


Introduction
Surgical videos are an invaluable medium for surgical education. They allow not only for objective assessment & informative audits but also permit introspective critical analyses of surgical techniques. One may be doing a fantabulous job in his / her operating room but shall never be able to share his/her experience and skill unless the surgical video is recorded in good quality. One of the biggest challenges faced by ophthalmologists is the steep rise in the price of medical equipment. A good quality medical grade HD recording system set up (3 chip CCD camera + C-mount+ HD recorder) is priced anywhere between 12 to 15 lakhs and sometimes this can turn out more expensive than the operating microscopes used by many solo practicing ophthalmologists and even some of the medical colleges.
The story behind selecting the mirrorless cameras…
It is said, “If necessity is the mother of invention, frustration is the father of creativity.” It was our keen desire to be active in academics and teaching while working within the cost constraints, that motivated us to think of out of the box solutions and look for alternate devices that could fulfill our need of an affordable surgical recording system for vitreoretinal surgery in particular. The first thing we tried were the cheaper single-chip cameras which produced videos that were either too pixelated or too dark with the endoilluminator looking like a bulb on a dark screen. This made us realize that camera sensor requirements for retina and cataract surgery are very different. This is because of the difference in illumination sources used during surgery. A bright Halogen/LED light from the microscope is used for anterior segment surgeries while retinal surgeries are performed in low light using the light from a fine endo-illuminator probe. Hence, vitreoretinal surgery recording needs a sensor with high quantum efficiency, high signal to noise ratio and a broad dynamic range so that it can capture images in low light and can visualize the well-illuminated and dark areas equally well without producing a grainy video.
Only the high-end three-chip CCD medical cameras fulfilled these exacting requirements in the past. Commercial mirrorless cameras such as Sony A7s1 (priced 1.3lakhs) and Sony A7s2 (about 2lakhs about 3yrs ago, currently priced at 1.7 lakhs). fulfilled these criteria and were reasonably priced. These cameras are used extensively for high-resolution videography and low light astrophotography. The difference between a medical camera and a commercial camera lies in the sensor technology. Medical cameras use Charged Couple Device (CCD) sensors while the commercial cameras rely on CMOS (Complementary Metal-oxide Semiconductor) sensors. The two sensor technologies were developed in the 1960’s but it was the CCD sensor technology that gained popularity and underwent refinements for the next 3 decades. The CCD sensors have high quantum efficiency and were widely used for high-quality image acquisition such as broadcasting, space shuttle photography, and medical recording. The interest in CMOS technology was renewed with the expansion of low cost and less exacting digital imaging technology in the form of mobile phone cameras. The technological refinement of CMOS sensors has leapfrogged in the last decade to a point that today all Mirrorless cameras and professional movie cameras employ CMOS sensors. Low light image capture of these sensors is enhanced by the use of a technology called Backside illumination, which increases the quantum efficiency of the sensor plate from 60% to 90%. Sony was the first company to introduce backlit sensors for commercial use. They called them as the EXMOR R sensors and it is this technology that is integrated in Sony Mirrorless cameras. In our personal experience we have found the Sony A7S 2 to perform better than the commonly available DSLRs/Mirrorless camera from other established companies. (no financial interest; Kindly note we have not tested each and every camera due to cost constraints/ availability!). At the time when we started the experiments way back in 2016 Sony A7S2 was one of the few cameras that allowed internal 4K recording hence it was future ready.
The Recording Assembly (Figure 1)
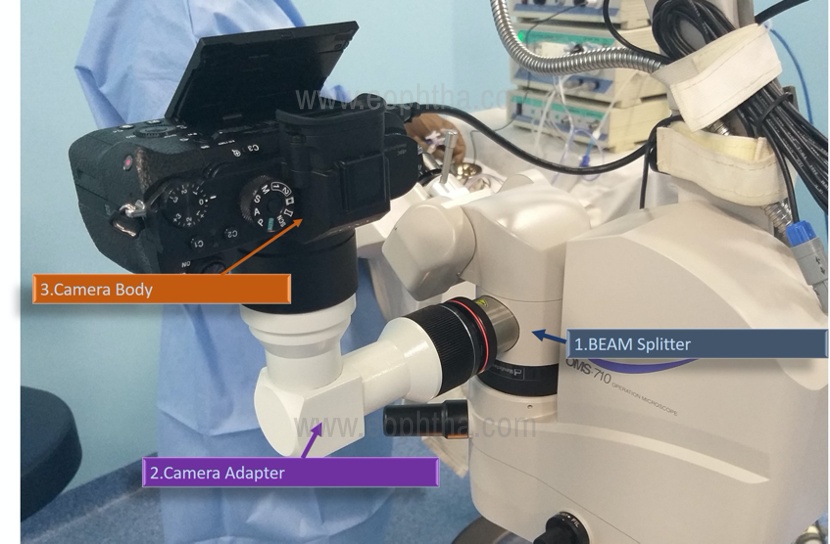
The fundamentals of the recording assembly remain the same whether using a CCD medical camera or a commercial camera i.e.
