

Case presentation:
A 65-year-old man presented to our clinic with gradually progressive protrusion and swelling of both eyes and double vision for 1 year associated with progressive drooping of the right upper eyelid. There is acute onset of pain in the left eye for 10 days. A smokerfor 25 years.
Past ocular history
No h/o previous ocular surgery or trauma
Past medical history
The patient is a diagnosed case of hyperthyroidism, Graves’ disease for 2 years. On treatment with Tablet Neomercazole 5mg per day. No history of radio-iodine therapy. The patient has no history of diabetes, hypertension, or cardiac disease.
Family history
No significant history
Ocular Examination:
|
Right Eye |
Left Eye |
|
|
IOP |
18 mmHg |
21 mmHg |
|
VISUAL ACUITY (UCVA) |
6/60 |
3/60 |
|
BCVA |
6/24 |
6/60 |
|
COLOUR VISION |
NORMAL |
8/21 |
|
OCULAR MOTILITY |
-1 RESTRICTION IN ALL DIRECTIONS |
-3 RESTRICTION IN ELEVATION -2 RESTRICTION IN ALL DIRECTION |
|
PALPATION |
NO PALPABLE MASS |
NO PALPABLE MASS |
|
LIDS AND LASHES |
NEAR-COMPLETE PTOSIS NO LAGOPHTHALMOS |
LID RETRACTION, LATERAL FLARE, LID EDEMA, 1mm LAGOPHTHALMOS |
|
HERTEL’s EXOPHTHALMOMETRY |
@105 - 27 |
@105 - 29 |
|
CONJUNCTIVA/SCLERA |
CONGESTION, CHEMOSIS, CARUNCULAR CHEMOSIS |
CONGESTION, CHEMOSIS, CARUNCULAR CHEMOSIS |
|
CORNEA |
NORMAL |
CONFLUENT PUNCTATE EPITHELIAL EROSIONS |
|
ANTERIOR CHAMBER |
NORMAL |
NORMAL |
|
PUPIL |
BRISK |
SLUGGISH, GRADE 2 RAPD |
|
IRIS |
NORMAL |
NORMAL |
|
LENS |
CLEAR |
CLEAR |
|
VITREOUS |
CLEAR |
CLEAR |
|
DISC |
DISC MARGINS CLEAR |
DISC EDEMA, HYPEREMIA |
|
MACULA |
NORMAL |
DULL FOVEAL REFLEX, CHOROIDAL FOLDS |
|
VESSELS |
NORMAL |
NORMAL |
|
PERIPHERY |
NORMAL |
NORMAL |
CLINICAL ACTIVITY SCORE (CAS) = 5
Pain on eye movement – 1
Lid edema – 1
Lid erythema – 1
Chemosis – 1
Congestion – 1
Caruncular chemosis - 1
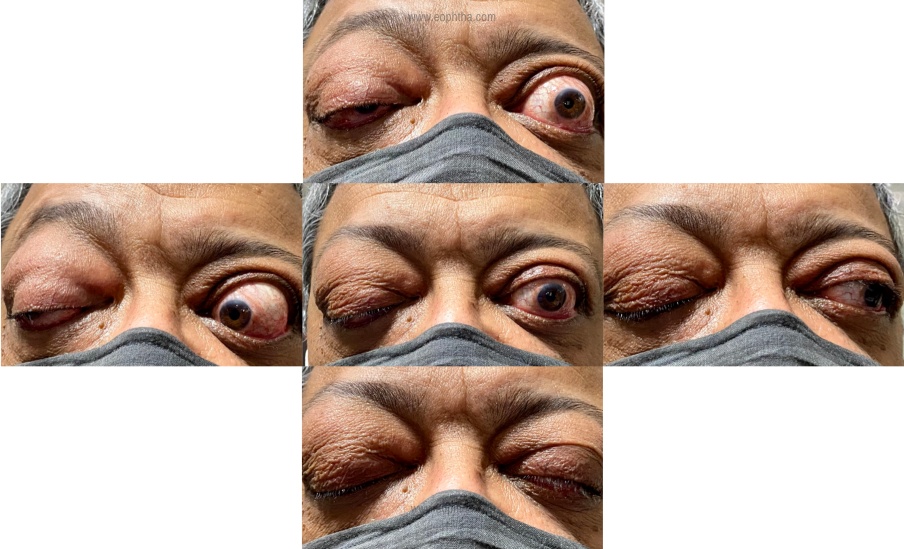
Figure 1: Clinical photographs demonstrating restricted ocular motility
Ancillary investigations
- FREE T3 and FT4- normal
- TSH- Normal
- TPO antibody- POSITIVE
- TRAb –POSITIVE
- CT SCAN- Bilateral extraocular muscle belly enlargement with sparing of tendons, forward displacement of the eyeball, crowding of the orbital apex on the left
- HVF 30-2 – (RE test could not be performed due to ptosis), LE shows constriction of field
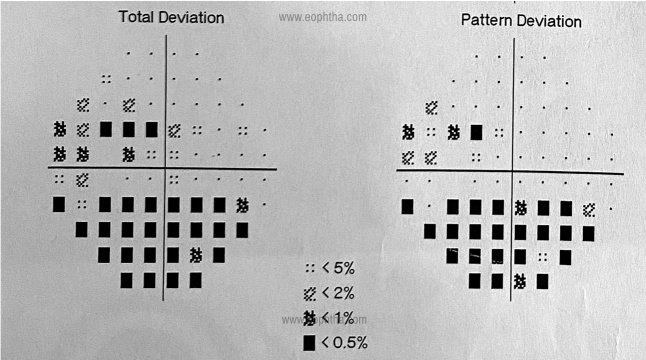
