

Introduction
Uveal melanoma is the most common primary intraocular malignant tumor in adults [1]. Second most common type of primary malignant melanoma after cutaneous melanoma. It arises from neuroectodermal melanocytes within the uveal tissue.
Epidemiology
There is strong racial variation in the incidence, with the white population most commonly affected. The mean age-adjusted incidence of uveal melanoma in the United States is 5.2 per million per year [2]. Males had a significantly higher age-adjusted incidence of 6.0 per million population compared to females, where the average age-adjusted incidence was 4.5 [3].
Malignant melanoma of the choroid is rare in dark pigmented races and has been reported infrequently in the Asian Indian population.[4] Ultraviolet (UV) radiation has been suggested as a major cause of malignant melanoma of the skin and uvea[5] because of the increased incidence and mortality among Caucasians living in tropical regions, where solar radiation is more intense.[5]
Most choroidal melanomas have been diagnosed in white patients over 50 years of age.[4, 11] In the Collaborative Ocular Melanoma Study, 1302 patients eligible for the study had a mean age of 60.2 years. Only 14% of patients were below 50 years of age. [6] Melanoma of the choroid usually presents as a dome shaped or mushroom shaped pigmented mass with secondary retinal detachment. Such lesions can be diagnosed by indirect ophthalmoscopy and ultrasonography. Diffuse malignant melanoma is a rare variant with a flat growth pattern with thickness of 20% or less than the greatest basal dimension.
Pre Disposing Factors
Weis et al. [7] provided a meta-analysis of all published reports on host factors for uveal melanoma and found that light eye color, fair skin color, and inability to tan were risk factors for the development of uveal melanoma. Shah et al. [8] investigated the environmental factors and found that intermittent ultraviolet exposure to arc welding was a significant risk factor.
Two important factors for the development of uveal melanoma are the presence of a pre-existing choroidal nevus and the presence of congenital ocular/oculodermal melanocytosis, also termed ‘nevus of Ota’.
Clinical Characteristics
