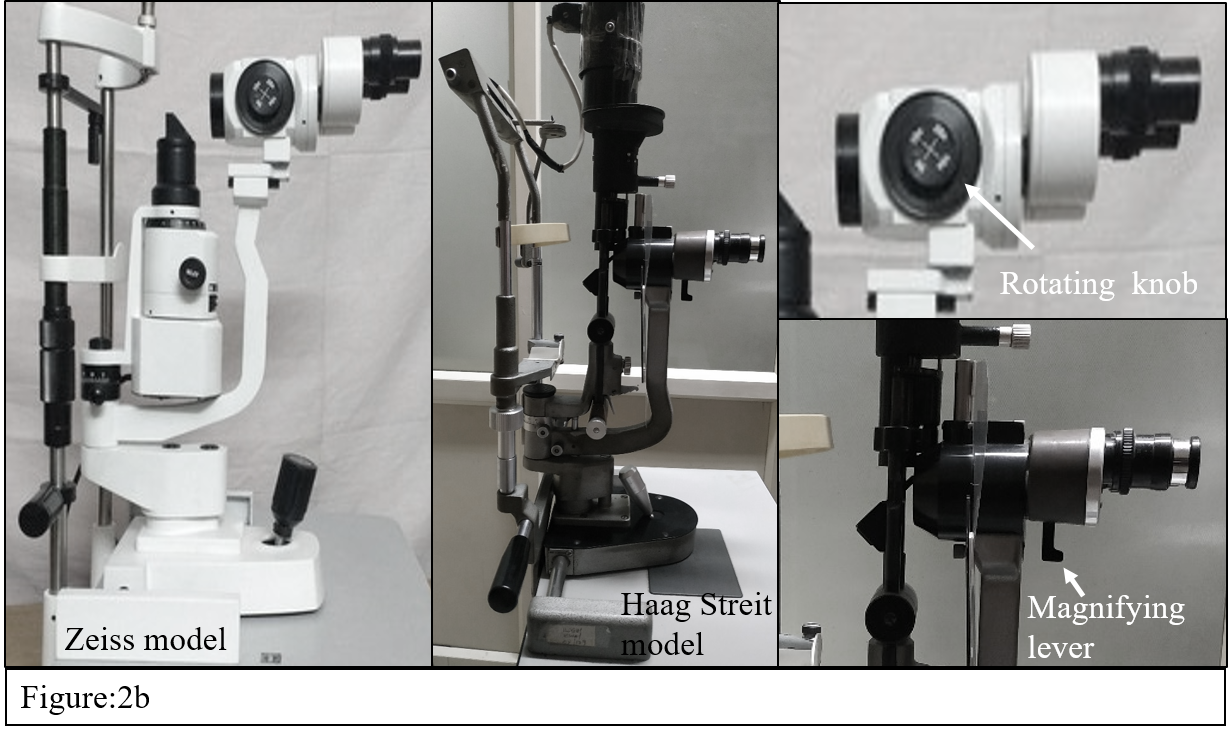
The illumination unit may be vertically oriented with a light source at the top (Haag Streit) model or the light source may be at the bottom with a horizontal prism reflecting the light (Zeiss model). In general, the magnification is achieved by a flip lever in the Haag Streit model (Greenough type) or knob to change magnification as in Zeiss model (Galilean changer type) (Figure 2b)
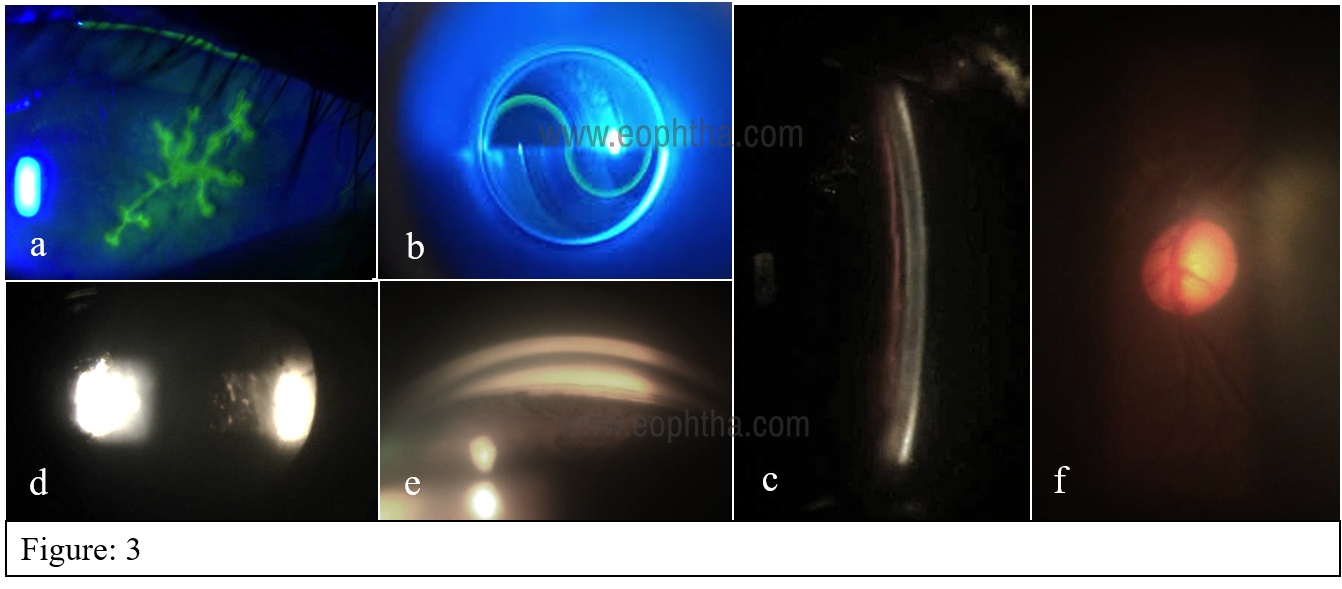
Just like filters in indirect ophthalmoscope, SLB is also fitted with a blue filter which, along with fluorescein stain is used to study the integrity of conjunctiva and cornea (Figure-3a) and also during applanation tonometry. (Figure-3b)Red free filters help in better visualization of blood vessels and hemorrhages. Neutral density filter decreases brightness comforting the patient. Polarising filters reduces unwanted specular reflections. Special yellow filters enhance contrast when used with fluorescein or cobalt blue filter.
Slit beam with its freedom of adjustable height, width, rotation, and intensity, allows examination of the anterior segment in different ways. A calibrated knob is provided to adjust the