

Manual small incision cataract surgery (MSICS) is now practiced in both developed and developing countries. It involves the extraction of a complete or divided nucleus from the capsular bag through the capsular opening and then through the sclero-corneal tunnel.
A number of techniques of nuclear delivery have evolved over the time. These techniques have their own merits and demerits. However they give similar results in the hands of experienced surgeons. The methods are broadly classified as follows:
- Anterior chamber maintainer technique
- Microvectis technique
- Phacofracture technique
- Phacosandwich technique
- Fish hook technique
- Ruit's technique
We shall now discuss the difference in steps involved in the various techniques.
1.Anterior Chamber Maintainer technique ( Blumenthal`s technique):
Fixing the AC Maintainer (Anterior Chamber Maintainer)
After the tunnel has been dissected with a crescent knife, two side ports are made with 19 or 20 G MVR knife, one for capsulotomy and the other for fixing the AC maintainer. All this is done prior to entry with the keratome because once the entry is made, the intraocular pressure falls and it becomes difficult to insert the AC maintainer. Thus, after ensuring that AC is adequately deep with viscoelastics, MVR blade is entered at 5 o'clock or 7 o`clock position parallel to limbus, away from the vascular arcade of cornea in the left and right eye respectively.
The AC maintainer is a hollow steel tube with 0.9 mm outer diameter and 0.65 mm inner diameter. It is held firmly not too far away from its tip, with thumb and index finger and entered with bevel up in a screwing manner and then turned 180 degrees so that the bevel faces the iris. Prior to its insertion it is flushed with balanced salt solution (BSS) not only to check patency but also to remove any air column in the tubing.ACM is preferably inserted from the temporal side.The tube of ACM is attached to BSS bottle suspended 50-60 cm above the patient's eye.
While making an entry with MVR, care should be taken to create a tunnel-like opening of adequate size. The blade should be held in such a manner that the widest portion is parallel to the iris surface and not tilted. A narrow opening causes difficulty in insertion of ACM whereas a large opening results in repeated slipping of ACM thereby preventing adequate buildup of hydropressure for delivery of the nucleus. Also while inserting the steel tube it has to be held from the steel portion and not too far away. A smooth, controlled entry of ACM averts injury to iris or Descemet's membrane. Stromal edema may occur if part of the bevel remains in the stroma and allows seeping of fluid into the cornea. Corneal haziness makes further surgical maneuvers difficult. This can be avoided by ensuring that the bevel is completely in AC facing the iris. If the corneal hydration at site of ACM is developing, one should choose another site for ACM insertion.
Nucleus delivery by ACM
The principle of the technique is to
1. Engage the nucleus into the sclerocorneal pocket tunnel with help of lens glide or thin iris repositor.
2. Push the nucleus out by hydropressure.
3. Pull the nucleus out by a needle if so warranted.
For engaging the nucleus into the sclerocorneal pocket tunnel, after injecting viscoelastic both in front and behind the nucleus, a lens glide is passed behind the nucleus one-third or half the nucleus width distance. The lens glide should not be pushed inside forcibly as it can cause iridodialysis and even posterior capsular rupture. A thin iris repositor can serve the same purpose. Once the lens glide is in position, ACM is opened and slight pressure is applied on the lens glide on the scleral side. Intermittent pressure facilitates the exit of the nucleus out of the tunnel's mouth. (Figure 1) Subsequently, few more taps enable the epinucleus and cortex to flow out of the AC.