Choroidal melanoma generally manifests with symptoms of persistent photopsia (flashes), floaters, visual field loss, or visual acuity loss or it can be asymptomatic. Occasionally, there are sentinel vessels if the tumor involves the ciliary body.
Choroidal melanoma is pigmented in 55%, non-pigmented in 15%, and mixed pigmented or non-pigmented in 30% [21]. (Image 1) Choroidal melanoma appears in one of three configurations- dome (75%), mushroom (20%), or diffuse (5%). A lesion may penetrate bruchs membrane and the retinal pigment epithelium with herniation into the subretinal space, assuming the shape of collar stud.
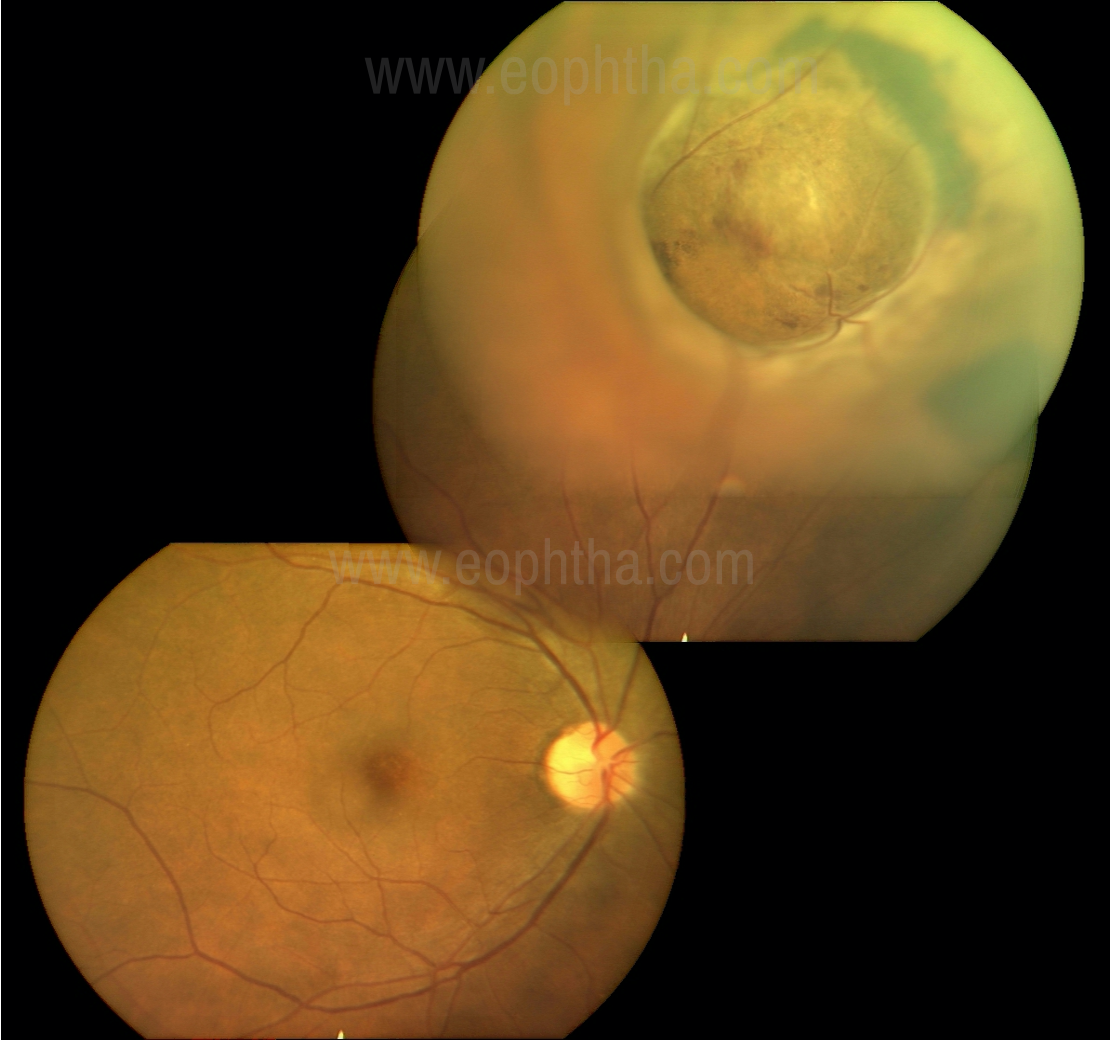
Figure 1:Dome-shaped pigmented melanoma with a smooth surface
Choroidal melanoma appears as a solitary elevated subretinal, without retinal feeder vessels, and often producing retinal detachment. Occasionally, vitreous hemorrhage can develop, obscuring the view of the tumor, requiring ultrasonography. Other signs can include choroidal folds, rubeosis iridis, secondary glaucoma and cataract.
Choroidal melanoma is clinically grouped into three sizes based on the tumor thickness-small (0–3.0mm), medium (3.1–8.0mm), and large (8.1mm or greater) [9]
Investigation
Clinical examination is usually sufficient for diagnosis. Ancillary testing may also be helpful.
USG- Highly accurate and reproducible for diagnosis of ocular melanoma. It is useful in cases of opaque media like in vitreous haemorrhage, exudative bullous retinal detachment. It is used for lesion dimensions, can also detect extra ocular extension. USG findings include internal homogeneity, low to medium internal reflectivity on A- scan, choroidal excavation (produced by the contrast between the normal high reflective choroid surrounding the tumor and the low reflectivity under the densely homogenous tumor mass), sound attenuation due to the densely homogeneous nature of the tumor seen as Acoustic hollowing (Characteristic hyporeflectivity in the basal aspect of the tumor) and the rapid decay of spikes on the A-scan – steep angle kappa, orbital shadowing and in certain cases collar stud/ mushroom-shaped configuration (Image 2). Sometimes internal blood flow can be demonstrated as flickering spikes on A-scan.