Figure 2: Humphrey’s Visual field (30-2) depicting constricted field of vision in left eye
DIFFERENTIAL DIAGNOSIS
- Thyroid Orbitopathy with dysthyroid optic neuropathy
- Thyroid Orbitopathy with Ocular Myasthenia
TREATMENT
We started the patient on 500mg IV steroid/week for 6 weeks. The patient is on the 4th-weekfollow-up. We notethe vision, fields, and optic nerve function at 6 weeks. If no improvement, we proceed with surgery for orbital decompression.
If he is medically not fit for surgery, we can then plan radiotherapy to salvage optic nerve function.
DISCUSSION:
ETIOLOGY
Thyroid eye disease (TED) is a complex orbital inflammatory disease, which can be sight-threatening, debilitating, and disfiguring. TED is also known as Graves’ ophthalmopathy, named after Robert J. Graves, an Irish physician who first described thyrotoxicosis in a woman presenting with goiter, rapid heartbeat, and exophthalmos1Thyroid-associated orbitopathy is an autoimmune disease caused by the activation of the orbital fibroblasts by the autoantibodies, that can affect the orbital and periorbital tissue, and also the thyroid gland and the pretibial skin or digits. Most frequently associated with Hyperthyroidism in 85% cases. 5% are euthyroid and 10% have hypothyroidism2. Other rare causes are Hashimoto thyroiditis, thyroid carcinoma and neck irradiation. In hyperthyroidism, eye signs of thyroid-associated ophthalmopathy(TAO) usually develop within 18 months. Radioactive Iodine (RAI) ablation of thyroid may initiate or exacerbate TED.3
RISK FACTORS
1) Smoking- increases the risk of TED by 7–8 times4
2) Family History
3) Female Gender5
4) Europeans
5) Monozygotic Twins
6) Genetic Predisposition- HLA B8, DR-3
7) HLA-DRB1-16 - Severe muscle involvement
EPIDEMIOLOGY
16 per 100,000 females and 2.9 per 100,000 males with - approximate prevalence.
Most Common Disease Affecting the Orbit:
Female: Male
9.3:1 (Mild Cases)
1.4:1 (Severe Cases)
Myasthenia Gravis is 50 Times More Common in Patients With TAO. 6
PATHOPHYSIOLOGY
Orbital changes in the thyroid ophthalmopathy result from de novo adipogenesis, hyaluronan synthesis, interstitial edema, and enlargement of the extraocular muscles.
Th1-like cytokine profile predominates into retrobulbar tissue. Th2 -type cytokines detected predominantly in orbital fat.
