


Introduction:
Scleral buckle surgery is indicated for uncomplicated rhegmatogenous retinal detachments. Scleral buckling indents the sclera and the overlying choroid retinal pigment epithelium complex towards the retinal break in the detached retina, resulting in retinal reattachment. Scleral buckle surgery evolved out of the works of Jules Gonin, who identified retinal breaks as the cause of retinal detachment, Custodis, Lincoff and Schepens who devised ways of using an epi / intrascleral implant to “buckle” the sclera inward to create the indent.1-3
Principles of scleral buckling:
The aim of scleral buckling is to close all retinal breaks to achieve permanent reattachment of the retina. General principles of retinal detachment surgery- Search for the breaks, find all the breaks, seal all the breaks, and relieve vitro retinal traction.
This is achieved by -
- Identification of the retinal break
- Retinopexy – creating a sterile inflammatory reaction that would result subsequently in chorioretinal adhesion that seals the retinal break
- Relief of vitreoretinal traction by indenting the sclera towards the retinal break and closure of the break
Indications:
Uncomplicated rhegmatogenous retinal detachment up to proliferative vitreoretinopathy (PVR) grade C1.
Scleral buckling is preferred in
- Young patients with adherent posterior hyaloid
- Phakic eyes4
- Retinal detachment associated with retinal dialysis5
Relative contraindications
- Retinal detachment with PVR > grade C1
- Coloboma choroid associated retinal detachment6
- Posterior retinal breaks (can be judged in the clinic by scleral depression. Breaks difficult to access by scleral depression, even with the eye in the primary position may be difficult to treat by scleral buckling)
- Extreme scleral thinning
- Opaque media – wherein retinal breaks may be missed
- Retinal detachment in pseudophakic eyes – Comparative studies indicate better surgical results with vitrectomy in pseudophakic rhegmatogenous retinal detachment.4
- Rhegmatogenous retinal detachment associated with peripheral retinal break and macular hole
- Prior squint surgery (recession of muscle) in the quadrant requiring scleral buckling
- Combined traction rhegmatogenous retinal detachments
- Patients with a potential vaso-occlusive disease such as sickle cell disease as it may increase the risk of anterior segment ischemia.7
- Post-glaucoma surgery wherein peritomy can compromise the bleb or in the presence of a glaucoma implant which can interfere with the buckle placement; advanced glaucomatous optic atrophy wherein the possible temporary elevation of intraocular pressure due to scleral buckle can compromise the remnant field; medically uncontrolled glaucoma which may necessitate anti-glaucoma surgery.
Surgical techniques
Scleral buckling may be only segmental wherein a segmental buckling element (tire) is placed episclerally over the lesion; an encircling element is not placed. A silicone tire with an encircling band is preferred in eyes with peripheral retinal degeneration and /or multiple breaks or vitreous traction in multiple quadrants.
Scleral buckling can be performed under peribulbar, parabulbar or retrobulbar anesthesia; general anesthesia being preferred for children and apprehensive adults. A mixture of lignocaine 2% and bupivacaine 0.5% with hyaluronidase 7.5units/ml and 1:10000 adrenaline is used for anesthesia. Pre-operative antibiotic prophylaxis is usually not necessary; instillation of Povidone Iodine 5% eye drops in the conjunctival cul-de-sac prior to surgery is however, required.
An adjustable lid speculum is used to keep the lids open after cleaning the eye and periorbital areas with Povidone Iodine 10% solution and draping the eye.
Peritomy: A 3600 limbal peritomy is performed if an encircling band is to be placed. If a segmental buckle is planned without an encircling band, peritomy is limited to the quadrant of the episcleral explant. The limited peritomy however extends 1 clock hour beyond the quadrant on either side to facilitate muscle tagging. The tenon conjunctival adhesions are lysed in the four quadrants by introducing the tip of the blunt curved scissors, hugging the sclera, and opening the blades.
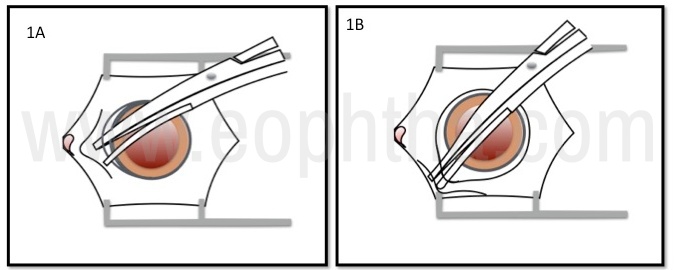
Figure 1A- A 3600 limbal peritomy is performed. 1B- The tenon conjunctival adhesions are lysed.
