
Introduction
Panophthalmitis is a severe ocular and orbital condition which can lead to phthisis bulbi or may necessitate evisceration. Severe inflammation of the anterior and posterior segments is frequently accompanied by microbial keratitis, necrotizing scleritis, and perforation or rupture following trauma. The disease develops rapidly and the prognosis is poor. The management of patients with intractable panophthalmitis remains challenging with eye salvage almost impossible in most cases.
Etiology and Pathogenesis
Panophthalmitisis a purulent inflammation of all coats of the eyeball includingintraocular structures. Although post-traumatic endophthalmitis is the most common preceding event, the infection can result after postoperative endophthalmitis following cataract surgery, keratoplasty, or rarely after posterior segment procedures. It can also be caused by septicemia or can spread from a pus-producing infection in another part of the body. [Table 1] Organisms implicated include - Bacillus species (most common), Streptococcus pneumoniae, Pseudomonas aeruginosa,Staphylococcus epidermidis, Clostridiumspecies, Salmonella, E coli, Klebsiella, Tuberculous, and also fungi. [1-6] [Table 2]
|
Post cataract surgery |
|
Post-traumatic |
|
Post penetrating keratoplasty |
|
Post microbial keratitis |
|
Endogenous or Metastatic ocular infection in systemic immune compromise |
Table 1 Etiology of Panophthalmitis
|
Bacterial |
Gram-positive |
Bacillus cereus (most common) Staphylococcus aureus, MRSA Streptococcus pneumoniae |
|
Gram-negative |
Pseudomonas aeruginosa (most common) Clostridium species E. coli Klebsiella Salmonella |
|
|
Tuberculous |
||
|
Fungal |
Aspergillus Fusarium Candida |
|
Table 2. Causative organisms of Panophthalmitis
Many theories have been postulated for the development of such overwhelming inflammation and necrosis in endophthalmitis which further progresses unabated to involve all the ocular coats. Endotoxins released by gram-positive cocci incite intense cellular and basement membrane inflammation which can cause a diffuse breakdown of various blood ocular barriers. This can lead to exuberant inflammation in cases where the infection does not get timely controlled and plays a significant role in the progression. [4]
Panopthalmitis is more commonly seen in immunocompromised patients or in patients with a debilitating illness, diabetes being a common association. The possibility of metastatic ocular infection may be suspected when patients with severe systemic illness, like pneumonia or sepsis, or poor immune status present with intraocular inflammation and severely impaired vision.
Panophthalmitis can have potentially serious complications like orbital cellulitis, cavernous sinus thrombosis, meningitis, or encephalitis and can be fatal if left untreated.
Clinical features

Figure 1: External photograph of the eye with panophthalmitis
The most common presentation includes pain and severe periorbital swelling, purulent discharge, proptosis, loss of vision, and complete external ophthalmoplegia. [Fig 1] Careful examination is required to look for signs pointing to the etiology like a postoperative wound, signs of trauma, sinus inflammation in case of fungal infections. [Table 3]
|
Symptoms |
Pain |
|
Swelling of the eye |
|
|
Redness |
|
|
Loss of vision |
|
|
Watering and discharge |
|
|
Malaise and fever |
|
|
Signs |
Light perception may not be present in most cases |
|
Severe periorbital edema and erythema |
|
|
Severe eyelid edema with complete mechanical ptosis |
|
|
Purulent discharge |
|
|
Conjunctival congestion and severe chemosis, hemorrhagic chemosis esp in trauma cases |
|
|
Corneal signs – perforated corneal ulcer, opacification, graft failure |
|
|
Anterior chamber – hypopyon, severe iritis, flat AC in case of corneal ulceration |
|
|
Pupils: RAPD may be present |
|
|
EOM: variable degree of limitation of movements in all gazes |
|
|
IOP: variable, low in case of perforated corneal ulcers, high in cases of POE |
|
|
B scan Ultrasonography: scleral thickening with ‘T’ sign |
Table 3 Clinical features of panophthalmitis
Diagnosis
Clinical presentation is almost always diagnostic. B scan ultrasonography of the eye shows thickening of the scleral coats and collection of fluid in the subtenon’s space giving rise to the classical ‘T’ sign [Fig 2]; confirms the clinical diagnosis.
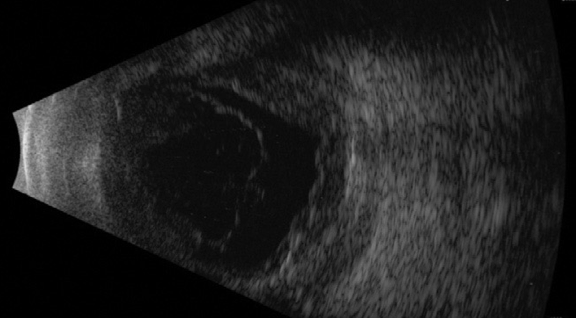
Figure 2: USG Bscan showing vitreous echoes, thickening of the choroid and subtenon’s fluid collection
Diffuse thickening of ocular coats along with altered signal intensity in the vitreous cavity is a common finding on contrast-enhanced MRI of orbits and brain. Extraocular muscles and peri-ocular tissues show abnormal enhancement along with variable distortion of the globes.
Laboratory investigations reveal anemia, leukocytosis along with neutropenia, and raised ESR. In patients with suspected septicemia, blood cultures are sent. Cultures from anterior chamber tap and vitreous tap samples may help isolate the causative organism.
Management
Panophthalmitis is a very serious infection and has usually an explosive course with rapid deterioration if untreated. Even with treatment, eye salvage remains a challenge more often than expected. The patient is hospitalized with close monitoring of ocular signs.