height of the slit and is used to measure the dimensions of lesions. A narrow slit beam at limbus can be used to measure the depth of the anterior segment angle (Figure-3c), Conical (pinpoint) slit through the anterior chamber appreciates Tyndal moment of cells and aqueous turbidity (Figure-3d). Angles can be studied by goniolens (Figure-3e) and fundus by +90diopter lenses. (Figure-3f)
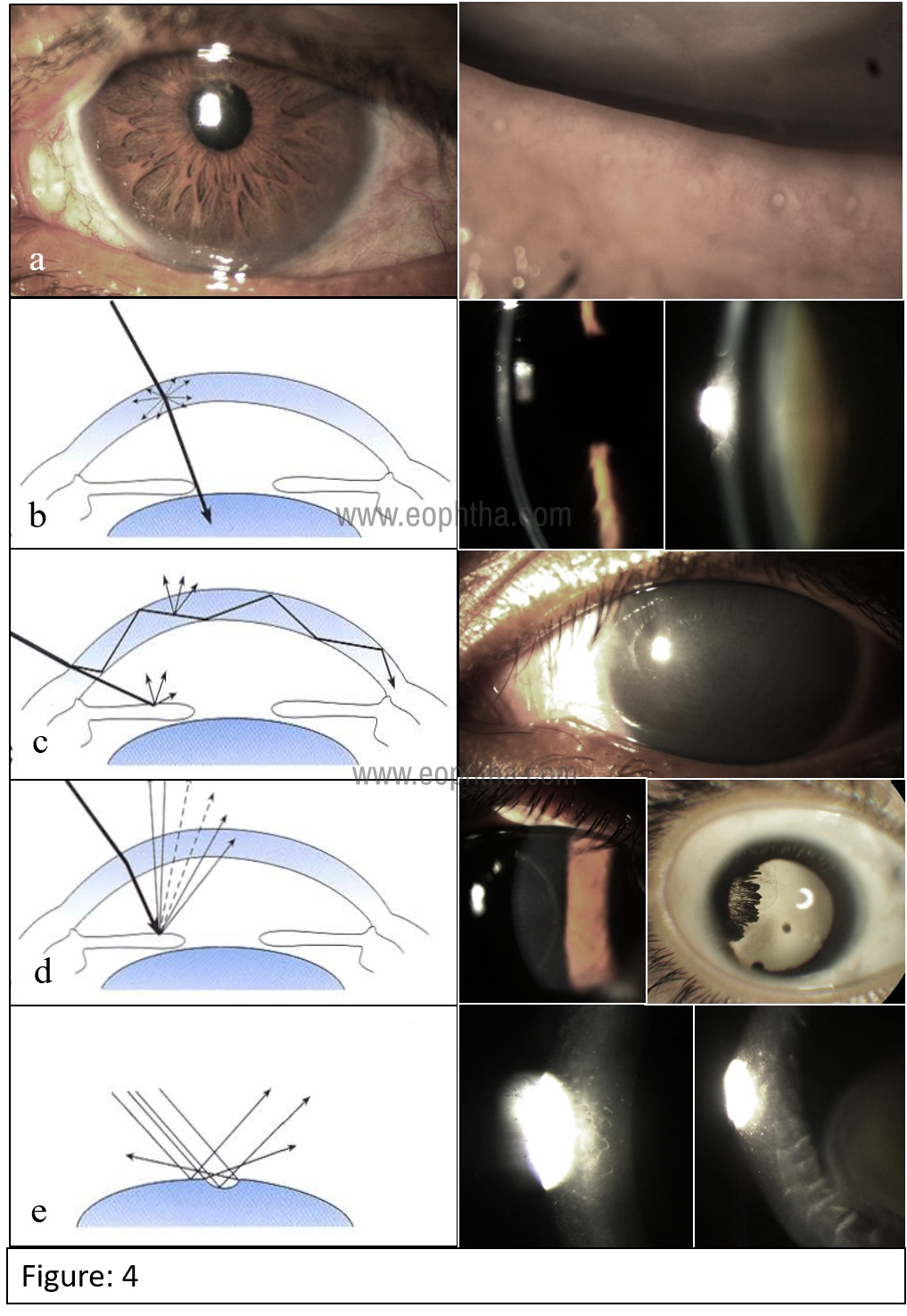
A diffuse slit-free illumination is used for gross pathologies of the lid margin, conjunctiva, and cornea. (Figure-4a) A direct slit illumination passes a narrow slit of light through the transparent tissues and helps in the cross-sectional study of opaque lesions like corneal and lens opacities (Figure-4b). The light directing at the sclera glows the cornea through total internal reflection and indirectly highlights subtle corneal pathologies (Figure-4c). Light is made to reflect from the iris (Iris retro illumination) or fundus (fundus retro illumination) to visualize corneal and lens opacities better. (Figure-4d). A parallelopiped beam of light focused at an angle over the cornea delineates enface architecture (Figure-4e). Tangential beam used for visualization of iris and lens surfaces.3 (Appendix-1)
Additional fittings: A beam splitter can be fitted to a viewing system to share visualization with secondary attachments like an observer tube to teach students or capture videos/ digital photos. Additional attachments like pachymetry, keratometry, OCT for angle study, smartphone camera system, and fundus camera can be fixed for respective uses. Collagen cross-linking system fixed to slitlamp for cross-linking can be carried as OPD procedures. Software programs can be inculcated into slit-lamp for remote operating which is under the evolving stage in the field of teleophthalmology. A miniature portable slit-lamp is a handy and mobile piece to examine bed-ridden patients and in operationtheatres.
Examination and drawings
A slit-lamp examination is done in a semi-dark room. After comfortable positioning of the examinee, adjust the chinrest position such that the patient lateral canthus is aligned with the mark on the headset bar. Target is given to fix during the examination. With appropriate illumination examine eyelids and lashes, tear film, conjunctiva, cornea, anterior chamber, iris and pupil, lens, and vitreous in order.