Muscle tagging: The four recti muscles are tagged with 2’0 silk sutures, aided by muscle hooks with eyelets. Sweeping the muscle hook close to the insertion of the muscle will avoid inadvertent hooking of vortex veins. It is preferable to hook the superior rectus from the medial to the lateral side to prevent inadvertent tagging of superior oblique muscle. The intermuscular fascia is wiped posteriorly with a cotton tip applicator and the quadrants are inspected, looking for areas of scleral dehiscence, anomalous insertion of vortex veins and staphyloma. Scleral dehiscence appears as radial areas of scleral thinning through with the underlying choroidal pigmentation shines through. (Figure 1)
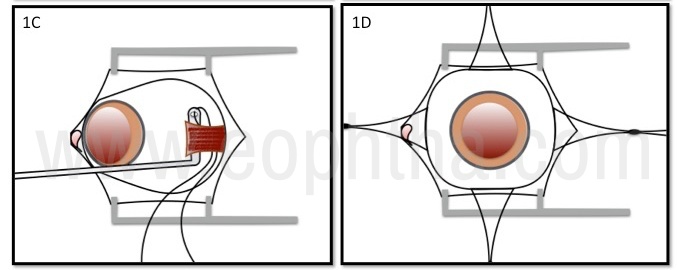
Figure 1C- Muscle tagging. 1D- All the 4 recti tagged
Localization: The retinal breaks and areas of lattice degeneration in the detached retina are localized with the aid of indirect ophthalmoscope. A diathermy, cautery, or a marking pen is used to mark the area of the retinal break on the sclera.
- Three-point localization is used to localize a horse-shoe tear – the two horns and the apex of the horse-shoe tear.
- A point localization for an atrophic hole.
- The lateral and the posterior-most extent are localized in case of lattice degeneration. (Figure 2)
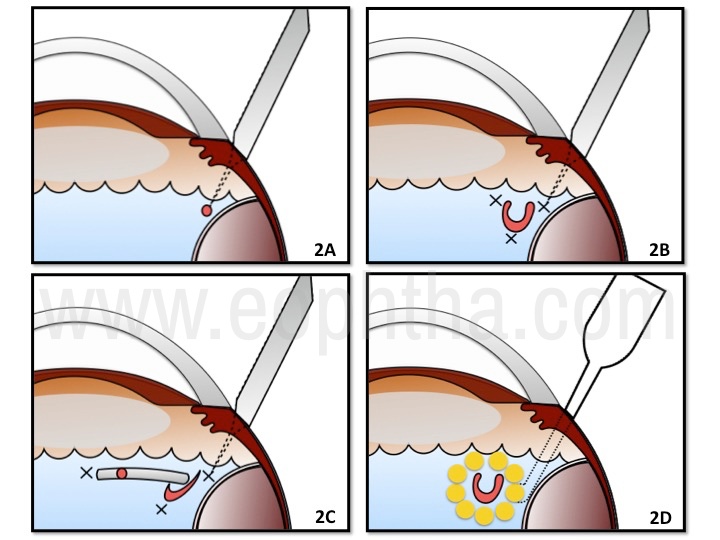
Figure 2: Localization point indicated by cross, 2A- A point localization for an atrophic hole. 2B- Localization of a horse-shoe tear – the two horns and the apex of the horse-shoe tear. 2C- The lateral and the posterior-most extent are localized in case of a lattice degeneration with breaks. 2D- Cryo edema around the horse-shoe tear.
Retinopexy: Retinopexy creates a chorioretinal scar thereby sealing the retinal break. This prevents the liquid vitreous from entering the subretinal space through the break, resulting in retinal detachment.
