

Introduction:
Syphilis is considered as a great mimicker due to its varied protean manifestations. It was first recognized in Europe in the late 15th century.[1] There have been several hypotheses regarding the origin and spread of syphilis and it is believed that the disease was brought back from the New World by the crew of Christopher Columbus, some of whom likely had syphilis on returning to Spain.
Since the advent of Penicillin in the mid-20th century, the incidence of syphilis has reduced however it still represents a larger global problem [2] and an estimated 12 million new cases of syphilis are added every year worldwide and more than 90% are from developing countries.[3] The risk is particularly higher in men who have sex with men (MSM) and socially marginalized groups and those with HIV Co-infection.[4]
The 2015 statistics from The Center for disease control and prevention (CDC) reported a 7.5 per 100,000 population of primary and secondary syphilis. (4). There has been a recent resurgence in cases of syphilis in the last few years. (5) In 2018, the total case count of reported syphilis was the highest recorded since 1991. The total number of reported cases of syphilis (all stages) increased by 13.3% during 2017–2018 (from 101,584 cases to 115,045 cases).(2) The risk is particularly higher in men who have sex with men (MSM) and socially marginalized groups and those with HIV Co-infection.[4]
Natural history/Course of infection:
Syphilis is caused by a spirochete Treponema pallidum, which can affect the skin, heart, blood vessels, central nervous system, bones, and eyes. T. pallidum disseminates within days after infection, resulting in the early invasion of distant tissues, including the central nervous system (CNS).
Modes of transmission
Syphilis is predominantly transmitted sexually, including oral and anal sex, via skin to skin or mucocutaneous contact during the primary and secondary stages. An increased risk of syphilis transmission occurs in mem having sex with men.
Congenital syphilis has increased 2-fold in the US between 2012 and 2016. Transmission occurs transplacentally at any time during pregnancy, and with very high rates of transmission and sequelae during untreated primary and secondary syphilis. Rare modes of syphilis transmission include blood transfusion, organ transplants and even through shared needles
Clinical Features
Clinical manifestations of Syphilis are divided into 3 stages.
A. Primary Syphilis
The primary stage of syphilis may be manifested clinically as a solitary painless chancre, indurated and ulcerative, with a clean base at genital or extragenital organs occurring 2–3 weeks after the agent’s exposure.[6]
Primary lesions heal without any sequela within 3 to 6 weeks.
B. Secondary Syphilis
Secondary syphilis may manifest as a rash on the palms and soles, fever, lymphadenopathy, mucosal lesions (condyloma latum).[7] If secondary syphilis remains untreated, it enters a further stage known as ‘‘latent.’’ This stage is subtle since no typical signs are present and the only serological tests may reveal the infection.[8] Latent syphilis is divided further into early and late latent stages, which have a significant meaning for therapeutic decision making. After several years, one-third of the untreated population develop further organs involvement, such as late neurosyphilis which presents generalized paresis or tabes dorsalis, cardiovascular involvement, and gummatous syphilis.
C.Tertiary Syphilis
Tertiary syphilis (i.e., late) predominantly affects the central nervous system and its neurologic manifestations are either meningovascular or parenchymatous.[9] Meningovascular syphilis usually occurs 5 to 12 years after initial infection but can occur earlier or later; manifestations may include hemiplegia, aphasia, and seizures. The vessels of the spinal cord may also be involved, resulting in meningomyelitis and spinal vascular syphilis. The parenchymatous forms, general paresis, and tabes dorsalis tend to occur later (>15 years after infection).[7]
Ocular syphilis and otic syphilis are distinct entities from neurosyphilis but may occur concomitantly. Ocular manifestations of syphilis can happen mostly in secondary and tertiary stages of syphilis, even though ocular involvement can occur in all stages.[10] Manifestations of ocular syphilis are diverse and patients may complain of eye pain, vision loss, floaters, and photophobia.