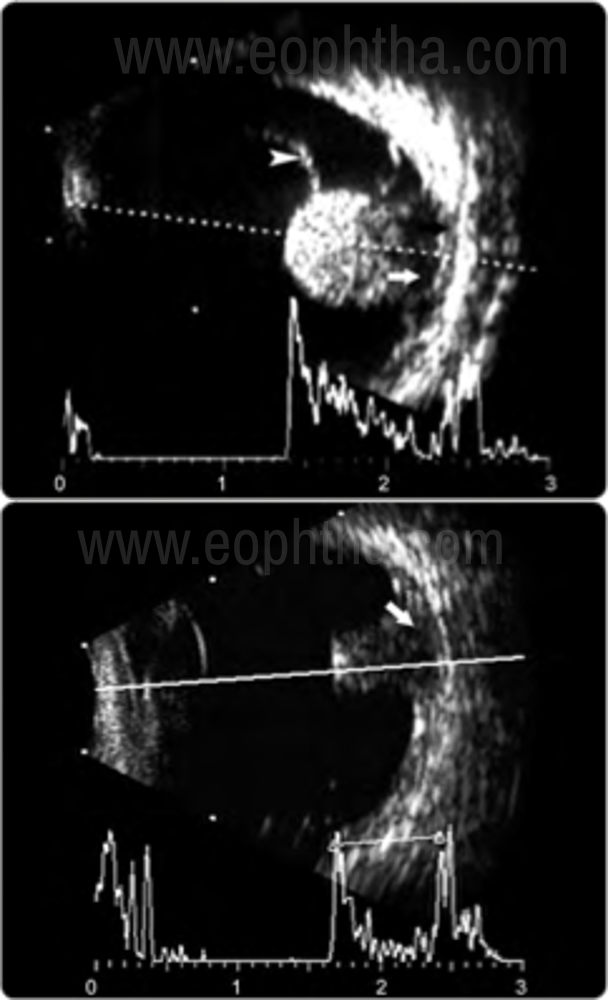
Figure 2: USG Bscan CHaracteristics of Melanoma
Highly accurate and reproducible for diagnosis of ocular melanoma
Can detect tumors ≥ 2 mm
Acoustic properties:
- Soild mass
- Dome shaped or mushroom collar button configuration due to tumor growth through a ruptured Bruch’s membrane.
- Regular internal structure on B scan
- Low to medium internal reflectivity on A scan
- Demonstrable internal blood flow seen as flickering spikes on the A scan.
FA- useful in the differential diagnosis of simulating lesions. Intrinsic tumor circulation (Dual circulation)- the superimposition of the intravascular fluorescence of the intact retinal vasculature over the fluorescence of large-caliber vessels within the choroidal tumor, Mottled Fluorescence in AV phase, late diffuse leakage and staining (Image 3).
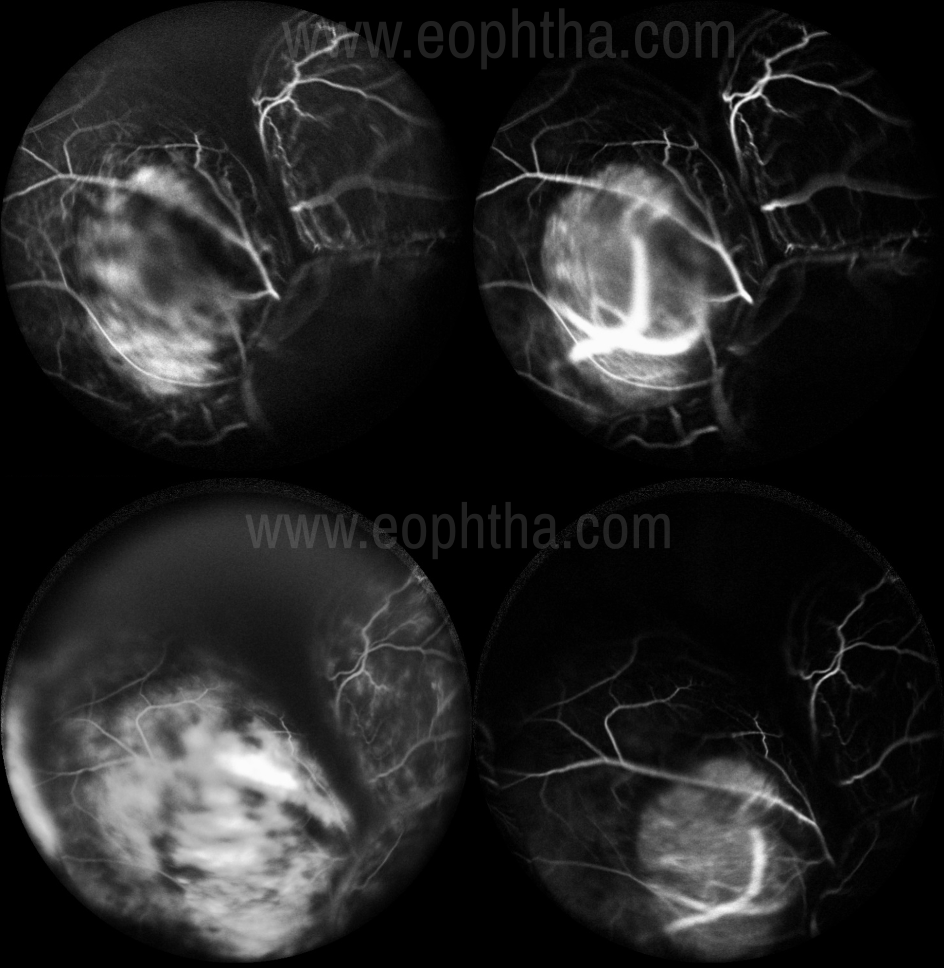
Figure 3:FFA ICG- depicting Dual Circulation with late diffuse leakage and staining
FAF- Can have diffuse or confluent Hyperautofluorescence.
