

Introduction:
Cataract is the second most common cause of preventable blindness worldwide and the most common cause of preventable blindness in India, affecting nearly 65.2 million worldwide [1-5]. To control the number, a high cataract surgery rate (CSR) is required. Sudden lockdown due to the current pandemic led to the cessation of elective cataract surgery [6,7], causing a sharp decline in the required CSR. In India as per the National Programme for Control of Blindness (NPCB) data 2018-19, the desired CSR was 947866 which could not be achieved [7]. As the unlock process has started, resumption of elective cataract surgeries is being initiated with precautionary measures. In this article, we have tried to summarize the current guidelines for elective cataract surgery.
Preferred practice for cataract surgery:
1. General measures:
The Govt. of India (GOI), Ministry of Health and Family Welfare (MoHFW) have advised certain preventive measures to avoid transmission (mask, hand hygiene, and social distancing) [6], and it must be followed everywhere. As the SARS COV-2 virus has a high rate of transmission and cross infection [7], some more precautions should be taken:
- Appointment based practice to prevent overcrowding in the waiting area.
- Well-trained and minimum staff for managing the OPD and Operating Room
- Regular infrared thermal screening of both employees and patients
- Questionnaire-based patient screening for symptoms of SARS CoV-2.
- Open door practice
- Full safety gear/standard PPE (Mask, gloves, eye gear, face shield, disposable gown, breath shield)
- Regular cleaning of all surfaces like tabletops, door handles etc. with 1% sodium hypochlorite solution.
- Use of the Arogya Setu app (if possible).
2. Patient Selection:
Sudden lockdown led to the postponement of planned cataract surgery and relinquished screening of new patients. As we are in midst of the pandemic and with the “unlock” announced, it is mandatory to prepare ourselves for resuming normal practice. Prioritization of patients based on ocular triage should be done and pre-evaluated patients prior to lockdown need to be telephonically contacted and planned for surgery. Also, new patients coming to the OPD should be screened and evaluated. Those having medical issues along with cataracts should be thoroughly assessed and planned only after clearance from concerned specialties. Eyes with mature, hypermature, lens-induced glaucoma, pediatric cataract and other ocular co-morbidity in which cataract precludes further treatment should be given priority.
|
Table 1: Criteria for patient selection for cataract surgery (proposed by RCOphth) [16] |
Criteria AThe patient has significant visual symptoms confirmed to be due to cataract Visual symptoms due to cataracts are impairing the patient’s activities of daily living, and it is anticipated that this will be improved by surgery |
Criteria BCataract surgery is needed to facilitate the management of ocular comorbidity, including but not limited to screening or treatment of diabetic retinopathy; glaucoma monitoring; treatment of angle-closure glaucoma |
Criteria CThe patient indicates a willingness to have cataract surgery following a discussion including: How the cataract affects the persons’ vision and quality of life Whether one or both eyes are affected Consequences of not undergoing surgery for ocular health, quality of life and other reasons such as continuing to meet legal driving standards |
3. Screening:
Various studies [8-15] have reported the presence of the virus in the ocular secretions of affected individuals. Hence it is important to take all necessary precautions. Social distancing should be practiced during the consultation and history taking [7]. Wearing of triple-layer surgical mask/N95 mask by the doctor and patient is deemed necessary, as by merely wearing a mask, the risk of transmission itself is highly reduced [17]. Handing over documents should be avoided [7], instead if possible, old documents should be shared over by email, WhatsApp, or Telegram.
4. Pre-op evaluation:
- Visual acuity testing: Avoid using occluder, patient should use their hand to cover the eye not being examined. Testing should be done from the smallest possible letter over the vision drum to finish the test as fast as possible [7].
- Intraocular Tension: To be measured only if signs of raised IOP are present, the patient is on any kind of steroids, is known case of glaucoma, or planned for cataract surgery. To record the IOP Goldman applanation tonometer, Schiotz tonometer or Tonopen. The tip should be cleaned with 70% isopropyl alcohol between cases and with 1% Sodium hypochlorite at the beginning and end of OPD day. Non-contact tonometer (NCT) should be avoided as it is an aerosol-generating procedure [7].
- Lacrimal Sac: The patency of the lacrimal sac can be assessed by ROPLAS method by wearing examination gloves or using fluorescein dye . In suspected cases of nasolacrimal duct blockage, cataract surgery should be postponed. Syringing should be avoided as it is an aerosol generating procedure. [7]
- Slit-lamp Examination: Breath shield should be present to prevent transmission through aerosolized respiratory droplets. Single person policy should be considered to prevent the transmission to other HCW’s. Slit lamp should be cleaned with 70% isopropyl alcohol before examining another patient [18].