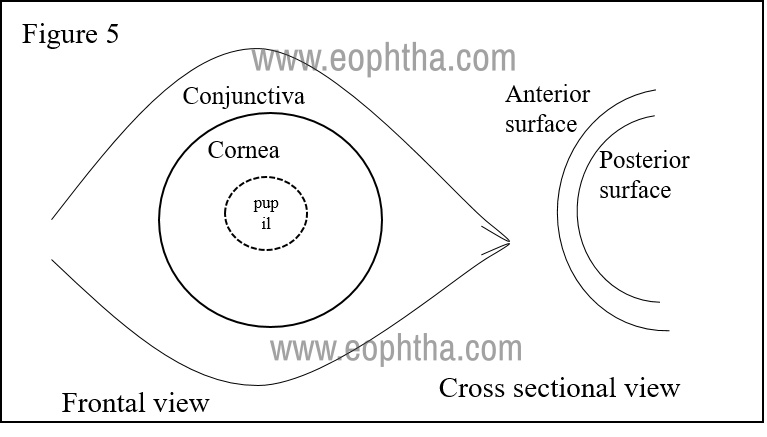
Drawing slit-lamp examination findings and pseudo coloring are important for follow-up and also for teaching purposes: (Figure: 5) Red for blood vessels and bleeds, Blue for edematous tissue, green for surface defects, yellow for infiltrates, hypopyon, and lastly blue/black for pigmented regions/lesions.
Fundus visualisation and lenses
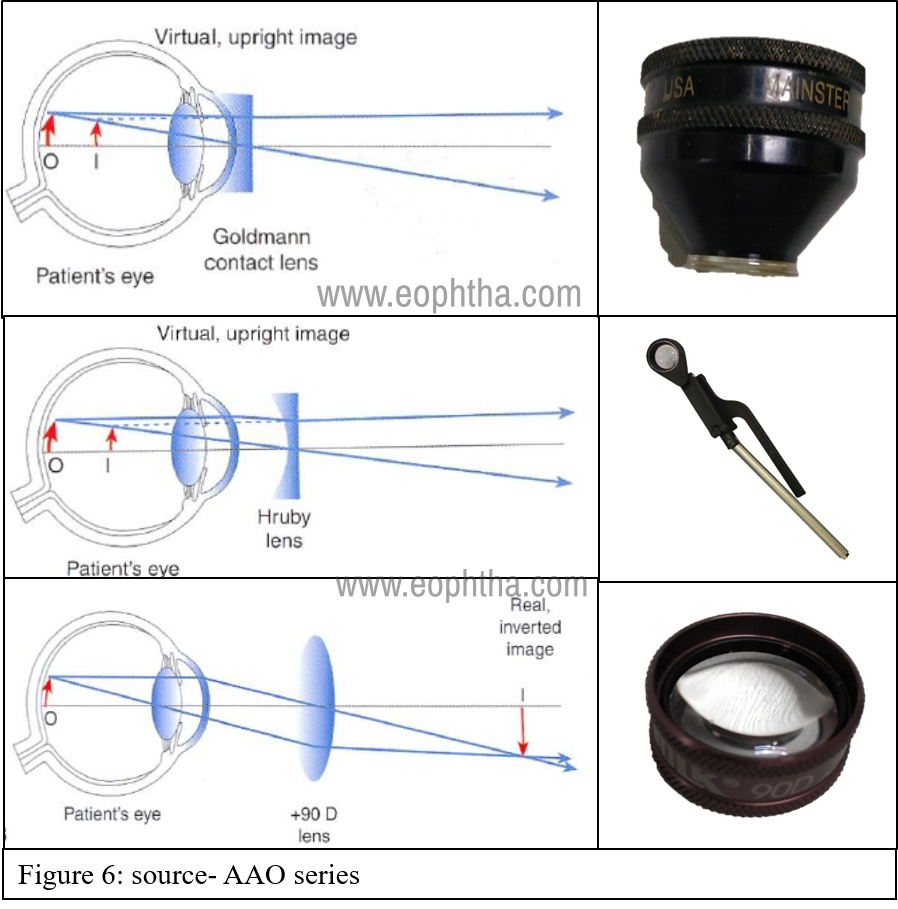
The high refractive power of cornea does not allow direct visualization of the fundus. Contact lenses are used to nullify the curvature effect of the cornea like Goldman fundus lens, Hruby Lens, Zeiss 4-mirror goniolenses. Here images are virtual and upright. Non-contact lenses with very high power can be used (+78, +90Diopter spherical lenses) to visualize the aerial image of the fundus just like an IDO (upside down and laterally inverted images).3 (Figure:6) With these lenses, SLB gives a magnified, stereoscopic view of the posterior pole. Panoramic fundus view up to the periphery can be obtained with appropriate lenses.