OCT- Can depict secondary changes in the retina overlying the tumor. Small choroidal melanoma shows smooth, moderately dome‑shaped topography, commonly with overlying shallow subretinal fluid that often depicted “shaggy” photoreceptors. EDI-OCT is a useful tool for differentiating choroidal nevus from small choroidal melanoma.
ICG – Hypofluoresence throughout the study.
MRI- Shows Contrast enhancement, T1 Image – tumor appears Bright Hyperintense relative to the darker vitreous, T2 Image- appears Dark Hypointense, useful for dimensions and extraocular extension. Scleral channels and vortex vein invasion can lead to orbital spread.
Recently shield’s et al emphasized the role of multimodal imaging to detect risk factors for transformation of a choroidal nevus into melanoma. [10] Transformation of choroidal nevus into melanoma is estimated at 1 in 8845. [11]
Increasing number of risk factors imparts greater risk for nevus transformation into melanoma
These factors can be recalled by the mnemonic “To Find Small Ocular Melanoma Doing IMaging” (TFSOM-DIM).
Table 1 Clinical Risk Factors for nevus growth to melanoma using MULTIMODAL IMAGING
|
Mnemonic |
Letter |
Variable |
Imaging Modality |
KM 5 yr Growth |
Hazard Ratio |
|
To |
T |
Thickness > 2 mm |
US |
11% |
7.8 |
|
Find |
F |
Fluid |
OCT |
26% |
2.7 |
|
Small |
S |
Symptoms VA<20/50 |
VA Chart |
27% |
2.1 |
|
Ocular |
O |
Orange Pigment |
AF |
9% |
3.2 |
|
Melanoma |
M |
Melanoma Hollow |
US |
37% |
2.1 |
|
Doing IMaging |
DIM |
DIaMeter > 5 mm |
Photograph |
12% |
NS |
Table 2 Risk depends on Number and Combination of Risk Factors
|
# Factors |
KM 5 yr Growth |
Hazard Ratio |
|
0 |
1% |
<1 |
|
1 |
11% |
3 |
|
2 |
22% |
11 |
|
3 |
34% |
15 |
|
4 |
51% |
15 |
|
5 |
55% |
26 |
|
6 |
NE |
ME |
Pathology
Uveal melanoma is composed of anaplastic melanocytic cells with a High N/C ratio, prominent nucleoli and frequent mitotic figures.
The most commonly used histologic classification of uveal melanomas is the MODIFIED CALLENDER CLASSIFICATION [12], which divides uveal melanocytic tumors into the following groups:
- Spindle cell nevi
- Spindle cell melanomas- less anaplasia, favourable survival prognosis
- Mixed cell melanomas- Mixture of small epitheloid cells and spindle cells, further subdivided into groups based on the percentage and size of the epithelioid cells. Tumors with predominantly epithelioid cells have unfavourable prognosis.
