

Brief Scenario of the case:
Decreased vision in the right eye in a 20-year-old high myopic female
History of Present Illness:
The patient is a 20-year-old female who presented with decreased vision in the right eye for 8 months. No history of headache, ocular pain, redness, and trauma were reported. She had no visual changes or symptoms in the left eye.
Past Ocular History: High myopic using glasses
Past Medical History/ History of Medication: No ophthalmic or systemic use of medication. No history of any substance abuse.
Allergy history: No known drug allergies or any other allergies.
Family History: History of mother having high myopic glasses since childhood. No significant family history of systemic diseases.
Review of Systems/Systemic Examination:
Systemic examinations within normal limits.
- Pulse: 72/min, regular
- BP: 100/70 mm of Hg
- ECG: WNL
- RBS: 113 mg%
- Chest X-Ray: WNL
OCULAR EXAMINATION
Best Corrected Visual Acuity (Snellen chart)
- Right eye (OD): PL+ PR accurate
- Left eye (OS): 20/20
Ocular Motility/Alignment :Full and free in all gazes
Intraocular Pressure (Applanation tonometry)
- OD: 8 mmHg
- OS: 16 mmHg
Pupils:
OD: RAPD
OS: Reactive to light
|
|
OD |
OS |
|
Best-corrected visual Acuity |
PL+ PR accurate |
20/20 (-5.5 DS) |
|
Intraocular Pressure |
8 mmHg |
16 mmHg |
|
Pupil Examination |
Relative afferent pupillary defect (RAPD) |
Reactive to light |
|
Motility |
Full |
Full |
|
External Examination |
Normal |
Normal |
|
Slit-lamp Examination |
Lids/Lashes: Normal |
Lids/Lashes: Normal |
|
Fundus Examination |
Disc: seen |
Disc: Normal |
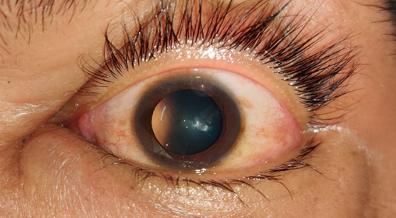
This is the preoperative anterior segment photo of the right eye showing early localized lenticular changes.
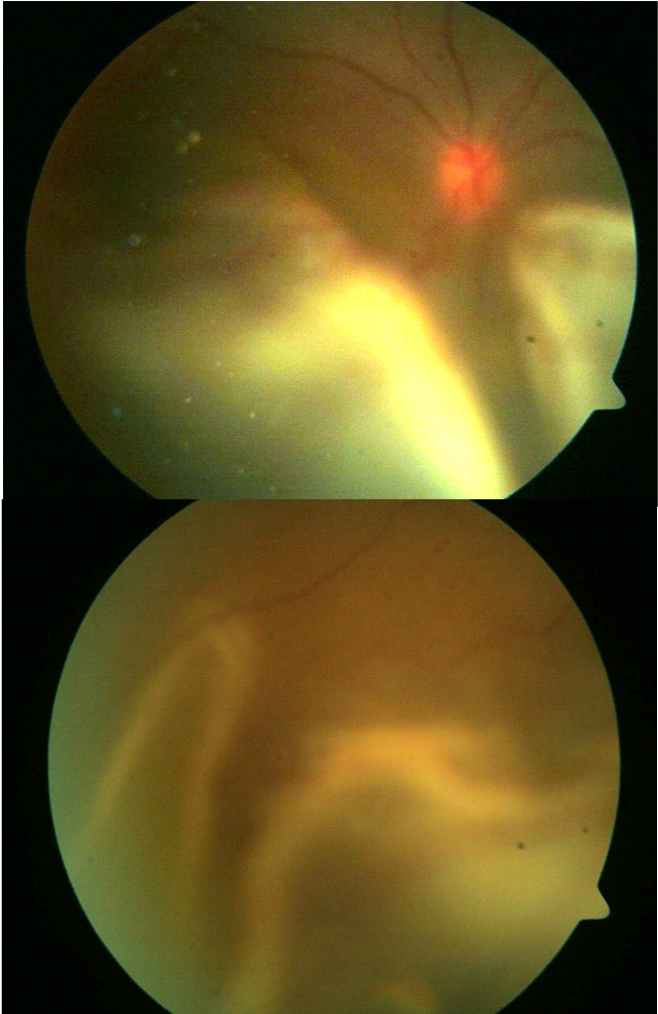
This is the pre-operative fundus photo of the right eye showing total bullous retinal detachment.