Ocular manifestations of Syphilis:
Ocular syphilis has varied manifestations and there has been a re-emergence in the current era in patients with HIV with/without HAART. Ocular manifestations occur in about 0.6-2% of all patients with syphilis at any stage of the disease. (6)
Conjunctiva:Syphilitic conjunctivitis is characterized by marked congestion and chemosis in the skin and mucous membranes. Chancres and conjunctival involvement secondary to gummatous tarsitis, have been known to occur as well.[11] Conjunctival biopsies in addition to serological tests may be useful in establishing the diagnosis of ocular syphilis.[11]
Cornea:Interstitial keratitis is a rare manifestation of ocular syphilis in the post-antibiotic era. The postulated pathophysiology behind this clinical entity is an immunologic phenomenon directed against treponemal antigens deposited in the cornea. Syphilitic interstitial keratitis usually presents in late childhood or early adulthood, and rarely after 40 years of age. It is classically bilateral and patients complain of watering and photophobia. It is to note that, syphilitic interstitial keratitis usually does not respond to penicillin alone and will also need steroids which have been shown to result in clinical improvement.[12]
Uveal tract: Ocular syphilis predominantly affects the uveal tract and it can manifest as non-specific anterior uveitis, intermediate uveitis, posterior uveitis, and panuveitis.[13] In a study of 24 patients by Barile and Flynn, the most common manifestations of inflammation secondary to syphilis were found to be granulomatous iridocyclitis (46%), followed by non-granulomatous iridocyclitis (25%), panuveitis (13%), posterior uveitis(8%), and keratouveitis (8%).[14] However, in a series of acute anterior uveitis in Sydney, recorded only two cases of syphilitic uveitis among 241 patients (0.8%). [15]
Retina and choroid:Posterior uveitis represents the most typical clinical presentation, even though syphilis may present variable forms of presentation. Syphilis is widely referred to as ‘‘the great imitator’’ since its posterior segment manifestation can mimic those of other ocular conditions, making the diagnosis challenging. The most frequent posterior segment manifestation of syphilis is retinochoroiditis in confluent or in the placoid form. [16] The posterior pole involvement is the main clinical finding, leading to different clinical findings such as neuroretinitis, retinochoroiditis, chorioretinitis, as well as retinal necrosis with a central clearing.[17] Multimodal imaging helps in differentiating these great mimickers.[18] In a case series consisting of syphilitic posterior uveitis, three-fourths of them presented with chorioretinitis.[16] Gass described a characteristic large, placoid, circular or oval, a yellowish lesion with faded centers at the level of pigment epithelium in the macular and juxtapapillary area, in six patients with systemic syphilis infection and labelled it as “acute syphilitic posterior placoid chorioretinitis” (ASPPC) Sometimes Syphilitic chorioretinitis can present as choroidal graunolma with associated subvascular pigmentation mimicking tubercular choroiditis.[19] Recently Pathengay et al., described that retinal miliary lesions seem to involve full thickness of the retina on OCT and may heal with pigmentation and they considered these lesions may be characteristic of ocular syphilis.[20]Superficial retinal precipitates in ocular syphilis have been described previously in the literature. It has been noted in previous studies that on OCT, these lesions were superficial and adherent to the retina, with authors hypothesizing that they consisted of white cell aggregates and are formed due to an exaggerated ocular response to syphilis infection with concurrent administration of HAART therapy Others hypothesized that these may be a collection of treponemal bacteria and a collection of exudates on the retina. We had recently described full-thickness miliary lesions which seem to involve full thickness of the retina on OCT and may heal with pigmentation as characteristic of ocular syphilis.[20]
Optic nerve:
Optic disc involvement in ocular syphilis includes neuroretinitis, gumma of the optic disc,[21] disc edema,[22] perineuritis, anterior or retrobulbar optic neuritis, and papilloedema [23] Syphilitic optic perineuritis is usually asymptomatic, while optic neuritis is characterized by rapid vision loss. Examination of pupils for light near dissociation and Argyll Robertson pupil is essential as it is a classical finding in neurosyphilis. Examination of the cerebrospinal fluid (CSF) is essential in patients with syphilitic nerve involvement to confirm the diagnosis of neurosyphilis and also in all cases of unexplained visual loss for subclinical optic nerve involvement.