Melanoma Genetics
TUMOR GENETICS is Done by Sampling with Fine needle aspiration Biopsy into the tumor and
then Using DNA or RNA Analysis to find the Cytogenetics or the Gene expression profiling.
|
DNA Cytogenetics |
RNA – Gene Expression Profiling |
|
Chr 3 – Poor Prognosis |
Class 1 – Good Prognosis |
|
Chr 6 – Good Prognosis |
Class 2 – Poor Prognosis |
|
Chr 8 – Poor Prognosis |
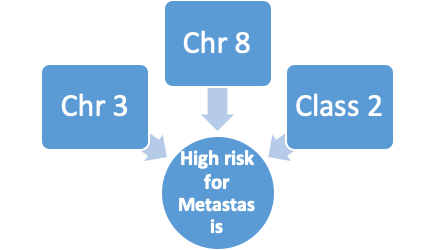
Two classes of uveal melanoma, class 1 and 2 were identified on mRNA analysis by gene expression profile (GEP)
- Class 1 tumors -
- Associated with disomy 3, and chromosome 6p gain
- are considered low-risk tumors
- Class 2 tumors -
- associated with monosomy 3
- are considered high-risk tumors with a greater rate of metastasis and melanoma-related mortality
In a study of 459 patients with uveal melanoma from 12 oncology centers, a strong association was noted between GEP and prognosis of uveal melanoma, with 1% metastasis in class 1 cases and 26% metastasis in class 2 cases at a median follow-up of 17 months. [20]
Classification
The Cancer Genome Atlas (TCGA) Classification [13]. Recently a simple, easy to understand classification has been devised. It is highly predictive plays an important role in selecting high-risk patients for adjuvant therapy protocols.
|
Class A |
Class B |
Class C |
Class D |
|
|
Definition |
Disomy 3 Disomy 8 |
Disomy 3 8q gain |
Monosomy 3 8q gain |
Monosomy 3 8q gain multiple |
|
# (%) |
342 (52%) |
91 (14%) |
118 (18%) |
107 (16%) |
|
Risk for Metastasis (4 yr) |
3% |
10% |
25% |
41% |
|
5 yr Metastasis Hazard Ratio |
1 |
4.1 |
10.1 |
30.0 |
Metastatic Evaluation
Posterior uveal melanoma has a high tendency to metastasize and is associated with high mortality rates. Despite excellent local ocular tumor control for primary UM in the era of plaque radiotherapy, death resulting from the metastatic disease remains prevalent, with metastasis in nearly 50% of all patients.[14] It hematogenously spreads to the liver(most common site), bone, and lungs. The COMS study reported liver metastasis with median survival once metastasis was diagnosed between 6 and 12 months. Systemic monitoring with physical examination and liver function tests twice yearly and chest radiograph and liver imaging using MRI or ultrasonography annually is advised [9].
Poor prognosis with uveal melanoma depends on several factors, such as tumor location in the ciliary body, large tumor size, diffuse (flat) configuration, and Extra Ocular Extension.
COMS
The Collaborative Ocular Melanoma Study (COMS) was designed to evaluate the management of choroidal melanoma in a prospective fashion.
Melanoma classified by these guidelines from the Collaborative Ocular Melanoma Study (COMS):
- Small: 1.5 -2.4 mm in height and 5-16 mm in diameter
- Medium: 2.5 - 10 mm in height and ≤16 mm in diameter
- Large: >10 mm in height and >16 mm in diameter
Tumor located within 2 mm of the optic disc
The COMS comprised three substudies including the large, medium, and small choroidal melanoma trials. The large tumor trial showed no difference in patient’s survival when comparing enucleation vs. preenucleation radiation groups [15]. Five-year Kaplan–Meier estimates for survival were 57% for the enucleation group and 62% for the pre-enucleation radiation group. The medium tumor trial showed no difference in patient’s survival when comparing enucleation vs. plaque radiotherapy [16]. The cumulative all-cause mortality at 12 years was 43% for patients in the plaque radiotherapy group vs. 41% for those in the enucleation group. The small tumor trial showed that small choroidal melanomas managed by observation showed tumor growth in 21% by 2 years and 31% by 5 years [17].