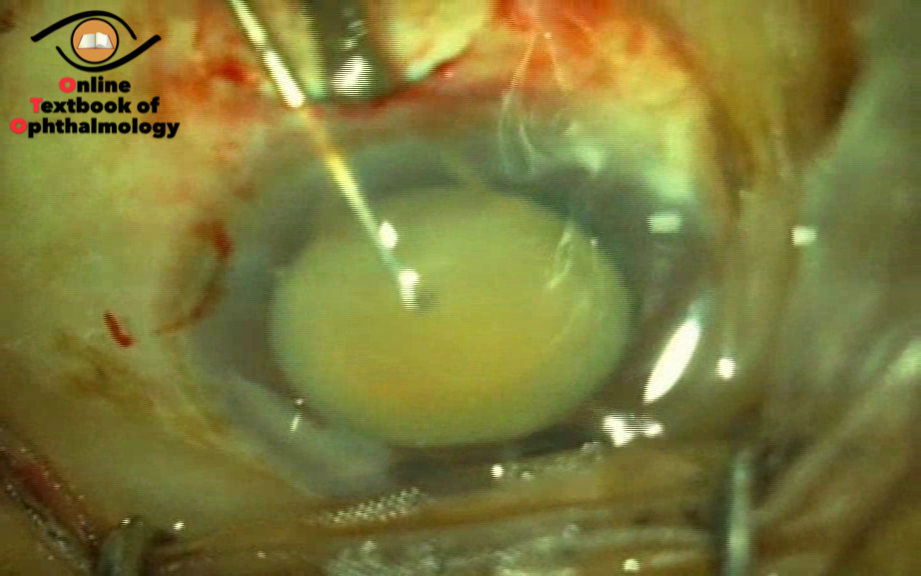
Figure 1 (click the image)
ASSISTED DELIVERY
If a portion of nucleus shows a bit out of the section but further progress is stalled even with full flow of ACM and lens glide or iris repositor in place, nuclear delivery can be assisted by 23 G needle held in the other hand. The nucleus is engaged at right angle to its axis with a 23 G needle, ACM generated hydropressure pushes the nucleus out. The needle assists by pulling it and the intermittent pressure on the lens glide or iris repositor guides the nucleus out.
The needle can also be used for debulking the nucleus by repeatedly engaging more and more of the extruded portion of the nucleus, chipping it off, pushing the remaining nucleus back into the AC, re engaging the smaller diameter and allowing it to flow out.
If the nucleus does not engage into the inner lip of the tunnel despite the full volume of ACM flow the reasons may be
- Small tunnel
- Irregular tunnel
- Incomplete dissection with some fibers still adhering
- AC leaking through irregularly created main opening or side port
- Premature entry in the AC with prolapsed iris obstructing the outlet
- Vitreous in AC.
Whenever such a situation arises, it is important to identify the cause. After injecting viscoelastics, tunnel may be revisited using 3.2 mm angled keratome to ensure that there is no disproportion between the inner lip of the tunnel and the size of the nucleus; If required, the side pockets may be enlarged because once the nucleus engages, the corneo scleral pockets will accommodate the large nucleus like a rat in the small mouth of a snake. Further built up of pressure within the AC will force a bit of nuclear portion out, which can be chipped off to make it smaller. It may be emphasized at this juncture that the tunnel dissected should not have multiple planes and uniform dissection should be ensured. Blunt knives should not be employed, as they not only have crushing effect on the tissues, but also the excessive force used can cause tissue dissection in undesired direction at times. This may lead to a leaking tunnel later or even total loss of integrity of the tunnel.
Adequate size of corneoscleral pocket tunnel and sufficient hydroprocedure usually delivers the nucleus. Once the nucleus is engaged and hypotony suspected, the bottle height may be increased. If the nucleus does not engage due to the hypotony, viscoelastic can be injected through the ACM to push the nucleus towards the section. Raising the bottle height before the nucleus is engaged does not help.
If the iris prolapses out, every time the ACM is on, it indicates premature entry near the root of the iris. Lens glide is more useful instead of iris repositor in this situation because the larger width of the lens glide pushes the iris back. If this does not help then section should be enlarged side ways with slit knife to prevent damage to iris and cornea.
2.NUCLEUS REMOVAL BY IRRIGATING WIRE VECTIS:
The irrigating wire vectis can be used to deliver the nucleus either by hydroexpression or by viscoexpression. Various sizes of vectis are available. The irrigating wire vectis which is used is 4 mm in width and 9 mm in length. It has two surfaces namely anterior and posterior. The anterior surface has a slight concavity with three 0.3 mm openings at one end. The other end continues as the main body of vectis to be attached to a syringe or infusion set.
