
6.jpg)
Definition:
Double elevator palsy is classically defined as a congenital inability to elevate one eye, with the limitation more in abduction than adduction.1 MED is most often associated with ptosis/pseudoptosis. The word Double elevator palsy was coined by Dunlap to describe the weakness affecting both muscles of elevation i.e. superior rectus and inferior oblique.
Pathogenesis/Theories: 2
Superior Rectus palsy: Superior rectus is the main elevator in abduction, adduction, or primary position. Thus, the defective elevation can be explained by the presence of superior rectus palsy alone.
Inferior rectus restriction: Subsequently it was found that inferior rectus restriction can also cause such a limitation. The word double elevator palsy is a misnomer, Nearly 70% of cases, the cause for limitation was found to be IR restriction and not palsy. This was confirmed in several studies using saccadic velocity measurement and forced duction test.
Supranuclear palsy: The nucleus for upgaze is located in the midbrain pretectum causing an interruption in the input from rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF) into the third cranial nerve nucleus. Thus affecting the fibers mediating upgaze, supranuclear elevation deficiency may be a type of true double elevator palsy.
We now recognize that it can be caused by inferior rectus muscle (IR) restriction in isolation, supranuclear causes, or paralysis of the SR without ipsilateral IO weakness. There also can be IR restriction secondary to ipsilateral SR paresis
Since the cause may be paralysis or restriction, the term Monocular Elevation Deficit Syndrome is now used most often.
Etiology2:
|
Congenital MED |
Acquired MED |
|
|
Classification
Using scleral research coil for evaluating saccadic velocities, Ziffer et al, classified MED into three types3:
|
Types of MED |
Type 1 |
Type 2 |
Type 3 |
|
Disorder |
IR restriction |
SR palsy |
Supranuclear palsy |
|
FDT |
Tight IR ( positive) |
Negative |
Negative |
|
Upward Saccade |
Normal/limited |
Slow/floating |
Slow/absent above midline (Normal/slow below midline) |
|
Bell’s phenomenon |
Poor |
Negative |
Present |
Clinical presentation:
Abnormal head posture: Chin elevation, helps in maintain binocularity and decreasing diplopia. AHP is absent if the affected eye is amblyopic.
Deviation: Hypotropia of the affected eye is common (Figure 1). If fixing with the affected eye then, hypertropia in the normal eye can be seen(based on Hering’s law).One-third of cases, present as orthophoria in primary gaze.4

Extraocular movement: Unilateral limitation of upgaze above the midline, both in adduction and abduction.
Ipsilateral ptosis/pseudoptosis: A hypotropic eye is associated with ptosis because of the fascial attachments between the levator palpebrae superioris and the superior rectus muscle.
True congenital ptosis is seen in 25% of cases. Most often, it ispseudoptosis with a large hypotropia. (Figure 2a),which disappears when the hypotropic eye takes up fixation in the primary position. (Figure 2b)
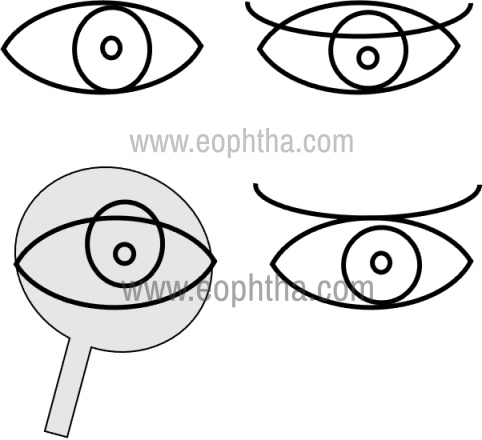
Figure 2 Upper picture showing primary gaze left Hypotropia of the left eye with ptosis Lower picture showing on occlusion of the right eye, left eye ptosis disappears suggesting pseudoptosis component.
Marcus Gunn's jaw winking phenomenon is seen in 25% of MED with congenital ptosis, due to abnormal development of oculomotor nerve with secondary muscle fibrosis.
Bell’s phenomenon is usually absent except if the supranuclear pathway is defective.
Acquired MED is associated with pupil abnormalities, convergence weakness, or downgaze paresis.
Upward saccade:
|
Slow/floating saccades |
SR palsy |
|
Absent saccades above midline with Normal/Slow below the midline |
Supranuclear palsy |
|
Normal initiation of saccades with an abrupt halt |
IR restriction |
Amblyopia is usually present owing to unilateral hypotropia of the affected eye or associated ptosis, or anisometropia.