|
Ocular structure |
Type of lesion/involvement |
|
Eyelid |
Chancre, Gumma, Tarsitis, Ulcerative blepharitis |
|
Conjunctiva |
Chancre, Conjunctivitis, Tarsitis |
|
Orbit |
Periostitis, Gumma (extraocular muscle, lacrimal gland or within orbit) |
|
Cornea |
Interstitial keratitis, Ulcers, Deep punctate keratitis |
|
Sclera, Episclera |
Scleritis, Episcleritis, Gumma |
|
Iris and ciliary body |
Roseolae, Papules, Gumma |
|
Pupil |
Argyll Robertson Pupil |
|
Lens |
Capsular rupture, Cataract, Traumatic dislocation |
|
Glaucoma |
Secondary glaucoma |
|
Optic nerve |
Papillitis, Perineuritis, Anterior optic neuritis, Retrobulbar neuritis, Neuroretinitis, Papilloedema, Optic atrophy |
|
Motility dysfunctions |
Oculomotor, abducens, trochlear associated paresis, Periodic alternating nystagmus |
|
Retina, vitreous |
Preretinal precipitates,Vitiritis, Choroidal granulomas, Chorioretinitis, Necrotizing retinitis, Retinal vasculitis, Central retinal artery/vein occlusion, Exudative retinal detachment, Placoid chorioretinitis |
|
Uveal tract |
Anterior uveitis, Intermediate uveitis, posterior uveitis Panuveitis |
Table 1: Ocular manifestations of Syphilis
|
Clinical Feature |
Fundus appearance patterns |
Autofluorescence |
OCT |
Pattern of Healing |
|
Full-thickness retinitis |
Full thickness, Wedge shaped, ground glass appearance, |
Hypoautofluorescent |
Hyperreflective dots in vitreous, inner and outer retinal cysts, loss of differentiation of inner retina and ELM, irregular elevations of RPE |
Pigmented scarring |
|
Placoid chorioretinitis |
Granular outer retinal placoid lesion |
Diffuse hyper autofluorescence involving the posterior pole and the arcades along the margins of the lesion with scattered stippled hypo autofluorescence |
Edematous inner retinal layers, ILM folds, loss of EZ, inflammatory subretinal deposits / lesions, Intra retinal hyper reflective dots and dipping down of inner retinal layers specifically IPL and GCL into INL, thinned RPE |
Resolve without pigmentation |
|
Miliary Retinal Lesions |
Full thickness lesions associated with ground glass retinitis and retinal vasculitis |
Hypoautofluorescent lesion with minimal perilesional hyper autofluorescence |
Involving entire thickness of retina as a hyperreflective small focus |
Resolve with pigmentation and scarring |
|
Choroidal Granuloma/Multifocal Choroiditis |
Elevated choroidal granuloma with full thickness retinitis, overlying tortuous vessels, multiple subvascular chorioretinal scars, disc edema, peripheral small active choroiditis lesions at the margins |
Uniform hyper autofluorescence corresponding to the choroidal elevation, hypoautofluorescent scars |