- Orbital fibroblast – principle cell responsible for the enlargement of the orbital soft tissue. Located in between the muscle fibers, orbital fat, and connective tissue. Based on the presence of Thy1/CD90 marker, OF are divided into 2 types. OF expressing Thy1 reside in perimysium of EOM and differentiates into myofibroblast. Thy1 deficient are preadipocytes and differentiates into mature adipocytes. The relative proportion of these 2 determines whether fibrosis or adipogenesis predominates. These OF have higher thyrotropin receptors and insulin-like growth receptors and thus are activated by them. The proliferation of the OF is activated by the interaction of autoantigens on the fibroblasts with T-cells.
- Fibrocytes- bone marrow-derived, fibroblast-like progenitor cell, expressing CD34 and leukocyte common antigen CD45 and various fibroblast proteins. In Grave’s disease, the amount of peripheral circulating fibroblast is more, infiltrating the orbital tissue and differentiating into adipocytes and myofibroblast and secrete inflammatory cytokines similar to OF.7
On activation- inflammatory cells T- cells, plasma cells, macrophages, mast cells) infiltrate orbital fat, lacrimal gland and orbital interstitium. And the release of cytokines (IL-1b, TNF-gamma, TGF-b) occurs on the interaction of CD4-T and fibroblast. These cytokines activate fibroblast to secrete hyaluronic acid and GAG.
Osmotic imbibition occurs causing swollen EOM and Compression of ON and later fibrosis and restrictive myopathy. Orbital fluid retention causes an increase in intraorbital volume thus leading to venous obstruction. Circulatory antibodies like TRAb, TSI are thought to be the mediators of orbitopathy.8
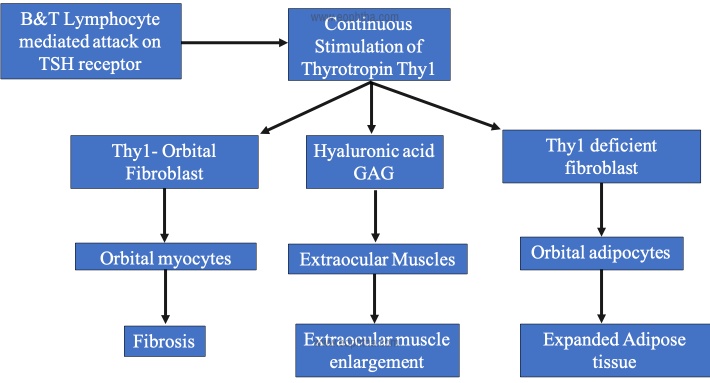
Table 1: Pathophysiology of TED
SIGNS
TAO has an active inflammatory phase and a stable post-inflammatory phase
The duration of the active phase is 6-18 months. The disease commences with an active (inflammatory) phase with rapidly worsening symptoms and signs, reaching a point of maximum severity which then improves to a static plateau but does not resolve to baseline (inactive phase). . This is known as Rundle’s curve9.image(webeye.optha.uiowa.edu). in “Inactive” disease defines the phase when no inflammation is present, yet residual fibrosis and its secondary effects persist. In the inactive phase, only surgical treatment can alter the outcome
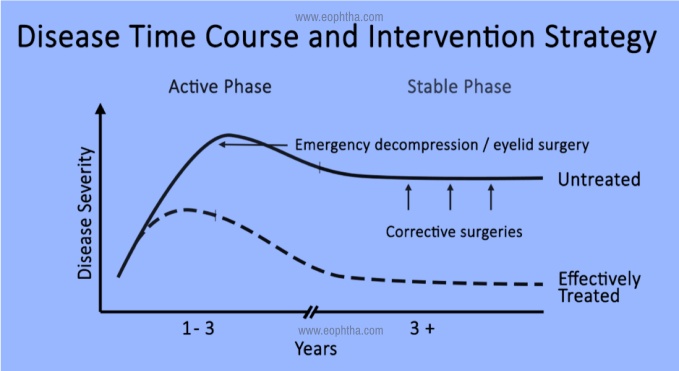
Table 2: Course of TED
In approximately 40% of patients with TED, the ocular and systemic symptoms have a simultaneous onset7. Approximately 60% of patients with hyperthyroidism will develop TED. For those with TED, 85% have hyperthyroidism, 10% have hypothyroidism and 5% are euthyroid2.