- Fundus evaluation: Retina of all patients undergoing cataract surgery must be examined, preferably using an Indirect ophthalmoscope or 90 D or 78 D lens and use of direct ophthalmoscopes should be avoided [7].
- Biometry [7]: Ultrasound Biometry- The tip of the probe should be cleaned with alcohol swab after every case and sufficient time to dry up should be given. In case of use of immersion scan, cleaning of the Prager shell along with the probe should be done with clean fluid. Whereas Optical biometry, is the preferable method for measuring the eye. The main instrument panel should be cleaned using a soft, lint‑free cloth dampened with 70% Isopropyl alcohol. All necessary cleaning should be followed as per manufacturer’s guidelines of each machine to avoid inadvertent damage by the cleaning solutions. Breath shields should be incorporate between the technician and the patient to prevent direct contact with the aerosols generated. The joystick, locking screw for the instrument base, head rest, chin rest, handlebar which the patient holds, keyboard and touch display should be cleaned with isopropyl alcohol 70% after every test.
- Keratometry: Any keratometer can be used. The breath shield can be customized and placed as a barrier. The joystick, locking screw for the instrument base, head rest, chin rest, handlebar should be cleaned using alcohol swab after examining each patient [7].
5. Counseling:
All the necessary information regarding surgery should be communicated either on the first visit for new cases or telephonically for pre-listed cases. Instructions for surgery‑day should be explained. Important information must be shared by phone, e-mail, or WhatsApp. Special COVID-19 consents can be added to the preoperative protocol [19].
6.Choice of Surgery:
The choice of surgery is primarily resource and surgeon dependent. Even-though phacoemulsification is the most preferred technique and considered as the gold standard [20] for cataract extraction, Manual Small Incision Cataract Surgery (MSICS) is equally practiced in a large part of the country. The debate on which technique is better has been going on for long and various studies have quoted the benefits over each other. The much-debated concern is the transmission of the virus through aerosol generated during cataract surgery. Although the presence of the virus in aqueous has not yet been confirmed by any authority, also the chances of transmission through aerosol in cataract surgery is exceptionally low [17]. According to AAO and AIOS, the aqueous is replaced by the viscoelastic initially and later by balanced salt solution (BSS) hence the aerosol generated is of the BSS and/ or viscoelastic [7,17]. The role of povidone-iodine 5% prior to surgery has also shown active response against the SARS CoV-2 virus [7,17]. Another source for aerosol generation is through wound/incision, which can be minimized by regular wetting of the ocular surface and incision site by viscoelastic [21].
|
Table 2: Techniques for preventing aerosol generation in different surgical techniques. |
|
Phacoemulsification [21] |
|
Method to minimize aerosol generation |
|
|
Manual Small Incision Cataract Surgery (MSICS) |
|
7. Role of pre-operative testing for SARS CoV-2:
ICMR reports state that more than 80% of those who were tested positive were asymptomatic and with limitations in the availability of diagnostic tests, it is prudent to assume that all patients are potential COVID-19 positive patients. Thus, it is necessary to take additional precautions during cataract surgery and perioperative period. But the mandatory pre-operative testing for SARS CoV-2 for elective cataract surgery is still undecided [6,17].
8. Operating room (OR) safety measures: [22,23]
- Well trained and minimum staff to assist the surgery
- Surgery to be done by well-trained surgeons to fasten the process.
- Disinfection of the OT should be done after each case as per guidelines by CDC.