3 Major COMS Trials |
|||
|
COMS Group |
Small |
Medium |
Large |
|
Study type |
Non-randomized, Prospective |
Randomized, Prospective |
Randomized, Prospective |
|
#N |
204 |
1317 |
1003 |
|
Objective |
To describe the time to tumor growth and characteristics associated with growth of small tumors. |
I-125 Brachytherapy vs. Enucleation for treatment of medium tumors. |
Pre-enucleation radiation vs. Enucleation alone for treatment of large tumors. |
|
Notable Findings |
21% grew by 2 years 31% grew by 5 years Characteristics associated with growth: initial thickness and diameter, lipofuscin, absence of drusen, absence of RPE changes |
No clinically statistically significant difference in survival between the 2 treatments for up to 12 years after treatment |
No significant difference in survival between the 2 treatments Age and largest basal diameter prognostic |
Pseudomelanoma
There are conditions that can clinically simulate melanoma, leading to diagnostic ambiguity. The most frequent included choroidal nevus, melanocytoma, peripheral exudative hemorrhagic chorioretinopathy (PEHCR), congenital hypertrophy of the retinal pigment epithelium (CHRPE), idiopathic hemorrhagic detachment of the retina or retinal pigment epithelium, circumscribed choroidal hemangioma, posterior scleritis, and age-related macular degeneration. The most common pseudomelanoma, choroidal nevus can have remarkably similar appearance to small choroidal melanoma. Melanoma typically shows growth over time, whereas nevus is usually stable. Using the aforementioned clinical risk factors (Table 1), melanoma can generally be differentiated from nevus. Melanocytoma is a maximally pigmented magnocellular nevus. It is more common near optic disc; can occur anywhere. Its malignant transformation is rare. Circumscribed choroidal hemangioma typically presents as a posteriorly localized smooth orange mass, can be differentiated using FFA and ICG. Posterior scleritis can also present with a large elevated lesion over the posterior pole, in contrast to melanoma it is associated with pain and other inflammatory signs, choroidal folds can be seen. USG can be used to differentiate it from melanoma. It has thickened sclera and choroid, retrobulbar edema, T-sign, and high internal reflectivity on USG.
Management
The extent to which ocular treatment influences survival is not yet defined. The management of melanoma is individualized depending on the tumor size, tumor location, associated features, status of the opposite eye, patient’s systemic status, and patient’s desire. Small tumors can be observed with periodic fundus photography and ultrasound.(This is debatable in today’s era, and most oncologists tend to treat). Risk factors for metastasis should be assessed. Management choices for choroidal melanoma include transpupillary thermotherapy, plaque radiotherapy, charged particle irradiation, local resection, enucleation, or orbital exenteration [18,19].
Transpupillary Thermo Therapy is useful as a primary treatment for a very limited group of patients with small pigmented choroidal melanoma, especially those near the fovea or optic disc. It can also be used as a secondary treatment to plaque radiotherapy for medium to large choroidal melanomas and even some small tumors that touch the optic disc. The two most frequently employed treatments for choroidal melanoma include enucleation or focal radiotherapy, using plaque radiotherapy or proton beam radiotherapy.
Brachytherapy involves the application of radiation from isotopes over very short distances in contact with a surface. The most commonly used sources are iodine-125, ruthenium-106, and palladium-103. Plaques consist of gold housing and seed carrier insert. It can be offered to those with small and medium-sized tumors outside the retinal vascular arcade and posterior to ora serrata.
Enucleation is an option in patients with large tumor size, Neovascular glaucoma, Optic nerve invasion, Blind painful eye, Localized extra scleral extension, Medium-sized tumors with poor visual potential, or because of patient preference.
Those with massive orbital extension require eyelid sparing extenteration, which provides good cosmetic appearance.
Newer treatments include
Target therapy - Light-activated AU-011 – a novel virus like particle drug conjugate administered through intravitreal injection and activation by laser to produce targeted, rapid, tumor necrosis while sparing healthy ocular tissue
Immunotherapy – Ipilimumab, Nivolumab, Dendritic cell vaccine
References
1.Strickland D, Lee JA.Melanomas of eye: stability of rates. Am J Epidemiol. 1981;113(6):700–2.
2.Aronow ME, Topham AK, Singh AD. Uveal melanoma: 5-year update on incidence, treatment, and survival (SEER 1973–2013). Ocul Oncol Pathol. 2018;4(3):145–51.
3.Singh AD, Turell ME, Topham AK. Uveal melanoma: trends in incidence, treatment, and survival. Ophthalmology. 2011;118(9):1881–5.