Diplopia:MED with congenital onset usually has no complaints of diplopia as the affected eye is usually amblyopic. In acquired MED presents with acute onset vertical diplopia and is bothersome
Differential diagnosisFor Congenital MED includes,
- Brown’s Syndrome: features of limitation of elevation more in Adduction than abduction, tight superior oblique noted on exaggerated FDT, V pattern ( Exo on upgaze) helps in differentiating from MED
- CFEOM ( congenital fibrosis of extraocular muscles): Its familial occurrence, involves all or most extraocular muscles, positive FDT with IR restriction is characteristic
- Vertical Duane syndrome: Globe retraction on upgaze with co-contraction characteristic
- Congenital absence of SR+/- IO: closely mimics MED and craniofacial abnormalities may be present
- Third cranial nerve palsy: features of third nerve palsy with the involvement of depression and adduction apart from elevation helps in diagnosis
Differential Diagnosis For acquired MED include,
- Thyroid orbitopathy, Orbital floor fracture with entrapment
- Myasthenia gravis, Progressive external ophthalmoplegia
- Post cataract surgery due to myotoxic injury of SR or IR from local anesthesia.
- Partial 3rd nerve palsy- Superior branch of oculomotor nerve lesion.
- Labrynthine disorders, Cerebellar tumors
- Orbital inflammatory disease, orbital cellulitis, Systemic amyloidosis with extraocular muscle infiltration
Management:
- Observation is recommended for patients with limited head position changes and orthotropia in the primary position.
- Amblyopia should be treated in a conventional manner.
- Pseudoptosis will resolve after successful strabismus surgery in MED.
- Ptosis repair should be considered only if significant ptosis persists after strabismus surgery.
Indications for surgery:
- Vertical deviation in primary gaze
- Deviation causing suppression and amblyopia
- Diplopia in primary gaze
- Contracted binocular fields.
Goal:
To improve the position of the affected eye in primary gaze, thereby increasing the field of binocular vision.
Procedure :
The procedure of choice is determined by forced duction testing.
It ascertains whether the cause is paretic, due to superior rectus palsy and/or inferior oblique defect or restrictive, due to inferior rectus restriction.
Surgical Techniques:
If IR recession ( positive FDT ) and transposition needed to correct hypotropia then it’s done in a staged manner to avoid the risk of anterior segment ischemia
Various options to improve elevation( transposition ) include :
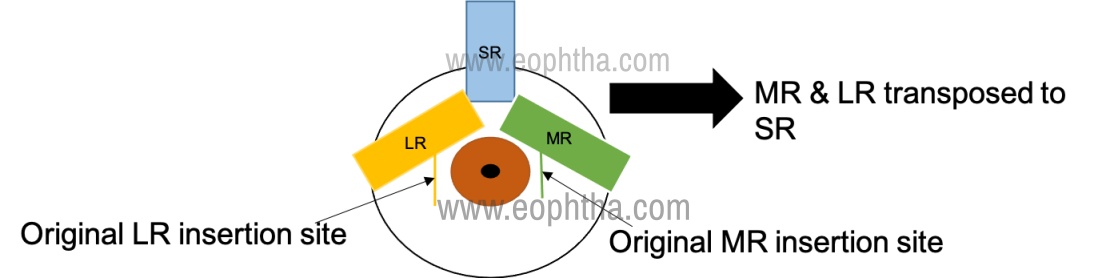
Knapp’s procedure: The full tendon of the medial and lateral rectus muscles are transposed to the insertion of the superior rectus muscle.5 (Figure 3)
Partial tendon Knapp’s procedure: Only half tendon i.e., superior halves of horizontal muscles is transposed to the superior rectus muscle insertion, leaving the inferior halves of tendon intact.(Figure 4) .
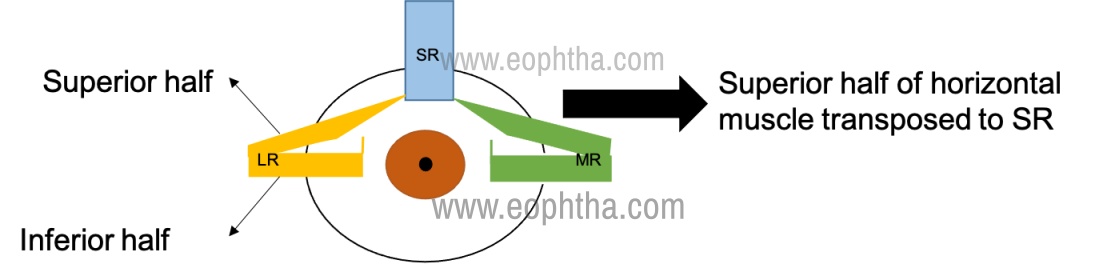
This avoids the risk of anterior segment ischemia with full tendon transposition of recti with IR recession.