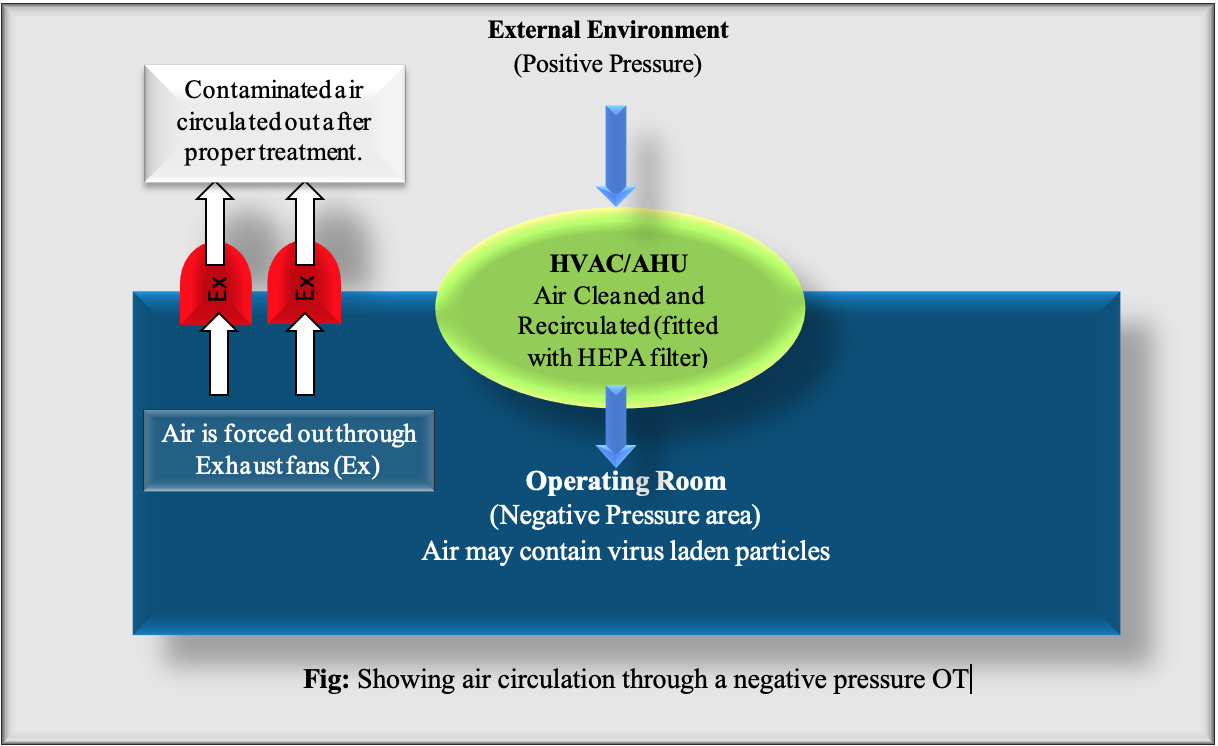
- The most important factor is to ensure that the virus laden airborne particles shouldn’t escape the room occupied by patient and simultaneously maintain a low concentration of viral load inside the OR in order to control the spread of infections and also to protect HCW’s.
- As all pre-existing OR’s are recirculatory type positive pressure OR’s, it is important to convert them into a non-recirculatory type, negative pressure OT (>5 Pa), with the recommended temperature of 24 to 30° C and relative humidity of 40 to 70%.
- This can be achieved by blocking off the return air vents in the OR. Air Handling Unit (AHU) must be a dedicated one for every OR and must have the provision of receiving adequate outdoor air supply. Additionally, an independent exhaust blower shall be provided to extract the room air and exhaust out into the atmosphere, after suitable “exhaust air treatment” by high-efficiency particulate air (HEPA) filtration. If not possible, then chemical disinfection (1% hypochlorite) or Ultraviolet (UV) irradiation or heating at 75° C can also be done.
- Places where availability of AHU is not possible, the option to have stand-alone room air-conditioners (Split AC of 2 tons each) can be considered as they re-circulate air within a single occupied zone. Recirculation of cool air by room air conditioners must be accompanied by outdoor air intake through exhaust by natural exfiltration. Fresh air intake through a fan filter (or a HEPA filter) unit will prevent outdoor dust entry and exhaust fans should be kept operational.
9. Intra-op safety tips:
It is important to take precautions and ensure complete safety while operating.
- Patient to wear a surgical mask (mask with respirators are not to be used) [17].
- The operating surgeon must wear an N 95 mask.
- Eye gear should be worn.
- Sterile double gloves should be worn and changed after every case.
- Use of standard PPE kit.
- Proper care must be taken to avoid any cut or needle prick during any procedure as the chance of infection through wound may be high.
- Ensure proper draping to prevent respiratory droplet infection.
- Use of 10% povidone Iodine for extraocular use and 5% for ophthalmic use pre and post-surgery.
- Although the chances of getting infected through aerosol generation during cataract surgery remain unclear, a new method of preventing aerosol spread is by creating a barrier using surgical drape [24].
10. Post-operative Care:
Patients following cataract surgery should not be called frequently to the clinic/hospital to prevent infection. They should be seen on the first post-op day and the rest of the follow-up should be done through telemedicine at 14th and 30th post-op day. They should be counseled about alarming signs for which they should consult on an emergency basis.
Conclusion:
Unlike novel coronavirus, cataracts may not systemically jeopardize the patient’s condition, but it surely does make one helpless and dependent by making them visually handicapped and also affects the health-related quality of life. The current pandemic may have slowed down our progress in fight against preventable blindness, but with careful and alert actions we can learn to live and survive the pandemic and continue to provide a safe and high-quality ophthalmic care and deflate the global burden of preventable blindness due to cataract. At the same time, the safety of ourselves and the surgical team should be paramount in our scheme of things so that we tide over this period of crisis by staying safe healthy, and alive. This is possible by being resilient, adaptable, and willing to learn from each other’s experiences.