Delivery by hydroexpression
The vectis is attached to infusion set. The nucleus is prolapsed into the AC, viscoelastic is injected both above and below the nucleus, the vectis is insinuated below the nucleus and the infusion is started. The flow through the vectis generates a hydropressure, the globe is stabilized by holding with a forceps at 6 o`clock position and the vectis is gradually withdrawn. Pressure on the posterior lip of the tunnel guides the nucleus out.(Figure 2)
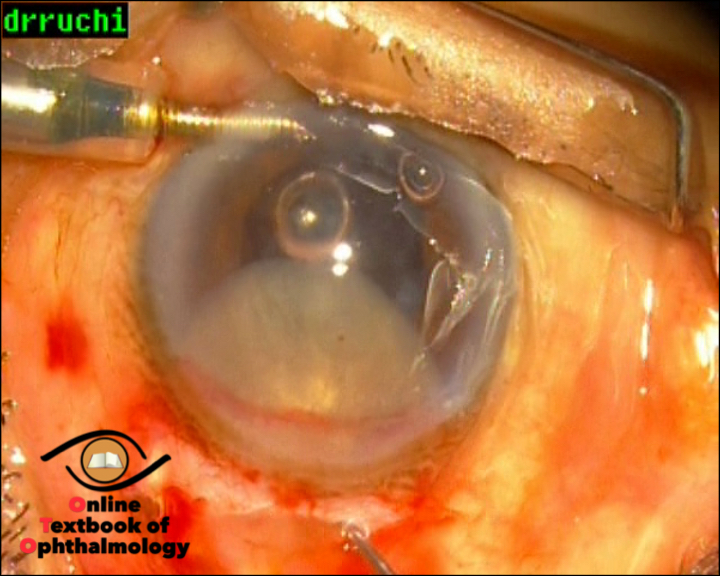
Figure 2 (click the image)
Alternatively, the vectis can be attached to a 5 ml syringe containing BSS. After immersing the nucleus in an ocean of viscoelastics, the superior rectus suture is held loosely in left hand. The vectis is positioned as earlier. The superior rectus is pulled tight and the globe thus fixed, the irrigating vectis is withdrawn slowly without irrigating till the superior pole of the nucleus is engaged in the tunnel. The irrigation is then started and the vectis slowly withdrawn while pressing down on the scleral lip. The force of irrigation has to be reduced when the maximum diameter of the nucleus just clears the tunnel. This step prevents the nucleus from being thrown out forcefully with consequent sudden decompression and shallowing.
DELIVERY BY VISCOEXPRESSION
Here the vectis is attached to a syringe carrying low molecular weight viscoelastics. Nuclear delivery is accomplished as before except that viscoelastics are used instead of BSS.
Advantages of Microvectis Technique
- Only a single instrument is used inside the anterior chamber
- Easy and faster delivery of nucleus.
- Especially useful in case of premature entry in the tunnel and superior zonular dehiscence
Disadvantages of Microvectis Technique
- Crushing of the inferior iris between the vectis and the nucleus if the vectis is not positioned properly.
- Endothelial damage if chamber is not kept sufficiently deep during nuclear delivery as insertion of vectis itself leads to some amount of shallowing of AC.
The pores on microvectis have a tendency to get blocked very fast so it is mandatory to check the patency before the vectis is insinuated.
3. PHACOFRACTURE:
The technique was initially described by Peter Kansas. He used two modified Kuglen instruments to prolapse the nucleus out of the bag. The superior pole is first engaged to tip the nucleus into the iris pupillary plane. The nucleus is then engaged with the second instrument and rotated so that it is loosened from its underlying attachments to the posterior cortex.
The anterior chamber is filled with viscoelastic. A solid curved vectis, is insinuated under the nucleus, the nucleotome is positioned on the anterior surface of nucleus and thetwoinstruments are maneuvered towards each other.
The nucleotome gradually cleaves its way through the nuclear substance and stops when it comes in contact with the vectis. Gentle lifting pressure with the vectis and steady pressure with the nucleotome splits the nucleus into two halves. The two halves are separated, viscoelastic is injected between the anterior surface of the nuclear fragments and the endothelium as well as the cleavage plane of the two fragments. The nuclear forceps, which has 9.0 mm long jaws (each having a double row of teeth) is introduced into the anterior chamber and the nuclear fragments are brought out one at a time.
Modification of Phacofracture
This technique involves use of Sinskey's hook instead of nucleotome and wire vectis instead of solid vectis.