Relative magnification, the field of view depends on the power of the lens and refractive status of the eye. In general, the higher the power of the lens, the lesser the magnification and wider is the field of view. The details are addressed in the appendix-2. Generally, +78/90 non-contact lenses are used in OPD settings for quick examination of the posterior pole (magnification factor for 78 is nearly ×1, hence often used for macular examination and disc examination). For laser delivery and other therapeutic procedures, contact lens methods are used which have a higher field of view than non-contact lenses.
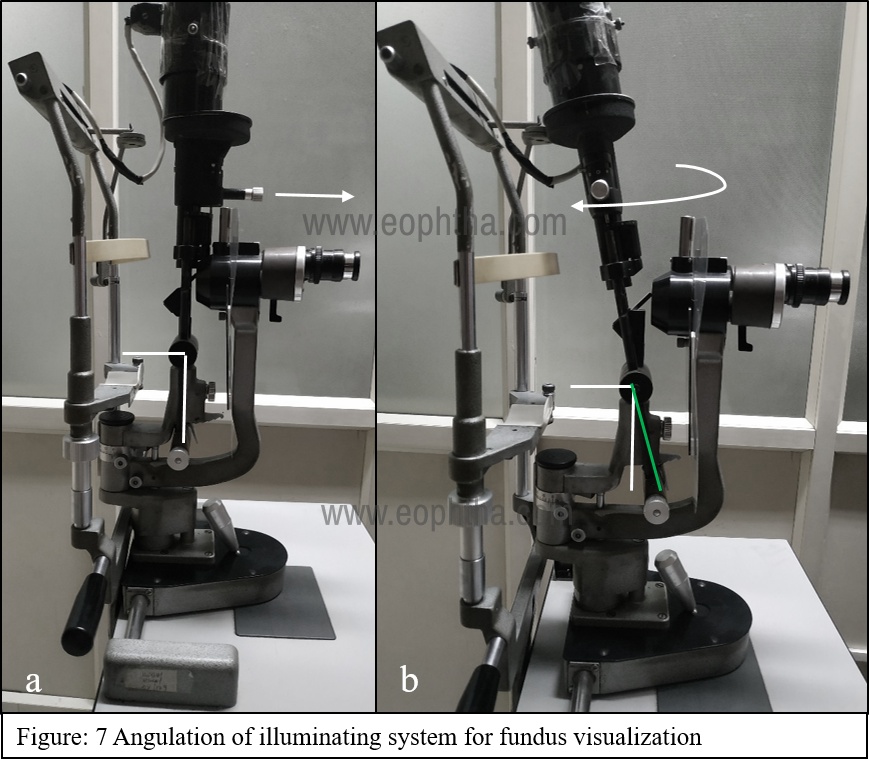
Haagstriet models have an illumination unit with tilting latch. Dissociation of parafocality is done by the tilting illumination unit. This trick coupled with a horizontal slit beam for 90/78D lens use avoids unnecessary reflexes allowing reflex-free fundus examination. (Figure:7)
Mastering fundus visualisation in slitlamp
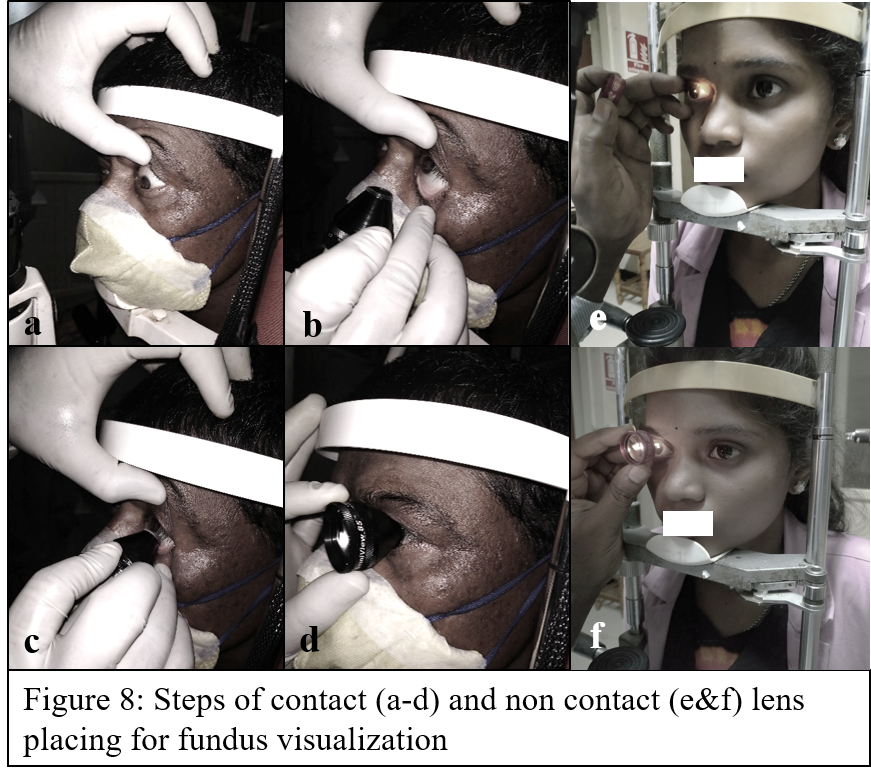
The technique of visualizing the fundus image in a non-contact method is the same as IDO. Just that a high magnifying lens is used here and working distance is brought down with the use of additional lenses in slit-lamp. The observer (observing unit) – lens-pupil of examinee should be on the same axis to visualize the fundus. The contact method examination involves a coupling agent like lubricant gel (4 mirror gonio lens may not need a coupling agent) and the lens is placed over the cornea for examination. After comfortable seating, both upper and lower lids are pulled and the examinee is asked to look upwards. The contact lens is placed from below over fornix and the examinee is asked to look straight while the observer slowly guides the contact lens over the cornea. (Figure 8a-d) The non-contact lenses are kept at an approximately 1-2 centimeter distance from cornea while fingers are used to separate both eyelids. (Figure 8 e&f).
Macular details can be visualized by macular contact lenses and larger areas can be visualized by pan-fundus lenses. Additionally, goniolenses are designed specifically for both angle assessment and fundus visualization. The mirrors are angulated and designed to visualize a specific portion of the posterior segment.