This is the post-operative fundus photo of the right eye showing PVR changes inferiorly.
Ancillary Investigations:
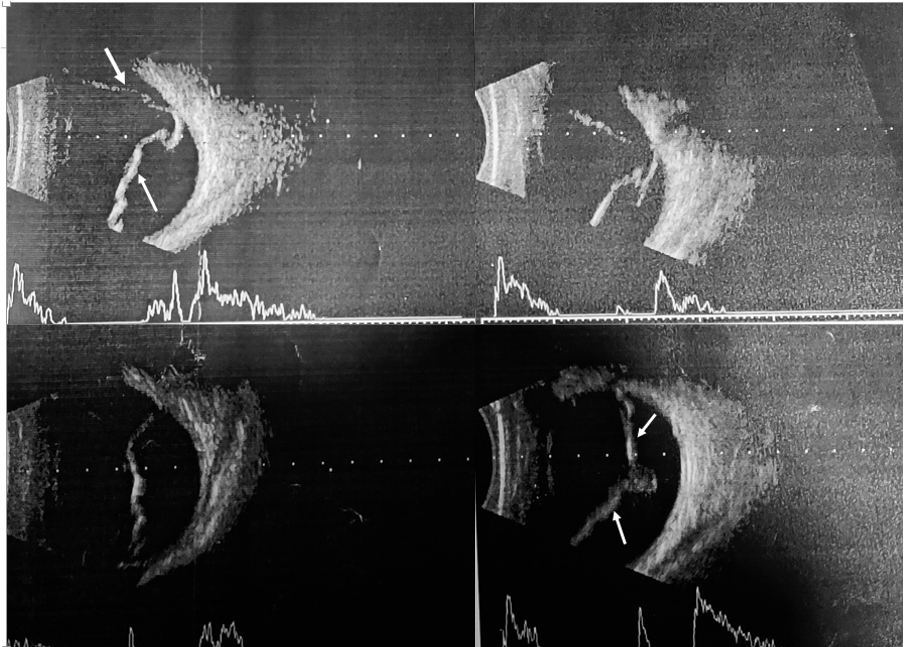
B-Scan USG was done to rule out peripheral choroidal detachment as IOP was low (8 mmHg). The above figure shows a thick membrane with few cystic changes (white arrows), which shows low mobility, A-scan spike, and attachment to optic nerve head.
Differential Diagnosis:
1.Retinoschisis
2.Choroidal detachment / ciliochoroidal or choroidal effusion
3.Uveal effusion syndrome
4. VKH
Diagnosis: Right eye early lenticular changes with Total chronic retinal detachment with proliferative vitreous retinopathy
Clinical Course of the condition
The 20-year-old myopic female patient was evaluated in the eye clinic 8 months after her initial onset of symptoms. Her visual acuity was recorded as PL+PR accurate in the right eye and 20/20 with glasses in the left eye. Her intraocular pressure was low in the right eye, 8 mmHg, the other eye being normal. On fundoscopy, the right eye was noted to have total retinal detachment (bullous) with proliferative retinopathy inferiorly. B-scan was performed to rule out the possibility of peripheral choroidal detachment. She was advised for the pars plana vitrectomy with encirclage buckle along with endolaser and silicone oil injection under local anesthesia.