Elevated choroidal lesion with full thickness retinal involvement, focal vitreous attachment, surrounding NSD, CME with intra retinal hyper-reflective dots at the macula |
Resolution of granuloma with pigmented scarring, straightening of overlying vessels |
Table 2: Imaging characteristics of Retinitis lesions in ocular syphilis
OCT – optical coherence tomography, ELM – external limiting membrane, RPE – retinal pigment epithelium, ILM – internal limiting membrane, EZ – ellipsoid zone, IPL – inner plexiform layer, GCL – ganglion cell layer, INL – inner nuclear layer
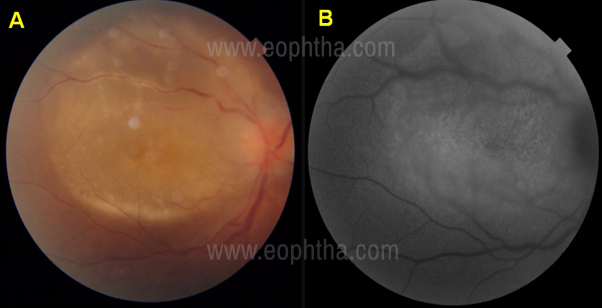
outer retinal placoid lesion, with the autofluorescence image
(1B) showing speckled hyperautofluorescent dots corresponding to the lesion and within the lesion, interspersed with pin point hypoautofluorescent dots
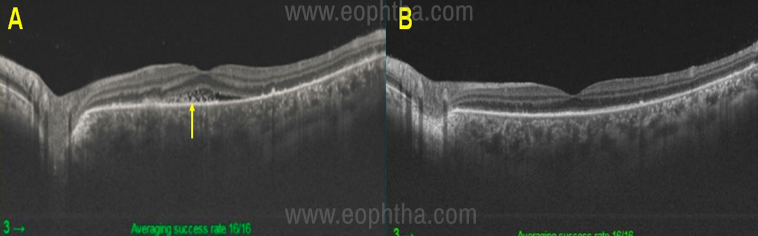
scans at initial presentation through the lesion of
placoid outer retinitis showing areas ofirregularity or loss of
ellipsoid zone, areas of thinned and thickened retinal
pigment epithelium (RPE), inflammatory subretinal and
subRPE deposits and intra retinal hyper reflective dots
Figure 2B After treatment showing resolution
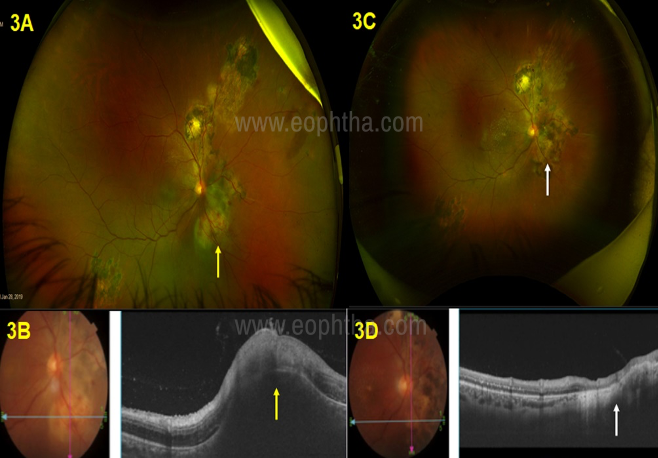
elevated lesion inferio-nasal to optic disc (yellow arrow)
Figure 3B OCT showing elevated choroidal granuloma
with overlying retinitis (yellow arrow)
Figure 3C,3D After treatment with IV pencillin
for 2 weeks showing complete resolution
of chorioretinitis and choroidal granuloma
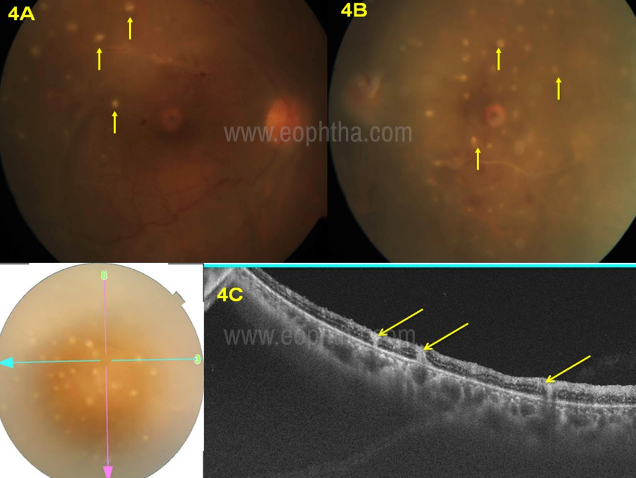
showing multiple military retinal lesions (yellow arrow),
retinal vasculitis Figure 4C OCT passing through the miliary
retinal lesions showing full thickness involvement

ground glass retinitis with military lesions and
central clearing of retinitis lesion (yellow arrow)
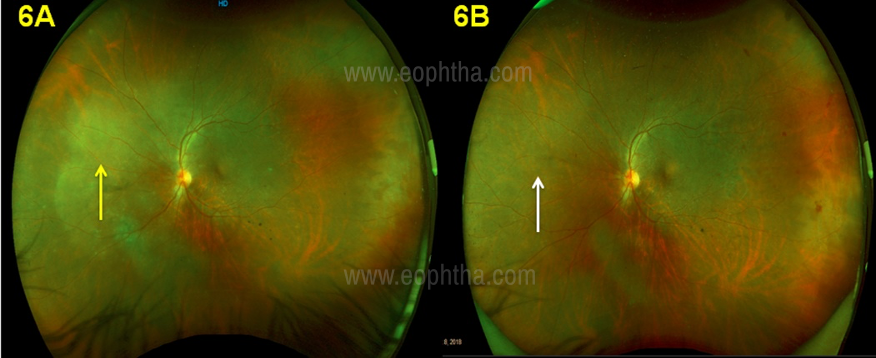
showing ground glass retinitis (yellow arrow) and Figure 6A after
treatment showing complete resolution of retinitis lesion (white arrow)

Investigations:
Direct detection methods:
Direct detection methods such as dark-field microscopy, polymerase chain reaction (PCR) and immunohistochemistry provide direct evidence of syphilitic infections, thus giving a definitive diagnosis of syphilis. Dark-field microscopy directly visualizes T. pallidum by examining the exudates from chancres, condyloma lata, lymph node aspirates using a compound microscope with a darkfield condenser.[25] The sensitivity and specificity of dark-field microscopy in the diagnosis of syphilis is approximately 90%and 100%respectively.[26]
Serological tests:
Serological tests can be divided into two groups: the non-treponemal tests, which detect non-specific treponemal antibodies, and the treponemal tests, which detect specific treponemal antibodies. Examples of treponemal tests are T. pallidum Hemagglutination Assay (TPHA), T. pallidum Passive Particle Agglutination test (TPPA) and Fluorescent Treponemal Antibody-absorption (FTA-abs). Non-treponemal tests include Venereal Diseases Research Laboratory test (VDRL) and Rapid Plasma Reagin test (RPR).
Spirochetes are believed to secrete cardiolipin,[27] and thus non-specific antibodies which react to cardiolipin are produced in syphilitic infections. This forms the basis of the non-treponemal tests,[25] which use a cardiolipin- lecithin-cholesterol antigen, and using antigenantibody interactions, measure the titers of IgG and IgM antibodies formed. Thus, they are usually used as screening tests for syphilis. In addition, since antibody titers correlate with disease activity, they can also be used to monitor disease activity and treatment efficacy.
Treponemal tests use recombinant treponemal antigens. Titers of IgG and IgM remain positive for life, thus, unlike non-treponemal tests, treponemal tests cannot be used to assess disease activity and treatment efficacy. Instead, treponemal tests are used as confirmatory tests for the diagnosis of syphilis when nontreponemal tests are positive due to their high specificity and lower incidence of false positivity.[13, 24,25,28,29] .Studies have also shown that treponemal tests like TPHA have a sensitivity and specificity of more than 90 percent for tertiary syphilis.
Nontreponemal tests are used to monitor the disease and detect reinfection. (19) Seroconversion with non-treponemal tests may take up to 3-6 weeks. Poor sensitivity (70%) in primary and late syphilis, false-positive tests due to cross-reactivity with other antigens, and false negativity due to the prozone phenomenon are the main limitations of non-treponemal tests like VDRL.
Testing for syphilis has been proposed in two main algorithms. The traditional algorithm involves screening with a nontreponemal test (VDRL or RPR), with reactive samples being confirmed now where initially screening of patients is done with a treponemal test. Positive tests of untreated or treated syphilis are then confirmed with nontreponemal assays (VDRL and RPR).
Cerebrospinal fluid antibody analysis:
Cerebrospinal fluid (CSF) analysis is indicated to assess CNS involvement in patients with ocular syphilis, as well as in those with other clinical signs of neurosyphilis, including cranial nerve dysfunction, auditory changes, acute/chronic altered mental status, loss of vibration sense, meningismus or evidence of stroke.