Retinopexy can be performed using
- Cryopexy – Cryopexy is performed under indirect ophthalmoscopic visualization of the fundus. A row of contiguous cryo burns are applied around the retinal break or lattice degeneration, taking care not to treat the bare RPE beneath the retinal break. Treating the bare RPE would result in liberation of the RPE cells, increasing the risk of subsequent proliferative vitreoretinopathy (PVR). The judicious application of cryotherapy involves termination of the cryo application as soon as the iceball touches the retina and not allowing it to freeze the overlying vitreous. The cryo burns are extended to the ora serrata to decrease the risk of recurrent retinal detachment if the tear were to extendanteriorlypost-operatively. Indenting the sclera towards the retina displaces the subretinal fluid and opposes the RPE to the retina, allowing the iceball to extend to the retina that subsequently becomes a strong chorioretinal scar. In case of a bullous retinal detachment, treating the underlying RPE alone or cryotherapy after drainage of subretinal fluid, would prevent unnecessary overtreatment. (Figure 2)
- Laser photocoagulation – intra-operatively with transscleral diopexy probe or the laser indirect ophthalmoscope or post-operatively on the first post-operative day with the laser indirect ophthalmoscope. Laser photocoagulation can be performed only if there is a shallow fluid separating the retina and retinal pigment epithelium (RPE). Hence it can be performed in shallow retinal detachments or after drainage of subretinal fluid.Hence laser is seldom preferred forretinopexy intraoperatively as it can be used only in select cases wherein the retina is opposed to the RPE as in very shallow / no residualsubretinal fluid with orwithout drainage
- Diathermy – Diathermy offers the strongest adhesion between the retina and the underlying RPE / choroid and hence it can be applied in staggered rows of burns 1.5mm apart that need not surround the break. However, diathermy results in shrinkage of the sclera and hence it is applied to the scleral bed after lamellar dissection of the sclera. Diathermy is seldom used, as the lamellar dissection is difficult with increased risk for complications such as scleral rupture.
Scleral Buckling:
Contemporary scleral buckling is performed with solid silicone implants most often. Silicone implants are soft synthetic rubber that is nontoxic and non-allergic. Silicone sponges are used rarely due to the increased propensity for buckle infection, due to presence of interconnecting pores within the implant. Fascia lata, palmaris tendon, plantaris tendon, knee cartilage, donor sclera, dura mater, polyviol, polyethylene, encircling nonabsorbable and absorbable sutures and gelatin have been used in the past for scleral buckling.
The buckle should extend sufficiently around the retinal break to be effective. The buckle should extend 3mm posterior to the break and 2 mm laterally on either side. For anteriorly placed retinal breaks, the buckle extends from the ora and for posterior breaks, an anterior clearance of 3mm is preferable. This measurement decides the selection of the buckle to be used in a particular case. For example for an HST that measures 3 mm X 3 mm from the ora, a 6 mm wide buckle is required with a circumferential extent of 7 mm (Figure 5D). If a similar HST were placed 3mm posterior to the ora a 9 mm wide buckle would be required. The implant parameters such as the width, thickness, symmetric or asymmetric implant, can be obtained from the chart provided by the manufacturer.
An encirclage of 2.5mm width is the most commonly used, when required, in addition to the solid silicone implant. An encirclage is preferred to support the vitreous base in the presence of significant vitreoretinal traction in areas away from the retinal break, as in an eye with extensive lattice degeneration.
The technique of scleral buckling:
Sutured Scleral buckle: A non-absorbable 5’0 braided polyester suture is used to take the mattress suture that secures the implant, “buckling” the sclera inwards.
Scleral buckles may be radially or circumferentially oriented. Radial buckles minimize the development of posterior retinal folds and are preferred for posterior horse-shoe tears. Circumferential buckles are preferred in eyes with multiple retinal breaks or when large areas are to be supported by the buckle.
Figure 3: 3A- Construction of scleral pocket with a crescent blade,3B- Scleral suture to secure encircling silicone band. 3C- 3C- Encircling band secured within scleral pockets andpassedbeneath the recti.3D- Ends of encircling band secured with Watzke sleeve.
For a radial buckle, the intrascleral suture limbs are placed radial to the spiral of Tillaux, parallel to the meridian of the retinal break. The sutures are placed parallel to the limbus/spiral of Tillaux for a circumferential buckle.