1. Eyelid retraction (91%)- with lateral flare- due to increased sympathetic innervation of muller muscle
- Overaction of the LPS contracting against a tight inferior rectus
- Muscle scarring between the lacrimal gland and levator
2. Proptosis (62%)- usually bilateral (90%). Axial, due to enlargement of the EOM and adipose tissue, as well as orbital fat deposits and the infiltration of the orbital tissue by GAGs and leukocytes. it is permanent in 70% of cases. Severe proptosis prevents adequate lid closure and may lead to severe exposure keratopathy and corneal ulceration
3. Restrictive myopathy (42%)- due to edema in EOM IR>MR>SR>LR
4. Soft tissue involvement- (often the earliest sign) conjunctival hyperemia, eyelid edema, chemosis, superior limbic keratoconjunctivitis
5. Optic neuropathy (6%)
SYMPTOMS
- Lid retraction (90%)
- Bulging eyes (60%)
- Movement restriction (40%)10
- Ocular pressure or pain
- Photophobia, lacrimation
- Diplopia
- Visual field loss
- Visual loss
- Dyschromatopsia
- Photopsia11
- Ptosis – potential mechanisms are levator dehiscence,compromise of the oculomotor nerve, or due to Idiopathic orbital inflammation (IOI) or, Others forms of myopathy
ANCILLARY INVESTIGATIONS-
- COLOUR VISION- an indicator of the optic nerve function
- VISUAL FIELDS- central, paracentral, arcuate, and nerve fibre bundle defects, increased blind spot, generalized constriction
- VEP- evidence of compressive optic neuropathy, prolonged P100 latency
- Highly Sensitive and Specific- T4+ TSH
- If eye findings associate with euthyroid Graves’ disease- TPO Ab
- Others- Free T4 Index, Anti Thyroid Antibodies, Serum T3, Thyroid Stimulating Immunoglobulin
IMAGING
1. CT SCAN- IMAGING OF CHOICE- Identify Minimal Enlargement of The Recti
2. MRI- sensitive for showing compression of the optic nerve. MRI is preferred over CT in the assessment of disease activity because it can estimate the water content of tissues. MRI protocol for TED patients is T1-weighted images and T2-weighted fat suppression or short tau inversion recovery (STIR) images in axial, coronal, and sagittal planes with 3-mm slice thickness. Imaging reveals –
- Thick muscle belly with tendon sparing- isointense on T1- weighted images and isointense to minimally hyperintense on T2- weighted images
- Usually IR and MR
- Isolated rectus muscle involvement (SR) up to 6%
- Bilateral muscle enlargement
3. ORBITAL ULTRASOUND- thickness of the eye muscles, high reflectivity and enlargement of belly and sparing of the tendons of the muscles
TREATMENT
In the active phase, systemic and local corticosteroids are considered and are most effective early in this phase, which prevents most of the morbidity associated with the disease. Other agents including cyclosporin, azathioprine, methotrexate, infliximab, and rituximab are gaining popularity and some are the subject of clinical trials12. Selenium supplementation can be used as it has been seen to significantly improve quality of life, decrease ocular involvement, and slow progression in patients with mild Graves' orbitopathy13. Orbital radiotherapy can be used as an adjunctive therapy and is particularly effective at improving ocular motility during active disease, due to the sensitivity of orbital lymphocytes to radiotherapy14According to the European group on graves’ orbitopathy (EUGOGO), a CAS score of 3 or higher defines active disease with a 65% positive predictive value for response to radiotherapy
For initial CAS, only score items 1–7
| 1 |
Spontaneous orbital pain |
|
2 |
Gaze evoked orbital pain |
|
3 |