CSF analysis is indicated six months after the treatment of neurosyphilis, as persistent pleocytosis and/or reactive CSF-VDRL may be indicative of retreatment.
Definition of Cure:
A four-fold reduction of VDRL titer after 3 months indicates a good response to treatment. Nontreponemal test antibody titers might correlate with disease activity and are used to follow treatment response. Results however need to be reported quantitatively. A fourfold change in titer, equivalent to a change of two dilutions (e.g., from 1:16 to 1:4 or from 1:8 to 1:32), is considered necessary to demonstrate a clinically significant difference between two nontreponemal test results obtained using the same serologic test.
Hoogewoud et al defined improvement as a 2-step decrease of both anterior chamber and vitreous haze inflammation levels and also by the reduction in chorioretinal lesions. Recovery was defined as the resolution of inflammation in all anatomic structures at 1 month [30]
Treatment:
The discovery of Penicillin by Dr. Alexander Fleming in 1928 and their subsequent widespread use ushered in the modern antibiotic era. Since then, parenteral penicillins have been the mainstay of therapy for all stages of ocular syphilis.[31]
Penicillins are a group of beta-lactam antibiotics that act by inhibiting the peptidoglycancross-linking in the bacterialcell wall, thereby inhibiting the synthesis of the bacterial cell wall.
According to the CDC guidelines, a single intramuscular (IM) administration of 2.4 million units (MU) of benzathine penicillin G has been recommended for the treatment of primary, secondary, and early latent syphilis and a total of 7.2 MU of benzathine penicillian G, administered as three IM doses of 2.4 MU each at one-week intervals is recommended for the treatment of latent syphilis of unknown duration, late latent syphilis, and tertiary syphilis without evidence of neurosyphilis [32]
Syphilitic uveitis is considered equivalent to neurosyphilis and therefore its treatment has been defined according to the treatment and other recommendations for neurosyphilis. Currently, aqueous crystalline penicillin G 18–24 million units per day, administered as 3–4 million units IV every 4 hours or continuous infusion, for 10–14 days is the treatment of choice[32]
Alternatively, neurosyphilis can be treated with 2.4 MU of IM procaine penicillin once daily and probenecid 500 milligrams four times a day, both for 10 to 14 days.[32] CSF evaluation should be repeated every 6 months.While there have been instances of the use of antibiotics like amoxicillin, azithromycin, doxycycline and ceftriaxone for ocular syphilis, the evidence for their use has been relatively scarce as compared to penicillin
Ceftriaxone:
In the late 1980s, ceftriaxone was proposed as an alternative to penicillin being anecdotally used even for the treatment of neurosyphilis.[33,34] Successful treatment of patients with ceftriaxone 1-2 g intramuscular (IM) daily for 14 days has been reported [33-36]
Sood et al have also reported the successful use of 2.25 mg/0.1 ml of intravitreal ceftazidime for a penicillin-allergic case .Improvement in the retinitis lesions was noted within 1 day of intravitreal antibiotic therapy. The patient was also treated with concurrent intravenous (IV) Ceftriaxone 2 grams daily for 3 days while undergoing penicillin desensitization and subsequently with 24 MU of intravenous aqueous crystalline penicillin G for 14 days by continuous infusion.[36]
Doxycycline:
Doxycycline, a tetracycline derivative also has spirochaetocidal activity. A daily dose of 200 mg (in two equal doses), given orally, is effective in early and late syphilis.