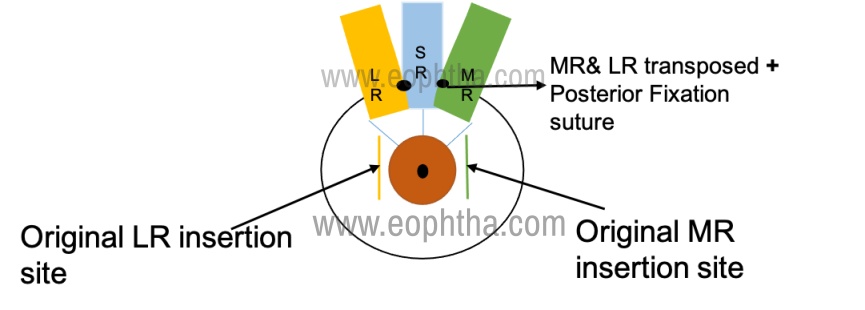
Augmented Knapp's procedure: Knapp's procedure combined with posterior fixation sutures on the horizontal recti, known as Augmented Knapp's.6(Figure 5)
Modified Nishida Procedure in MED: Newer No split-No tenotomy technique which involves using nonabsorbable suture to transpose superior 1/3rd of MR and LR to a point on sclera midway between SR and MR, SR and LR respectively 7
The advantage allows IR recession to be done simultaneously without risk of anterior segment ischemia noted and being a relatively reversible procedure.
Following the surgical correction of hypotropia, and improvement in Bell’s phenomenon, associated ptosis and/or Marcus Gunn phenomenon be addressed.
To summarise,
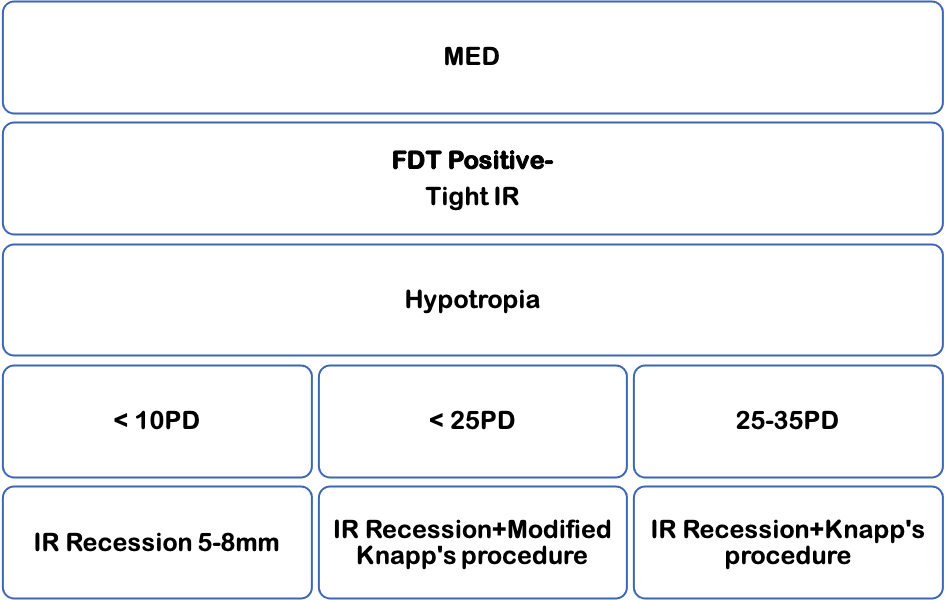
Management of MED with FDT Positive:
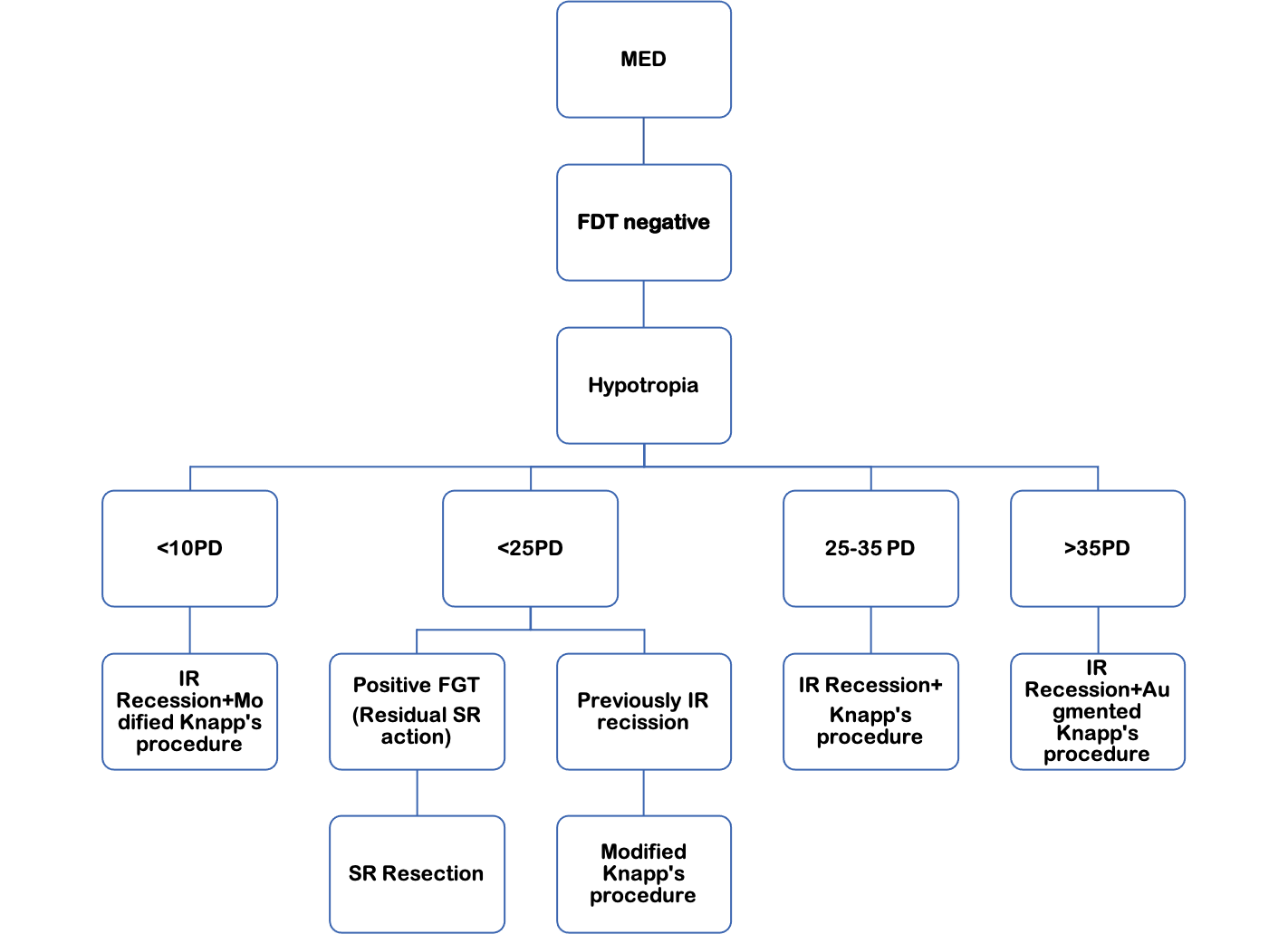
Management of MED with FDT Negative:
References:
- Wright, K. and Spiegel, P., 1999.Pediatric Ophthalmology And Strabismus. St. Louis: Mosby,3rd edition:345-346.
- Rosenbaum AL. Clinical strabismus management. 1st ed. Philadelphia: WB Saunders; 1999.
- Ziffer AJ, Rosenbaum AL, Demer JL, Yee RD. Congenital double elevator palsy: vertical saccadic velocity utilizing the scleral search coil technique. J Pediatr Ophthalmol Strabismus. 1992; 29:142–9.
- (Kanski JJ, Bowling B. Strabismus. Clinical Ophthalmology, 7th edn. Elsevier, p774.)
- Knapp P. The surgical treatment of double elevator paralysis. Trans Am Ophthalmol Soc. 1969; 67:304–23.
- Snir M, Frilling R, Steibel HK, Bourla D, Weinberger D. Combined rectus muscle transposition for posterior fixation sutures for the treatment of double elevator palsy. Am J Ophthalmol. 2005;112:933-8.
- Sowmya Ravendra Murthy, Mithuna Pappuru, Modified Nishida's procedure for monocular elevation deficiency JAAPOS, 2018 August;327-329.