1) a beam splitter
2) a focusing adapter camera body and
3) Mirrorless Camera Body only (Sony/Panasonic/ Blackmagic)
The adapter is a fabrication fitted with an array of lenses to focus the light rays diverted from the beam splitter onto the camera sensor. The adapter is latched to the camera body in the same way as any lens is done. The other end on the adapter is inserted in the beam splitter tube and is secured in place with a tightening ring. Just like we have a C-mount adapter for the CCD cameras, mirrorless cameras need a focusing adapter which can be a Flexio-still adapter ( Carl Zeiss Inc.) or can be sourced from local sources ( We use the indigenous adapter from 3-D Medisys , Ambala, No Financial interests) The C-mount adapter used for CCD cameras have different focal lengths and hence cannot be used for the mirrorless cameras. Also each mirroless camera has different sensor size hence the focusing adapter required would be different and not interchangeable between the various camera bodies.
Also, when using CCD cameras, one needs an external recorder without which we cannot record, however in our method using the mirrorless cameras there is a high- speed SD card (64gb/128gb) in the camera which allows internal recording. So, there is no need to buy an external recorder unless the surgical volumes are too high. This also adds flexibility to the system and one can carry the whole setup in a camera carrying bag and use it between centers or operation theatres. It requires less than a minute to setup the system for recording.
Recording settings:
It is important to understand that the best photographs are not produced by the best cameras but by a good photographer who knows how to use his camera to its fullest potential. Recording surgical videos using mirrorless cameras is not a point and shoot affair! The users need to understand the camera settings and use it optimally to get the best results. This is because no two-microscope optics are the same, the efficiency of the beam splitter varies depending on the manufacturer and the type (50:50, 80:20, 90:10), so does the quality of the lenses used in the camera adapter. The settings need to be individualized for these variables in the first place. Although it may sound complicated it just takes a few seconds to change the settings in the camera once one becomes familiar with the camera settings. (detailed presentation can be watched on YouTube; AIOS 2020: Instruction course- A to Z of surgical video recording Chief Instructor Dr. Raju S https://youtu.be/2tIXpE4Kim4 )