Amode et al demonstrated the use of oral doxycycline at 200 mg/day, divided into two equal doses, for 28 days in a patient with syphilitic uveitis.[37]
B.Corticosteroids:
Topical and systemic corticosteroids have an adjunctive role in the management of ocular syphilis. Topical corticosteroids are effective in the management of interstitial keratitis and anterior uveitis
The use of systemic corticosteroids has been described as an adjunct r posterior uveitis, vitritis, scleritis, and optic neuritis and also to address the problem of Jarisch–Herxheimer reaction resulting from a hypersensitivity reaction to treponemal antigens that are released in large numbers because of the destruction of spirochaetes.However, the use of periocular dexamethasone injections and methylprednisolone pulses was significantly correlated to treatment failure.[30]
We believe that caution needs to be exercised before using periocular or intraocular steroids since these are known to reduce ocular immune responses and have been known to activate dormant infections and also lead to the development of viral retinitis and even toxoplasmosis
Conclusion:
Ocular Syphilis can have myriad presentations and it is important to keep it as a differential diagnosis in all cases of uveitis. Testing with treponemal and non-treponemal tests at the first visit itself is of utmost importance, as non-treponemal tests like VDRL may be frequently non-reactive and treponemal tests are more reliable in diagnosing ocular syphilis. Syphilitic uveitis is considered equivalent to neurosyphilis and therefore its treatment has been defined according to the treatment and other recommendations for neurosyphilis
Points to remember:
- All HIV patients need to be screened for Syphilis
- Treponemal tests have high specificity for Ocular Syphilis and should be used for diagnosing Ocular Syphilis
- Partners of patients diagnosed as syphilis need to be screened and may need treatment
- Ocular Syphilis needs to be treated on lines of neurosyphilis
- Currently, aqueous crystalline penicillin G 18–24 million units per day, administered as 3–4 million units IV every 4 hours or continuous infusion, for 10–14 days is the treatment of choice
References:
- Harper KN, Zuckerman MK, Harper ML, Kingston JD, Armelagos GJ. The origin and antiquity of syphilis revisited: an appraisal of Old World pre-Columbian evidence for treponemal infection. Am J Phys Anthropol 2011; 146: Suppl 53: 99-133.
- Primary and secondary syphilis--United States, 2003-2004. MMWR Morb Mortal Wkly Rep 2006;55:269-73
- Hook EW, Peeling RW. Syphilis control: a continuing challenge. N Engl J Med. 2004;351(2):122–124.
- Sexually transmitted disease surveillance 2018. Atlanta: Centers for Disease Control and Prevention, 2019.
- Fonollosa A, Giralt J, Pelegrín L, et al. Ocular syphilis—back again: understanding recent increases in the incidence of ocular syphilitic disease. Ocul Immunol Inflamm. 2009;17 (3):207–212.
- Sparling PF, Swartz MN, Musher DM,Healy BP. Clinical manifestations of syphilis. In: Holmes KK, Sparling PF, Stamm WE, et al., eds. Sexually transmitted diseases. 4th ed. New York: McGraw- Hill; 2008: 661-84.
- Ghanem KG, Ram S, Rice PA. The Modern Epidemic of Syphilis. N Engl J Med. 2020;382(9):845-854.
- Anderson J, Mindel A, Tovey SJ, Williams P (1989) Primary and secondary syphilis, 20 years’ experience. 3: diagnosis, treatment, and follow up. Genitourin Med 65(4):239–243.
- Merritt HH, Adams RD, Solomon HC. Neurosyphilis. New York: Oxford University Press, 1946.
- Kiss S, Damico FM, Young LH. Ocular manifestations and treatment of syphilis. Semin Ophthalmol. 2005;20(3):161-167.
- Spektor FE, Eagle RC, Nichols CW. Granulomatous conjunctivitis secondary to Treponema pallidum. Ophthalmology. 1981;88(8):863–865.
- Orsoni JG, Zavota L, Manzotti F, Gonzales S. Syphilitic interstitial keratitis: treatment with immunosuppressive drug combination therapy. Cornea. 2004;23(5):530–532
- Davis JL. Ocular syphilis. Curr Opin Ophthalmol. 2014;25(6):513-518
- Barile GR, Flynn TE. Syphilis exposure in patients with uveitis. Ophthalmology 1997; 104(10):1605–9.
- Karaconji T, Maconochie Z, McCluskey P. Acute anterior uveitis in Sydney. Ocul Immunol Inflamm 2013; 21:108–114.