Eyelid swelling that is considered to be due to active GO |
|
4 |
Eyelid erythema |
|
5 |
Conjunctival redness that is considered to be due to active GO |
|
6 |
Chemosis |
|
7 |
Inflammation of caruncle OR plica |
Patients assessed after follow-up (1–3 months) can be scored out of 10 by including items 8–10
|
8 |
Increase of >2 mm in proptosis |
|
9 |
Decrease in uniocular ocular excursion in any one direction of >8° |
|
10 |
Decrease of acuity equivalent to 1 Snellen line |
MANAGEMENT SYNOPSIS FOR THE PATIENT WITH TAO
1.Restore euthyroidism
2. To stop smoking
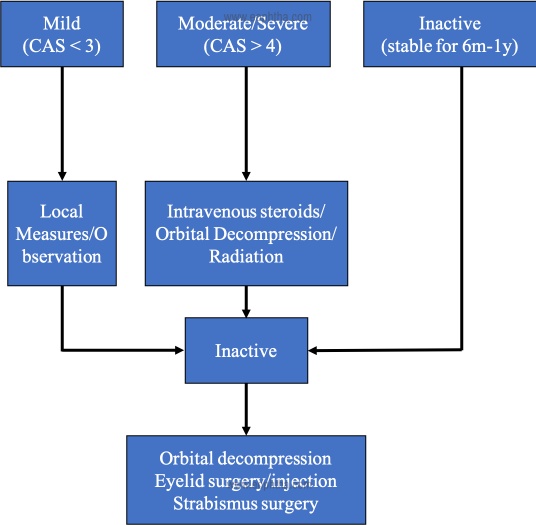
Table 3: Treatment Algorithm of TED
1. LOCAL MEASURES
- Add Selenium for 3-6 months
- Stop smoking
- Artificial tears for dry eye
- Nocturnal taping
- Topical adrenergic blocking agents (5% guanethidine sulfate) drops to improve lid eyelid retraction
- Dark goggles for photophobia
- Prisms to correct diplopia
2. IVMP pulse therapy- 500 mg/week for 6 weeks f/b 250 mg for 6 weeks OR oral prednisolone 1mg/kg/day in weekly tapering doses
3. Radiotherapy – for Optic Neuropathy, congestive signs and EOM involvement 20Gy per eye fractioned in 10 daily doses over a period of 2 weeks
4. Management of DON- IVMP 1gm for 3 days, if no improvement orbital decompression f/b steroids/ radiotherapy
5. Teprotumumab- biologic infusion therapy to reduce signs and symptoms of TED. It binds to IGF-1R and blocks its activation and signaling15,16
SURGICAL
Orbital Decompression– As a rule, each orbital wall would provide approximately 2 mm reduction in proptosis, and fat alone would provide 2 mm reduction.
Indications
a) Compressive Optic Neuropathy
b) Severe Exposure Keratopathy Due to Proptosis
c) Cosmesis
Trans-antral approach is the most preferable17
Endoscopic orbital surgery for thyroid decompression- provides excellent visualization with enhanced safety and less chances of infraorbital nerve and hypoglobus. There is no external scar. Postoperative recovery is faster.
It requires equipments and expertise. There is requirement of other procedure for better visualization like septoplasty.
Navigation guided surgery for thyroid decompression-The image guidance allows for more extensive bone removal near the optic tubercle as well as the sphenoid. In addition, it would greatly help in identifying crucial structures like the bony optic canal, onodi cells and the genu of carotid artery and hence has the potential to prevent any inadvertent injuries.
1. STRABISMUS SURGERY-
No active disease for at least 6 months
The aim is the resolution of the diplopia in primary position and downgaze.
Typically involves the release of the restricted muscle by the recession rather than resection
2. EYELID SURGERY- Most common indication is Eyelid Retraction- graded Muller and levator weakening. Surgery should be performed during the inactive phase.
- Lower lid lengthening is indicated in the lower lid retraction
- Surgical debulking of the excess skin and fat restore the normal appearance of the eyelid.
- Tarsorrhaphy-A lateral, paramedian or central tarsorrhaphy can help to protect the ocular surface, and augment the healing of frank microbial keratitis
- Full-Thickness Blepharotomy-This is done for moderate upper eyelid retraction, and involves a full-thickness eyelid incision, from the skin to conjunctiva, at the level of the eyelid crease
- Lower Eyelid Retraction-classified as mild (1 mm), moderate (2–3 mm), and severe (>3 mm) based on the inferior scleral show in primary gaze. Temporary nonsurgical correction is achieved by hyaluronic acid gel injections.