Maintenance of Slit lamp and lenses.
A lint-free cloth moistened with alcohol is used to clean the headrest, chin rest, and hand holder. If paper strips are used for chin rest, they have to be replaced with every use. Gonio lens, +90D/78D to be washed with soap and water and air-dried.
Take-home tips:
1. Learning para focal illumination and focusing comes with practice. The majority of anterior segment lesions are best appreciated when techniques are perfectly executed.
2. Make the best use of filters for different conditions and at different times of examination.
3. Angulation of the illuminating unit removes unwanted reflexes during fundus examination by contact and non-contact lenses.
4. Keeping the slit-beam horizontal makes macular visualization more comfortable and convenient.
5. Don’t miss an opportunity of using and learning the contact method fundus visualization technique which is easier with a better view than non-contact one.
|
LENS |
MAGNIFICATION |
FIELD OF VIEW (Degrees) |
|
78 D |
0.93x |
81/97 |
|
90 D |
0.76x |
74/89 |
|
GOLDMANN 3 MIRROR |
1.06 |
60/66/76 |
|
AREA-CENTRALIS |
1.06x |
70/84 |
|
TRANSEQUATORIAL |
0.7x |
110/132 |
|
QUADRASPHERIC |
0.5X |
120/144 |
Appendix-1.
Source: Textbook of Optometry science and clinical management
|
Illumination |
Diffuse |
Parallelepiped |
optic section |
Conical section |
Sclerotic scatter |
Fundus retro illumination |
Iris Retro- illumination |
Specular reflection. |
|
Beam angle |
450 to 600 |
450 to 600 |
450 to 600 |
600 to 750 |
600 |
00 |
600 |
(usually 450) |
|
Beam height |
Maximum |
Maximum |
maximum |
3-4mm |
Maximum |
Maximum |
Maximum |
maximum |
|
Beamwidth |
4mm to wide open |
1-2mm |
0.2-0.3mm |
0.5-0.6mm |
1mm |
1-2mm |
1-2mm |
1-2mm |
|
Magnification |
Low |
Start low then increase |
Increase as necessary |
20-30X |
Low |
Low to high as necessary |
Low to high as necessary |
High |
|
Illumination level |
Low |
Low |
Moderate to high |
Maximum |
Moderate |
Moderate |
Moderate |
moderate |
Appendix-2: Lenses and its magnifying power, field of view.
Source: Textbook of Optometry science and clinical management