A wire vectis which is 3 mm wide and 9 mm long is used. The wire vectis occupies lesser space and conforms to the shape of nucleus in comparison to the solid vectis. The anterior chamber is filled with viscoelastic and the nucleus is prolapsed out. Wire vectis is insinuated beneath the nucleus and the Sinskey's hook is placed diagonally on the anterior surface of nucleus. The two instruments are maneuvered towards each other and the nucleus is crushed into two halves. Sinskey's hook is brought out and wire vectis is left in place.(Figure 3) The two halves are separated after injecting viscoelastic. Each half is brought out sandwiching it between the vectis and the viscoelastic cannula, viscoelastic being injected as the nuclear piece is brought out.
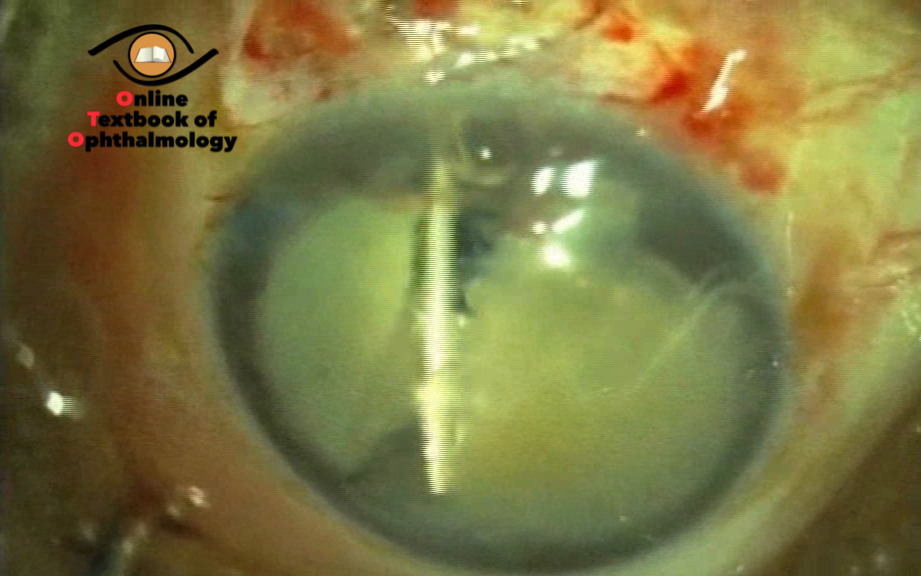
Figure 3 (click the image)
MANUAL MULTIPHACOFRAGMENTATION
This has been described by Francisco J Gutierrez - Carmona. In this technique the nucleus is fragmented into multiple tiny pieces of 2x2 mm. It can be performed through 3.2 mm clear corneal or 3.5 mm scleral tunnel incisions. He uses a racquet shaped-nucleotome 8 mm long and 2 mm wide, divided along its short axis by three thin transverse bars 2 mm apart, set at 45 degrees to a long straight handle, two straight handled manipulators, right and left, used to collect nuclear fragments. Once the nucleus has been prolapsed into the AC, high density viscoelastic is injected into the surrounding area to fill the AC. The spatula is placed beneath and the nucleotome on the top of the nucleus. The two instruments are pressed against each other and the nucleus is fragmented into four pieces which remain within the nucleotome. The fragments of the nucleus are extracted from AC using a sandwich technique. The right and left manipulators are used to displace the remaining fragments of nucleus to the center of AC for further fragmentation and extraction. A conscious effort is made to keep the AC deep by injecting viscoelastics as and when required.
PHACOFRACTURE—OTHER TECHNIQUES
1. Bisector technique.
2. Trisector technique.
3. Wire loop technique.
4. Phacosalute and fracture.
5. Phacofracture at the exit.
Limitation of Phacofracture
- It is difficult to break grade V nuclei, so is better to use techniques in which nucleus is removed piecemeal in such cases to avoid damage to the endothelium caused by excessive manipulation of instrument in the anterior chamber.
- Since two instruments have to be manipulated inside the anterior chamber, the chances of endothelial damage are more therefore copious use of viscoelastic is advisable. In phacosalute there are even greater chances of injury to the cornea.
Advantages of Phacofracture
1. Side pocket dissection is not required therefore there is lesser distortion of cornea. This conforms to the square geometry and produces lesser astigmatism.
2. Requires a smaller wound size.
4.PHACOSANDWICH TECHNIQUE:
This technique was introduced by Luther L Fry with a standard 10-11 mm incision which was gradually reduced to 7.5 mm. He proposed 7.5 mm opening for most of the nuclei.