- Surgically, two broad types of procedures commonly performed are 1) recession of lower eyelid retractors and 2) extirpation, both being reported with and without an eyelid spacer graft.
- Botox injection is a minimally invasive temporary treatment for lid retraction. Other minimally invasive procedures for lid retraction are triamcinolone injection and Hyaluronic acid.
REFERENCES
1. Onimode YA, Dairo DM, Ellmann A. Pattern of presentation of Graves� disease and response to radioiodine therapy in South African men. Pan Afr Med J. 2018;29. doi:10.11604/pamj.2018.29.48.13655 2. Soeters MR, van Zeijl CJJ, Boelen A, et al. Optimal management of Graves orbitopathy: a multidisciplinary approach. Neth J Med. 2011;69(7):302-308. 3. Bartalena L, Marcocci C, Pinchera A. Graves’ ophthalmopathy: a preventable disease? European Journal of Endocrinology. Published online April 1, 2002:457-461. doi:10.1530/eje.0.1460457 4. Perros P, Neoh C, Dickinson J. Thyroid eye disease. BMJ. 2009;338(mar06 1):b560-b560. doi:10.1136/bmj.b560 5. Lazarus JH. Epidemiology of Graves’ orbitopathy (GO) and relationship with thyroid disease. Best Practice & Research Clinical Endocrinology & Metabolism. 2012;26(3):273-279. doi:10.1016/j.beem.2011.10.005 6. Peacey SR, Belchetz PE. Graves’ disease: associated ocular myasthenia gravis and a thymic cyst. J R Soc Med. 1993;86(5):297-298. 7. Epstein FH, Bahn RS, Heufelder AE. Pathogenesis of Graves’ Ophthalmopathy. N Engl J Med. 1993;329(20):1468-1475. doi:10.1056/NEJM199311113292007 8. Smith TJ, Hegedüs L, Douglas RS. Role of insulin-like growth factor-1 (IGF-1) pathway in the pathogenesis of Graves’ orbitopathy. Best Practice & Research Clinical Endocrinology & Metabolism. 2012;26(3):291-302. doi:10.1016/j.beem.2011.10.002 9. Rundle FF. Management of exophthalmos and related ocular changes in Graves’ disease. Metabolism. 1957;6(1):36-48. 10. Bartley GB, Fatourechi V, Kadrmas EF, et al. Clinical Features of Graves’ Ophthalmopathy in an Incidence Cohort. American Journal of Ophthalmology. 1996;121(3):284-290. doi:10.1016/S0002-9394(14)70276-4 11. Denniston AKO, Murray PI. Oxford Handbook of Ophthalmology. Fourth edition. Oxford University Press; 2018. 12. Verity DH, Rose GE. Acute thyroid eye disease (TED): Principles of medical and surgical management. Eye. 2013;27(3):308-319. doi:10.1038/eye.2012.284 13. Marcocci C, Kahaly GJ, Krassas GE, et al. Selenium and the Course of Mild Graves’ Orbitopathy. N Engl J Med. 2011;364(20):1920-1931. doi:10.1056/NEJMoa1012985 14. Bartalena L, Marcocci C, Tanda ML, et al. Orbital Radiotherapy for Graves’ Ophthalmopathy. Thyroid. 2002;12(3):245-250. doi:10.1089/105072502753600223 15. Douglas RS, Kahaly GJ, Patel A, et al. Teprotumumab for the Treatment of Active Thyroid Eye Disease. N Engl J Med. 2020;382(4):341-352. doi:10.1056/NEJMoa1910434 16. Smith TJ, Kahaly GJ, Ezra DG, et al. Teprotumumab for Thyroid-Associated Ophthalmopathy. N Engl J Med. 2017;376(18):1748-1761. doi:10.1056/NEJMoa1614949 17. Rath S, Naik MN. Surgery in Thyroid Eye Disease: A Conceptual Approach.; 2020.