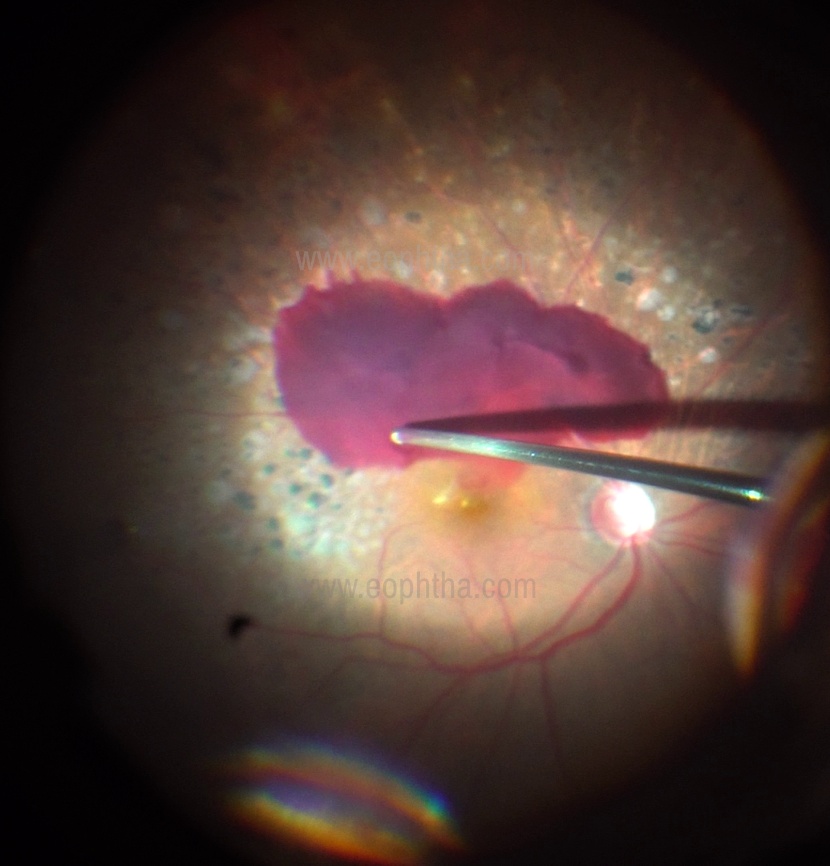
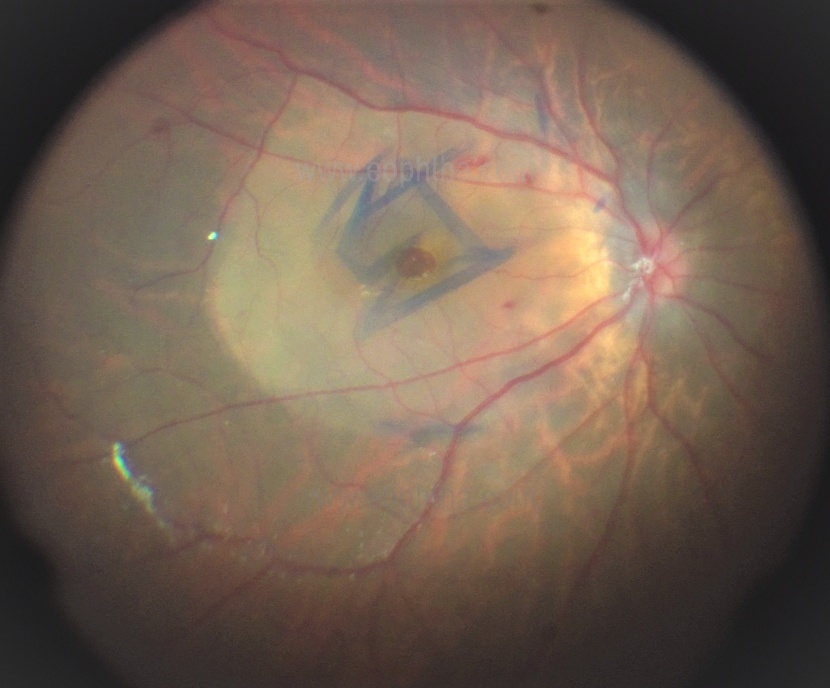
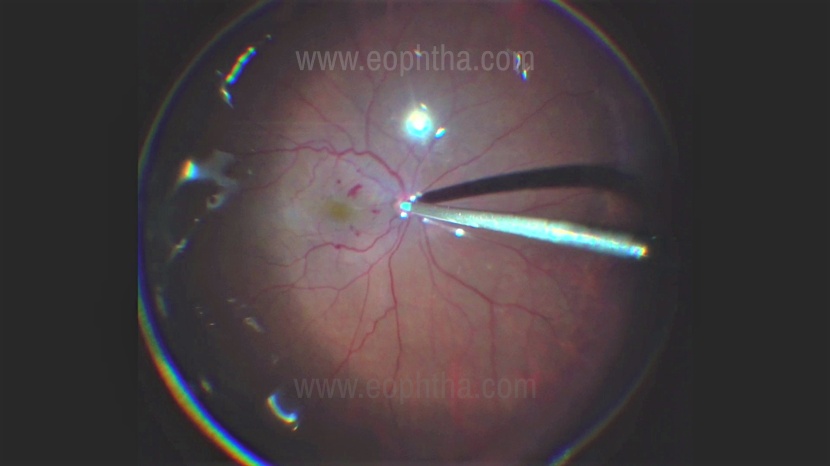
Briefly, the most important setting to adjust is the ISO of the camera. One can set the ISO setting in Auto mode keeping 100 as minimum and 1600 to 3200 as maximum initially for recording retinal surgeries. While recording anterior segment surgeries maximum ISO can be set at 400 to 800. Light during anterior segment surgeries is constant however, lighting in vitreo-retinal surgery is very dynamic during the surgical procedure. The human eye has a very broad dynamic range hence, we don’t see the difference while operating. The intensity of the light varies with the gauge of the surgery 23g vs. 25g vs 27g. Also, the light intensity varies depending on how the light pipe is used during some of the critical steps like ILM peeling along with the type of lens used. Some surgeons shine the light keeping it very close to the retina during ILM / membrane peeling. In these situations, the camera sensor cannot adjust to the excessive light hence there will be blooming in the video recorded. The trick to the great surgical recording is to have a uniform illumination and optimal use of the light pipe. We would suggest to use Chanderlier lights if one were to record an interesting case. Another tip is to hold the light pipe bit away from the retina. Also, by connecting the camera output to a TV monitor via the HDMI cable one can have a live view. The ISO setting can be modified using real time feedback from the monitor to get the optimal image quality for great videos. (few stills from various surgeries- Courtesy Dr Raju S)


Although one can record the best quality videos in Ultra High Definition (4K), it takes up a lot of memory space and would require high end computing for editing such videos. Also to appreciate the 4K quality videos one needs to have a 4k TV or 4k projector systems. Currently, in most conferences there is no facility to project 4k videos. In the present scenario recording in the best quality HD will suffice for all practical purposes. However, the system is future ready for 4k without need for any additional upgrade.
There are a few limitations to our system which can easily be overcome.
- Battery backup of 2.5 hour - There are three batteries which are supplied with the camera which can be kept charged on the day of surgery and changed as and when required. Another solution is connecting a USB power supply for continuous battery back-up.