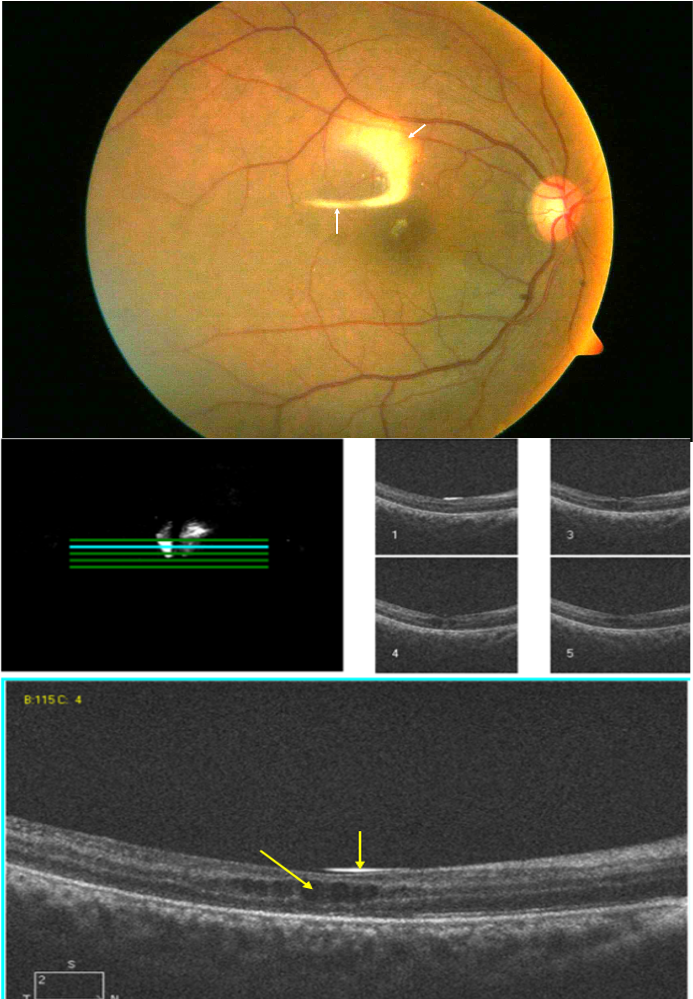
This is the post-op 1 month Fundus photo (OD) showing attached retina and silicone reflex (white arrow) post-surgery.
This is the post-op 1 month OCT (OD) showing silicone oil reflex (yellow arrow) and cystoid degenerative changes (red arrow) in the outer plexiform layer of the retina.
DISCUSSION
Epidemiology/ Etiology: Rhegmatogenous retinal detachment (RRD) incidence demonstrates significant geographical variation and its incidence has been reported to be between 6.3 and 17.9 per 100 000 population. Retinal detachment is defined as a separation of the neurosensory epithelium and the retinal pigment epithelium (RPE). The rhegmatogenous term is derived from the Greek word rhegma, meaning a discontinuity or a break or a tear; therefore, RRD is characterised as retinal detachment due to tear or break or hole in the retina in association with /following vitreoretinal traction leading to seepage and accumulation of subretinal fluid in the potential subretinal space I.e. between neurosensory retina and RPE.
Risks factors :
- Age: More common in 55-70years of age, although age is no bar.
- Sex: more common in males (M: F- 3:2)
- Myopia (axial myopia): over 40% of RRD cases are reported in myopic and risks is directly proportional to the degree of refractive error in myopes. Refractive correction of -3 D increases the risk of RD fourfold.
- Trauma: blunt ocular trauma leading to tearing of the retina. The rate is comparatively low.
- Aphakia and Pseudophakia: The risk increases for pseudophakic RD if associated with intraoperative manipulations, vitreous loss, nucleus drop, or post-op YAG capsulotomy.
- Retinal degenerations: Lattice degeneration is 6-10% common in the general population and 15-20% in myopic patients being bilateral in 50% of cases.
- Family or genetic history of RD
- History of inflammatory ocular diseases like Eales disease, chronic uveitis, etc. as they lead to liquefaction of vitreous gel.
Pathophysiology :
For the occurrence of RRD, essential factors required are:
- Liquefaction of vitreous gel
- Tractional forces inducing retinal tears
- Retinal break allowing seepage of liquid vitreous into Subretinal Space.
Myopia and old age commonly leads to Synchysis i.e. splitting of vitreous or liquefaction of vitreous gel
↓
Vitreous syneresis
↓
Posterior vitreous detachment
↓
Vitreoretinal traction
↓
Retinal tear
↓
Seeping of liquefied vitreous into subretinal space
Leading to an accumulation of subretinal fluid downwards because of gravitation. Through Lincoff's rule, the site of a retinal tear is located and the final shape and position of retinal detachment are thus determined.
↓
Causing reduction in vitreous volume
↓
Low IOP explaining cause of hypotony in RD
↓
If untreated can lead to phthisis bulbi
Clinical Features :
Symptoms - In the initial stages, the symptoms may be non-specific due to shallow detachment. Most of the patients complainof floaters or dark spots (muscae volitantes ) and photopsia (flashes of light). Floaters can occur because of the rapid posterior vitreous degeneration. Photopsia occurs because of the retinal traction causing irritation to the retinal neuroepithelium. Photopsia is not found in other types of RD. After a period of time, the sudden appearance of a dark cloud or veil or curtain in front of the visual field can occur if the detachment occurs posterior to the equator. Sudden painless loss of vision can occur if fovea is involved or there is a large bullous RD.