The mattress suture is placed 2mm wider than the implant with a spatulated cutting needle, traversing through ~1/2 – 2/3rd of scleral thickness. At least 2 adjacent sutures, the posterior bites extending to 5-6 mm in length each, would be required if the buckle extends up to a quadrant. The needle is passed parallel to the scleral surface, visualizing the needle tip through its intrascleral passage, to minimize the risk of globe perforation. The mattress sutures are tied with temporary knots initially and made permanent once the placement of the buckle is deemed appropriate.
If an encirclage is used, it rests in the pre-existing groove in the buckle, beneath the mattress suture and is secured with either sutures or intrascleral tunnels in other quadrants. The sutures are placed in such a way that the encirclage is able to slide easily beneath the suture. The ends of the encirclage are secured with a clove-hitch knot, a Watzke sleeve, or a tantalum clip. The ends of the encirclage are pulled to tighten it around the sclera creating an indent to counter the vitreous base traction. Usual encirclage is of 2.5mm, commensurate with the groove in the solid silicone buckle. A 4 mm band can also be used in case a broad area of support is required. The encirclage is placed in such a way as to support the vitreous base (2-3mm posterior to spiral or Tillaux); it is also used to support areas of lattice degeneration that is unsupported by the solid silicone implant.
Sutureless buckle (Figure 5A): A sutureless buckle can be used to treat lesions that extend <1½ clock hours. Two adjacent scleral tunnels are created close to the break and the solid silicone implant is placed fitting snugly between the tunnels. When tightened, the encirclage passing between the closely placed tunnels creates the buckle indent.8
Subretinal fluid drainage
In eyes where opposition of the RPE and retina could be obtained with the buckle indent, subretinal fluid (SRF) drainage is not necessary. In fresh retinal detachments, the retina attaches even if the break is separated from the RPE with shallow fluid (~3mm) overlying the buckle indent; the tamponading effect of the overlying gel vitreous aids closure of the break. Other mechanisms such as displacement of SRF away from the break, reduction of vitreoretinal traction achieved by the displacement of the eye wall and retina centrally, post-operative increase in buckle height, increase in resistance to fluid flow through the retinal break and alteration of the shape of the eyeball redirecting the intraocular currents resulting in liquid vitreous entering the retinal break, are mechanisms that may synergistically result in retinal reattachment despite non drainage of SRF. (Figure 4)
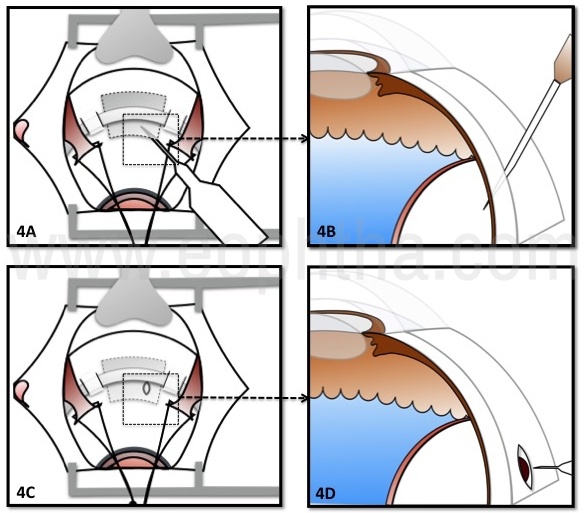
Figure 4: 4A, 4B- Needle drainage of subretinal fluid. 4C, 4D- SRF drainage after scleral cut-down
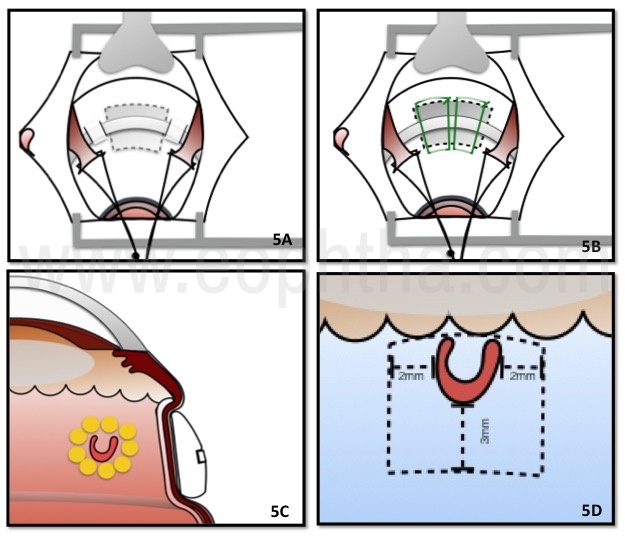
Figure 5: 5A- Solid silicone tire secured in between 2 scleral pockets to induce indent. 5B- Solid silicone element apposed to the sclera by sutures. 5C- Buckle effect 5D- Ideal dimensions of buckling required.