- Samson CM, Foster CS (2001) Syphilis. In: Foster CS, Vitale AT (eds) Diagnosis and treatment of uveitis. WB Saunders, Philadelphia, pp 237–243
- Gass JD, Braunstein RA, Chenoweth RG (1990) Acute syphilitic posterior placoid chorioretinitis. Ophthalmology 97:1288–1297
- Pichi F, Neri P. Multimodal imaging patterns of posterior syphilitic uveitis: a review of the literature, laboratory evaluation and treatment. Int Ophthalmol. 2020;40(5):1319-1329
- Dogra A, Tyagi M, Kaza H, Pathengay A. Syphilitic chorioretinitis presenting as a choroidal granuloma. BMJ Case Rep. 2020;13(4):e234022
- Pathengay A, Kaza H, Tyagi M, Patel A, Pappuru RR, Agrawal H. Miliary Retinal Lesions in Ocular Syphilis: Imaging Characteristics and Outcomes Ocul Immunol Inflamm. 2019;1-5.
- Lee SY, Cheng V, Rodger D, Rao N. Clinical and laboratory characteristics of ocular syphilis: a new face in the era of HIV co-infection. J Ophthalmic Inflamm Infect. 2015;5(1):56.
- Browning DJD. Posterior segment manifestations of active ocular syphilis, their response to a neurosyphilis regimen of penicillin therapy, and the influence of human immunodeficiency virus status on response. Ophthalmology. 2000;107 (11):2015–2023.
- Smith GT. Neurosyphilis with optic neuritis: an update. Postgrad Med J. 2006;82(963):36–39.
- Dutta Majumder P, Chen EJ, Shah J, et al. Ocular Syphilis: An Update. Ocul Immunol Inflamm. 2019;27(1):117-125
- Majumder PD, Sudharshan S, Biswas J. Laboratory support in the diagnosis of uveitis. Indian J Ophthalmol. 2013;61 (6):269–276.
- Tsang RS, Morshed M, Chernesky MA, Jayaraman GC, Kadkhoda K. Canadian public health laboratory network laboratory guidelines for the use of direct tests to detect syphilis in Canada. Can J Infect Dis Med Microbiol. 2015;26 (Suppl A):13A–7A.
- Morshed MG. Current trend on syphilis diagnosis: issues and challenges. Adv Exp Med Biol. 2014;808:51–64.
- Centers for Disease Control and Prevention. Discordant results from reverse sequence syphilis screening- Five laboratories, United States, 2006-2010. MMWR Morbid Mortal Wkly Rep. 2011;60:133–137.
- Centers for Disease Control and Prevention. Syphilis testing algorithms using treponemal tests for initial screening- Four laboratories, New York City, 2005-2006. MMWR Morbid Mortal Wkly Rep. 2008;57:872–875.
- Hoogewoud F, Frumholtz L, Loubet P, Charlier C, et al. Prognostic Factors in Syphilitic Uveitis. Ophthalmology. 2017 Dec;124(12):1808-1816.
- Mauro J, Samson CM, Foster CS. Syphilis. In: Foster CS, Vitale AT, eds. Diagnosis and Treatment of Uveitis. New Delhi, India: Jaypee Brothers Medical Publishers; 2013:337
- Workowski KA, Bolan GA, Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64:1-137
- Fernanda A. Agostini MD, Rafael P. Queiroz MD, Danuza O. M. Azevedo MD, PhD, et al: Intravenous Ceftriaxone for Syphilitic Uveitis, Ocular Immunology and Inflammation, DOI: 10.1080/09273948.2017.131192
- Hook EW III, Roddy RE, Handsfield HH. Ceftriaxone therapy for incubating and early syphilis. J Infect Dis. 1988;158:881–884.
- Gentile JH, Viviani C, Sparo MD, et al. Syphilitic meningo- myelitis treated with ceftriaxone: case report. Clin Infect Dis. 1998;26:528
- Sood AB, Pearce WA, Workowski KA, Lockwood J, Yeh S. Combined Intravitreal and Systemic Antibiotic Therapy in a Patient with Syphilitic Uveitis. Ocul Immunol Inflamm. 2017 Oct 20:1-3
- Amode R, Makhloufi S, Calin R, Caumes E. Oral doxycycline for syphilitic uveitis: a case report highlighting potential efficacy. J Antimicrob Chemother.2018 Mar 23.