4. Manohar S, Ramachandran R, Das T, Namperumalsamy P. Malignant melanoma of choroid. Indian J Ophthalmol 1991;39:70-73.
5. Seddon JM, Evangelos S, Gragoudas, Host factors, UV radiations and Risk of uveal melanoma. A case-control study. Arch Ophthalmol 1990;108:1274-80.
6. The collaborative ocular melanoma study (COMS) randomised trial of pre-enucleation radiation of large choroidal melanoma. I: Characteristics of patients enrolled and not enrolled. COMS report No.9. Am J Opthalmol 1998;125:767-78.
7. Weis E, Shah CP, Lajous M, et al. The association of host susceptibility factors and uveal melanoma. A meta-analysis. Arch Ophthalmol 2006; 124:54–60.
8. Shah CP, Weis E, Lajous M, et al. Intermittent and chronic ultraviolet light exposure and uveal melanoma. A meta-analysis. Ophthalmology 2005; 112:1599–1607.
9. Shields, Carol L.; Manalac, Janet; Das, Chandana; Ferguson, Kyle; Shields, Jerry A.Choroidal melanoma: clinical features, classification, and top 10 pseudomelanomas, Current Opinion in Ophthalmology: May 2014 - Volume 25 - Issue 3 - p 177-185
10. Shields, Carol L. MD; Dalvin, Lauren A. MD; Ancona-Lezama, David MD; Yu, Michael D. BS; Di Nicola, Maura MD; Williams, Basil K. Jr MD; Lucio-Alvarez, J. Antonio MD; Ang, Su Mae BS; Maloney, Sean BS; Welch, R. Joel MD; Shields, Jerry A. MDCHOROIDAL NEVUS IMAGING FEATURES IN 3,806 CASES AND RISK FACTORS FOR TRANSFORMATION INTO MELANOMA IN 2,355 CASES, Retina: October 2019 - Volume 39 - Issue 10 - p 1840-1851
11. Singh AD, Kalyani P, Topham A. Estimating the risk of malignant transformation of a choroidal nevus. Ophthalmology 2005;112:1784‑9.
12. McLean IW, Foster WD, Zimmerman LE, Gamel JW. Modifications of Callender's classification of uveal melanoma at the Armed Forces Institute of Pathology.Am J Ophthalmol. 1983;96(4):502‐509. doi:10.1016/s0002-9394(14)77914-0
13. Vichitvejpaisal, P. et al. Genetic analysis of uveal melanoma in 658 patients using the cancer genome atlas classification of uveal melanoma as A, B, C, and D.Ophthalmology126, 1445–1453 (2019).
14. Coupland SE, Lake SL, Zeschnigk M, et al. Molecular pathology of uveal melanoma. Eye (Lond). 2013;27(2): 230e242.
15. The Collaborative Ocular Melanoma Study Group. The Collaborative Ocular Melanoma Study (COMS) randomized trial of preenucleation radiation of large choroidal melanoma II: initial mortality findings. COMS report no. 10. Am J Ophthalmol 1998; 126:779–796.
16. CollaborativeOcularMelanoma Study(COMS)Group. TheCOMSrandomized trial of Iodine 125 brachytherapy for choroidal melanoma. V. Twelve-year mortality rates and prognostic factors: COMS report no. 28. Arch Ophthalmol 2006; 124:1684–1693.
17. The Collaborative Ocular Melanoma Study Group. Factors predictive of growth and treatment of small choroidal melanoma. COMS report no. 5. Arch Ophthalmol 1997; 115:1537–1544.
18. Shields JA, Shields CL. Intraocular tumors. An atlas and textbook. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2008; pp. 59–196.
19. 19Shields CL, Shields JA. Surgical removal of intraocular tumors: dismissing old wives’ tales. Am J Ophthalmol 2013; 156:3–4.
20. Onken MD, Worley LA, Ehlers JP, Harbour JW. Gene expression profiling in uveal melanoma reveals two molecular classes and predicts metastatic death. Cancer Res. 2004;64(20):7205–7209.
21. Shields CL, Kaliki S, Furuta M, et al. Clinical spectrum and prognosis of uveal melanoma based on age at presentation in 8033 cases. Retina 2012; 32:1363–1372.