Signs - RAPD is present in the case of total RD. IOP is usually low (hypotony). If it is extremely low, it can be associated with choroidal detachment. Rarely high IOP is also noted in the case of Schwartz - Matsuo syndrome due to migration of degenerated photoreceptor cell or RPE pigments anteriorly which block the normal trabecular outflow. Iritis is common, but usually, it is mild. The anterior chamber may have some cells and flare. Distant direct Ophthalmoscopy shows a grey reflex in the quadrant of the detached retina (normally pink-red reflex is present), mobility of retina is present along with retinal folds (Proliferative vitreous retinopathy), which oscillate with the movement of the eye. Vitreous pigments or tobacco dust are present in the anterior vitreous called the Shaffer sign. Retinal tears or breaks are present in various forms like horse-shoe( most common), round, slit-like, or large anterior dialysis, or giant retinal tear if occupying more than one quadrant of the whole circumference. Retinal breaks are most commonly found in the superotemporal quadrant.
Chronic cases of RD show retinal thinning due to atrophy, intraretinal cysts, and subretinal demarcation lines( high water or tide marks) due to proliferation of RPE cells at the junction of a flat and detached retina.
Complications - This usually occurs in long-standing cases.
- Complicated cataract -as nutrition is affected in long-standing cases.
- Phthisis bulbi due to hypotony
- Uveitis leading to secondary glaucoma
- Proliferative vitreous retinoscopy - RD repair surgery further increases the risk for PVR.
Ancillary Investigation: Diagnosis is based on ophthalmoscopy or fundoscopy using scleral indentation (to enhance visualization of peripheral retina anterior to the equator).
B-scan- It is a non-invasive diagnostic tool used to look for posterior segment lesions of the eye. RRD appears as a free-floating membrane in the vitreous cavity or funnel-shaped in case of total RD (hyperechoic) with high reflectivity/spike on A-scan having an attachment at the disc.
Optical Coherence Tomography ( OCT)- It can be used to assess detailed cross-sectional views of the retina especially the foveal architecture.
Visual Field Testing - Although uncommon, visual field charting (especially by confrontation testing) can be helpful to assess the subretinal fluid level and primary location of the retinal tear by revealing the scotoma or visual field defect occurring first.
Treatment :
RD is one of the vision-threatening emergencies which should immediately be treated. If left untreated, it can lead to blindness.
Prophylaxis of RD can be done by identifying the areas of retinal breaks and predisposing lesions like lattice degeneration and treating them with the application of cryotherapy or laser photocoagulation in patients associated with high-risk factors like high myopia, family history of RD, RD in the fellow eye, aphakia, etc.
Surgical management: Various procedures have been utilized for the management of RD. The basic principle in all types of RD surgery is first sealing the retinal breaks by creating aseptic chorioretinitis then releasing any vitreous or pre-retinal traction, drainage of SRF and then maintaining chorioretinal apposition through external or internal tamponade. Sealing of retinal breaks is done by creating aseptic chorioretinitis through cryocoagulation or laser photocoagulation.
The common types of procedures used today are:
- Pneumatic retinopexy- In this procedure, an intravitreal gas is injected trans-conjunctivally, coupled with cryotherapy or laser photocoagulation to provide apposition of the retinal break against the RPE. Most common gases used are SF6 ( sulphur hexafluoride) OR C3F8 (perfluoropropane).
- Scleral buckling- This procedure provides an external tamponade by inward indentation of sclera towards the detached retina. It is done by insertion of explants ( silicone sponge or soft silicone encircling band) with mattress sutures. Complications include diplopia, cystoid macular edema, buckle extrusion ,intrusion or infection, choroidal detachment, raised IOP, ant.segment ischaemia, surgical failure.
- Vitrectomy- It is becoming the standard of care with promising results and faster rehabilitation. It involves three-port vitrectomy through pars plana approach allowing complete vitreous removal and providing tamponade with gases like SF6 or C3F8 or silicone oil. Gases gradually get absorbed over a duration of time, but silicone oil needs to be removed later on follow-up. If SO left unremoved can cause worse visual outcome.
Complications of RD Surgery:
- Persistent detachment or re-detachment
- Increase risk of PVR, Macular pucker
- Diplopia because of damage to extraocular muscles
- Anterior segment ischemia
Rhegmatogenous Retinal Detachment |
|
|
Etiology
|
Signs
|
|
Symptoms
|
Differentials
|
|
Investigations -
|
Treatment -
|
Comments