Medical
All patients are started empirically on broad-spectrum intravenous antibiotics (usually ceftriaxone 2 g/ cefotaxime 1g and gentamycin 80 mg twice daily) along with supportive therapy. In cases of trauma, metronidazole is added alongside either intravenously or oral. In patients with suspected fungal infections, especially in immunocompromised cases with suspected fungal sinus infections, amphotericin B infusions are prescribed. These patients often need aggressive sinus intervention by otolaryngologists. [6] Monitoring and control of blood sugars levels is crucial in patients with diabetes. Antibiotics may be reviewed depending on the findings of microbial culture and antibiotic sensitivity tests.
Pappuru et all have recommended the simultaneous administration of systemic corticosteroids to control the inflammation in cases of endophthalmitis progressing to panophthalmitis. They found the administration of systemic steroids to have very high odds of a favorable final outcome. [4] However this still remains controversial, especially in diabetic patients.
Surgical
Treatment in the form of intravitreal antibiotics is advocated, but usually, the functional outcome is very poor. Vitrectomy is not possible, due either to poor media clarity or weak outer coats of the eye and severely congested choroidal tissues. In most reports in the literature on the management of panophthalmitis, the globe was lost requiring evisceration or enucleation. Although in some cases infection may be controlled with prolonged antibiotic therapy, functional outcomes remain poor with eyes going into phthisis bulbi. Factors predicting good outcome in endophthalmitis progressing to panophthalmitis have been hypothesized by some authors.[4] [Table 4]
|
p-value |
|
|
Systemic steroid administration |
0.001 |
|
Intravenous antibiotics administration |
0.04 |
|
Presenting vision ≥ LP |
0.06 |
|
Gram-positive cocci in smear |
0.03 |
|
Culture positivity |
0.03 |
|
Age < 40 years |
0.47 |
Table 4 Factors predicting good outcome in endophthalmitis progressing to panophthalmitis.[4]
Because of a relatively high extrusion rate and the potential for sympathetic ophthalmia in the other eye, enucleation has been recommended [7,8]. In recent decades, evisceration with either delayed or immediate implant placement has been recommended in patients with endophthalmitis. Although delayed primary closure has certain theoretical advantages, primary implantation of orbital implants can prevent prolonged hospitalization and the need for additional surgeries [9-14].However, attempts at implant placement with evisceration are typically abandoned during surgery because the implant is considered unlikely to remain within the necrotic sclera. Melting of the scleral necrotic tissue causes a high extrusion rate of the orbital implant. [12] Frill evisceration is a technique popularised in these situations, wherein all the necrotic sclera is excised leaving a frill of healthy sclera around the optic nerve head. The conjunctiva may or may not be sutured.
Conclusion
Early diagnosis and prompt treatment is very important in the management of this condition. Outcomes are invariably poor and globe salvage still continues to remain a challenge.
References
- Abel AD, Meyer DR.Enucleation with primary implant insertion for treatment of recalcitrant endophthalmitis and panophthalmitis.Ophthal Plast Reconstr Surg2005;21:220–226.
- Green, Mary T.; Font, Ramon L.; Campbell, James V.; Marines, Hector M. (1987). "Endogenous Clostridium Panophthalmitis".Ophthalmology.94(4): 435–438.
- Drancourt, Michel; Fenollar, Florence; Denis, Danièle; Raoult, Didier (2009)."Postoperative Panophthalmitis Caused by Whipple Disease".Emerging Infectious Diseases.15(5): 825–827.
- Pappuru RP, Dave VP, Pathengay A, Gangakhedkar S, Sharma S, Narayanan R, Tyagi M, Grzybowski A & Das TP (2018) Endophthalmitis Progressing to Panophthalmitis: Clinical Features, Demographic Profile, and Factors Predicting Outcome, Seminars in Ophthalmology, 33:5, 671-674.
- Chawla R, Garg S, Venkatesh P, Kashyap S, Tewari HK. Case report of tuberculous panophthalmitis. Med Sci Monit 2004;10:CS57-9
- Adulkar NG, Radhakrishnan S, Vidhya N, Kim U. Invasive sino-orbital fungal infections in immunocompetent patients: a clinicopathological study.Eye (Lond). 2019;33(6):988‐994.
- Androudi S, Theodoridou A, Praidou A, Brazitikos PD.Sympathetic ophthalmia following postoperative endophthalmitis and evisceration.Hippokratia2010;14:131–132.
- Rathinam SR, Rao NA.Sympathetic ophthalmia following postoperative bacterial endophthalmitis: a clinicopathologic study.Am J Ophthalmol2006;141:498–507.
- Hui JI.Outcomes of orbital implants after evisceration and enucleation in patients with endophthalmitis.Curr Opin Ophthalmol2010;21:375–379.
- Jackson TL, Paraskevopoulos T, Georgalas I.Systematic review of 342 cases of endogenous bacterial endophthalmitis.Surv Ophthalmol2014;59:627–635.
- Migliori ME.Enucleation versus evisceration.Curr Opin Ophthalmol2002;13:298–302.
- Shore JW, Dieckert JP, Levine MR.Delayed primary wound closure. Use to prevent implant extrusion following evisceration for endophthalmitis.Arch Ophthalmol1988;106:1303–1308.
- Tawfik HA, Budin H.Evisceration with primary implant placement in patients with endophthalmitis.Ophthalmology2007;114:1100–1103.
- Ozgur OR, Akcay L, Dogan OK.Primary implant placement with evisceration in patients with endophthalmitis.Am J Ophthalmol2007;143:902–904.
Comments