SRF drainage is preferable in
- Eyes with pre-existing glaucoma wherein the elevated intraocular pressure resulting from a non-drainage surgery may aggravate optic nerve damage.
- Chronic retinal detachments
- Bullous retinal detachments
- Retinitis pigmentosa associated retinal detachments
Preferable location of SRF drainage site
- On either side of the horizontal recti due to the relative avascularity of the choroid
- Beneath the area of maximum SRF
- Away from the retinal break – inadvertent drainage of liquid vitreous through the break may result in hypotony and loculated SRF
- Beneath a fixed fold or subretinal gliotic band
- Beneath the buckle
Subretinal fluid can be drained via needle drainage wherein a 26g short needle is used to penetrate the full thickness sclera tangentially, or using a scleral cut-down. In a scleral cut-down a radial incision of 3-4 mm is created, allowing the choroid to prolapse through it. The choroid is penetrated with a needle, diathermy or laser, the last two decreasing the risk of bleeding from the choroidal vessels. Gentle pressure is applied to the globe to combat the hypotony induced by the SRF drainage. Clumps of pigment eschewing out of the drainage site or ooze of blood usually signifies end of drainage and is a sign to secure the site of drainage. If the drainage site is located away from the area of the buckle, the drainage site should be sutured after drainage and a pre-placed suture facilitates this.
The mattress sutures and the encirclage are temporarily tightened after SRF drainage to create the buckle effect. Residual hypotony is managed by intravitreal injection of balanced salt solution or air/gas. The fundus is visualized for
- Ensure patency of the central retinal artery
- SRF drainage site complications
- Appropriate positioning of the scleral buckle beneath the retinal break
- Retinal reattachment
The mattress suture knots are then made permanent, episclera washed with antibiotic solution, and the conjunctiva closed with absorbable sutures.
DACE- Drainage Air Cryo Encirclage
In cases with bullous retinal detachments, localization of the break would be false due to the parallax or breaks that can be hidden in between the retinal folds. The application of the cryo in a detached retina may be difficult. Drainage of the subretinal fluid helps to better identify the breaks and avoid false localization. The SRF can be replaced by either air or fluid injection in the vitreous cavity and cryo application is done and the scleral buckling procedure is completed.
Complications of scleral buckling surgery:
Intra-operative complications
- Disinsertion of extraocular muscle
- Oculo-cardiac reflex resulting in bradycardia during muscle tagging
- Vortex vein disinsertion
- Globe rupture
- Subretinal hemorrhage
- Suprachoroidal hemorrhage / hemorrhagic choroidal detachment
- Retinal incarceration at the site of SRF drainage
- Scleral perforation
- Retinal break
- Vitreous loss
- Fish-mouthing of the retinal break (though the break is on the buckle, it remains open by communicating with a radial retinal fold that extends posteriorly, beyond the buckle)
Post-operative complications
- Recurrent retinal detachment –most often due to a missed retinal break or PVR
- Ptosis resulting from levator muscle damage
- Anterior segment ischemia
- Refractive error
- Buckle infection
- Buckle intrusion / extrusion
- Strabismus
- Muscle imbalance
- Choroidal detachment
- Increased intraocular pressure
- Epimacular membrane
- Cystoid macular edema
- Scleral abscess / endophthalmitis
The outcome of surgeries: Scleral buckling results in attachment of the retina with asingle surgeryin 85-95% of treated eyes.9, 10The Most common cause of recurrence is a missed retina break, followed by PVR. Better pre-operative vision is associated with better post-surgical visual outcomes.