Further modifications in the procedure allow an external incision size of 6.5 mm. Nucleus is prolapsed into the AC and brought out by sandwiching it between a dialer and vectis.(.Figure 4)

Figure 4 (click the image)
ADVANTAGES
1. Easy to deliver the nucleus even if there is hypotony.
2. Nuclear delivery can be easily performed even if the integrity of the tunnel is compromised.
DISADVANTAGES
1. Requires a larger incision size.
2. Increased chances of endothelial damage as two instruments have to be inserted in the anterior chamber.
5. FISH HOOK TECHNIQUE
This method was popularized by A. Henning. After filling the chamber with viscoelastics, only the superior pole of nucleus is brought into the anterior chamber. Viscoelastic is injected both in front and behind the nucleus The tip of 30 G needle is bent in the form of hook. It is entered into the AC with a sidewards tilt and then rotated so as to prevent endothelial injury. It is then maneuvered behind the nucleus to hook the undersurface of the nucleus. Viscoelastic may be reinjected behind the nucleus if there is difficulty in traversing the fish-hook. Once the nucleus is hooked, it is slided out with slight pressure by the fish-hook on the posterior lip of the tunnel. The nucleus is thus delivered without performing extensive maneuvers in the AC.(Figure 5)
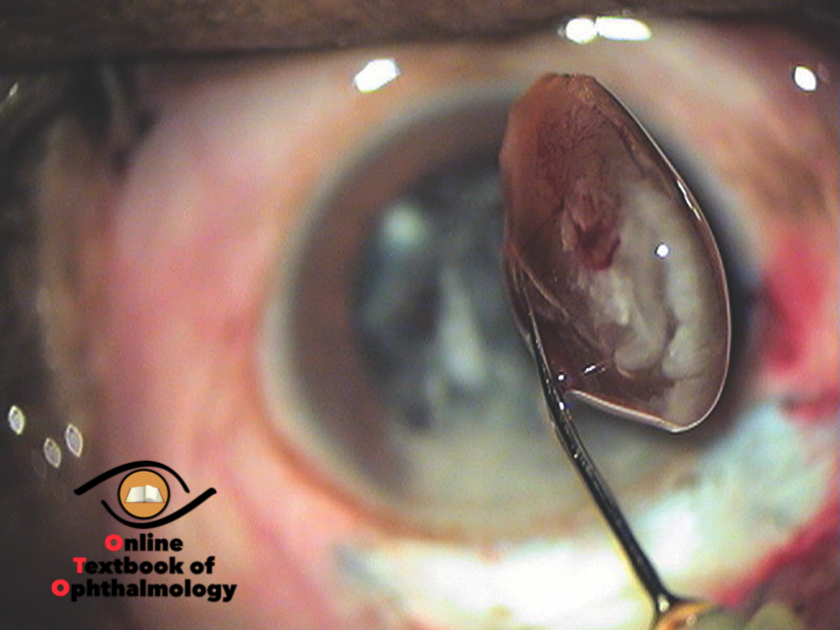
Figure 5 (click the image)
RUIT TECHNIQUE
A 6.5- to 7-mm temporal scleral tunnel is created. Viscoelastic is injected around the nucleus, and the nucleus is dislocated into the anterior chamber. An irrigating Simcoe cannula is inserted below the nucleus, and the nucleus is extracted through the scleral tunnel.
CONCLUSION
Various techniques of nuclear delivery are practiced by different surgeons while performing SICS. The entire nucleus is prolapsed out of the bag except in phacosandwich (Luther Fry) and Fish hook techniques, where only the superior pole is prolapsed out first.
The external incision size varies mostly from 5.5 to 6.5 mm. The exceptions being a larger section as described by Luther Fry (Phacosandwich), in a very large hard brown/black nucleus or in case of zonular dehicense. Smaller section is required in phacofragmentation. The advantage of modified Blumenthal technique is minimum instrumentation inside the chamber unlike phacosandwich and phacofragmentation. Microvectis is easier to perform than Blumenthal technique in case the tunnel construction is poor or the lens is subluxated but the demerit is that instrument manipulation is more than with the iris repositor or lens glide as employed in Blumenthal's technique. There are no studies to prove superiority of one technique over other.