- Continuous Recording limit of 30 mins: To overcome some tax laws this limit has been set in the camera. The simplest way to solve this problem is to ask your assistant to restart the recording button at 29th minute and continue recording for the next 30 mins. Otherwise one can buy external recorders (eg Blackmagic, Atmos shogun, Avermedia etc) either HD or 4K to have continuous recording without time limits.
Validation:
We have validated the video quality of Sony A7s2 to the current industry gold standard the Sony 3 chip full HD medical camera (Model no. PMW-10MDC) and the results were published in the Indian Journal of Ophthalmology.1 We established that Sony A7s2 was non-inferior to Sony 3 chip full HD medical camera in terms color, contrast and overall picture quality. Our work has also been acknowledged in the Survey of Ophthalmology.2
Conclusion:
Although we do agree that 3 chip medical-grade CCD cameras produce very high-quality videos it comes at a high cost too. If you can afford the best recording system then go for it! but for many of us for whom there are cost constraints, this innovative solution will deliver equally good videos at probably 1/3rd the cost of medical grade HD recording systems. Based on our experience we would say this system is “cost-effective and as effective” as the CCD cameras for all practical purposes and is a value for money option for those considering having a recording system for ophthalmic/retinal surgeries. Currently, there are at least 200 installations in India including some big institutes which are using this option.
Award
This innovative solution was also selected as one of the winning abstracts that were presented at the Retina World Congress 2019, at Fort Lauderdale, USA.
For further information contactrajusampangi@gmail.com or drkhanduja@gmail.com
References:
- Khanduja S, Sampangi R, Hemalatha BC, Singh S, Lall A.Use and validation of mirrorless digital single light reflex camera for recording of vitreoretinal surgeries in high definition. Indian J Ophthalmol. 2018 Jan;66(1):106-109. doi: 10.4103/ijo.IJO_511_17
- Sampangi R, Hada M, Sud R, Khanduja S. Letter to the editor: Video recording in ophthalmic surgery.Surv Ophthalmol. 2020;65(3):394-395. doi:10.1016/j.survophthal.2019.10.005
- AIOS 2020: Instruction course- A to Z of surgical video recording Chief Instructor Dr Raju S Sample Videos shot on Sony A7S2 mirrorless recording(Click the link)
- Epiretinal membrane removal(Click the link)
- Cataract Surgery(Click the link)