Advances in scleral buckling surgery:
Traditionally visualization of the retina in scleral buckling is performed using the indirect ophthalmoscope. Decreasing familiarity with indirect ophthalmoscopy and postural issues associated with its use during the scleral buckling surgery are some of the factors for the waning popularity of scleral buckling. Some authors suggest viewing the fundus using a wide-angle viewing system and chandelier illumination instead of the indirect ophthalmoscope. This approach allows better visualization of the fundus pathology utilizing the magnification capabilities of the operating microscope; postural issues associated with indirect ophthalmoscopy are also avoided. This technique, however, needs a more complex, expensive vitreoretinal set up comprising of the surgical microscope, wide-angle viewing system, chandelier light fiber and a light source.11,12
Recently suprachoroidal buckling using absorbable viscoelastic material has been described.13 In this technique, a specially designed illuminated catheter is passed in the suprachoroidal space via an anteriorly placed sclerotomy. This catheter, passed along the meridian of the retinal break is positioned beneath the break with the aid of its illuminated tip and a long-acting viscoelastic is injected. This suprachoroidally injected viscoelastic indents the overlying choroid towards the retinal break and seals it. In eyes with extensive SRF, it has to be drained to allow suprachoroidal injection. Retinopexy is performed with the laser indirect ophthalmoscope. The viscoelastic absorbs over time, thus making it a temporary buckle, by which time however, the break would have sealed permanently because of the retinopexy performed.
While it is an elegant procedure, it necessitates the use of the special illuminated catheter, a steep learning curve and is not without complications. Suprachoroidal hemorrhage, inadvertent perforation of the overlying choroid and retina are some of the reported complications.
Conclusions
Scleral buckling is an elegant surgery, however with unwarranted waning popularity. Decreasing familiarity with indirect ophthalmoscopy and postural issuesassociated with its use during the scleral buckling surgery(for the surgeon)are some of the factors for the waning popularity of scleral buckling.It is the preferred choice in treating uncomplicated rhegmatogenous retinal detachment in phakic patients, offering the same success rates as vitrectomy. It is also preferable in young patients as it does not increase the risk of cataract, as does a vitrectomy.
References
1. Gonin J. Treatment of detached retina by sealing the retinal tears. Arch Ophthalmol 1930;4:621. 2. Schepens CL, Okamura ID, Brockhurst RJ. The scleral buckling procedures I. Surgical techniques and management. Arch Ophthalmol 1957;58:797. 3. Lincoff HA, Baras I, McLean J. Modifications to the custodis procedure for retinal detachment. Arch Ophthalmol1965;73:160. 4. Scleral Buckling versus Primary Vitrectomy in Rhegmatogenous Retinal Detachment Study Group. Scleral buckling versus primary vitrectomy in rhegmatogenous retinal detachment: a prospective randomized multicenter clinical study. Ophthalmology. 2007 Dec;114(12):2142-54. 5. Stoffelns BM, Richard G. Is buckle surgery still the state of the art for retinal detachments due to retinal dialysis? J Pediatr Ophthalmol Strabismus. 2010 Sep-Oct;47(5):281-7. 6. Jesberg DO, Schepens CL. Retinal detachment associated with coloboma of the choroid. Arch Ophthalmol. 1961;65:163–173. 7. Ryan SJ, Goldberg MF. Anterior segment ischemia following scleral buckling in sickle cell hemoglobinopathy. Am J Ophthalmol. 1971 Jul 30;72(1):35-50. 8. Shanmugam PM, Singh TP, Ramanjulu R, Rodrigues G, Reddy S. Sutureless scleral buckle in the management of rhegmatogenous retinal detachment. Indian J Ophthalmol. 2015 Aug; 63(8): 645–648. 9. Häring G, Wiechens B. Long-term results after scleral buckling surgery in uncomplicated juvenile retinal detachment without proliferative vitreoretinopathy Retina. 1998;18(6):501-5. 10. Schwartz SG, Kuhl DP, McPherson AR, Holz ER, Mieler WF . Twenty-year follow-up for scleral buckling. Arch Ophthalmol. 2002 Mar;120(3):325-9. 11. Gogia V, Venkatesh P, Gupta S, Kakkar A, Garg S. Endoilluminator-assisted scleral buckling: our results. Indian J Ophthalmol. 2014 Aug; 62(8):893-4. 12. Aras C, Ucar D, Koytak A, Yetik H. Scleral buckling with a non-contact wide-angle viewing system. Ophthalmologica. 2012; 227(2):107-10. 13. En El Rayes et al. Suprachoroidal Buckling: Technique and IndicationsJ Ophthalmic Vis Res. 2013 Oct; 8(4): 393–399.