References:
- World Health Organization 2010, “Vision 2020 action plan 2006,” 2010. Available from http://www.who.int/entity/blindness/Vision2020 report.pdf. [Last Accessed on July 20, 2020]
- Rao GN, Khanna R, Payal A. The global burden of cataract. CurrOpin Ophthalmol. 2011;22:4–9.
- Directorate General of Health Services. “National Programme for Control of Blindness and Visual Impairment (NPCB&VI)”. Available from https://dghs.gov.in/content/1354_3_NationalProgrammeforControlof BlindnessVisual.aspx [Last Accessed on July 28, 2020]
- World Health Organization 2019, “Blindness and Visual Impairmnet” 2019. Available from https://www.who.int/news-room/fact-sheets/detail/blindness-and-visual-impairment. [Last Accessed on July 29, 2020]
- Review of Ophthalmology, “Thoughts on Cataract Surgery-2015”. Available from https:// www.reviewofophthalmology.com/article/thoughts-on--cataract-surgery-2015. [Last accessed on July 20, 2020].
- Sengupta S, Honavar SG, Sachdev MS et al. All India Ophthalmological Society‑Indian Journal of Ophthalmology consensus statement on preferred practices during the COVID‑19 pandemic. Indian J Ophthalmol 2020;68:711‑24.
- Reddy JC, Vaddavalli PK, Sharma N et al. A new normal with cataract surgery during COVID-19 pandemic. Indian J Ophthalmol 2020;68:1269-76.
- Peng Y, Zhou YH. Is novel coronavirus disease (COVID 19) transmitted through conjunctiva, J Med Virol, 2020 Mar 16.
- Lu CW, Liu XF, Jia ZF. 2019 nCoV transmission through the ocular surface must not be ignored. Lancet 2020;395:e39.
- American Academy of Ophthalmology, Coronavirus kills Chinese whistleblower. Available from: https// www.aao.org/headline coronavirus kills Chinese whistleblower Ophthalmol. [Last accessed on July 20, 2020].
- Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020 Feb 28.
- Wu P, Duan F, Luo C, et al. Characteristics of Ocular Findings of Patients with Coronavirus Disease 2019 (COVID 19) in Hubei Province, China. JAMA Ophthalmol. 2020 Mar 31.
- Xia J, Tong J, Liu M, Shen Y, Guo D. Evaluation of coronavirus in tears and conjunctival secretions of patients with SARS‐CoV‐2 infection. J Med Virol 2020.
- Sun X, Zhang X, Chen X et al.The infection evidence of SARS-COV-2 in ocular surface: a single-center cross-sectional study. medRxiv 2020.02.26.20027938
- Zhou Y, Zeng Y, Tong Y, et al. Ophthalmologic evidence against the interpersonal transmission of 2019 novel coronavirus through conjunctiva. medRxiv 2020.02.11.20021956
- The Royal College of Ophthalmologists, UKISCRS, “Cataract surgery guidelines for Post COVID-19 pandemic: Recommendations”. Available from https://https://www.rcophth.ac.uk/wp-content/uploads/2020/05/RCOphth-UKISCRS-COVID-cataract-surgery-restoring-services-070520.pdf. [Last Accessed on July 27, 2020]
- American Academy of Ophthalmology, “ Special considerations for ophthalmic surgery during the COVID-19 pandemic”. Available from https://www.aao.org/headline/special-considerations-ophthalmic-surgery-during-c. [Last Accessed on July 20, 2020]
- Bhalla JS, Mehtani A, Gothwal Y, et al. Ophthalmology practice in the era of COVID-19 pandemic. DOS Times.2020 Jan-Feb; vol 25:18-24.
- All India Ophthalmology, “Ophthalmic Practice Guidelines in the current context of COVID-19”. Available from https://aios.org/pdf/Ophthalmicpracticeguidelines in the current context covid19.pdf. [Last accessed on July 20, 2020].
- Gogate P. Comparison of various techniques for cataract surgery, their efficacy, safety, and cost.Oman J Ophthalmol. 2010;3(3):105-106
- Darcy K, Elhaddad O, Achiron A et al. “Reducing visible aerosol generation during phacoemulsification in the era of Covid-19”.medRxiv2020.05.14.20102301
- NABH, “Revised Guidelines for Air Conditioning in Operation Theaters 2018”. Available from https://www.nabh.co/images/pdf/RevisedGuidelines_AirConditioning_OT2018-final.pdf. [Last Accessed on May 10, 2020]
- Malhotra N, Bajwa SJ, Joshi M, Mehdiratta L, Trikha A. COVID Operation Theatre‑ Advisory and Position Statement of Indian Society of Anaesthesiologists (ISA National). Indian J Anaesth 2020;64:355-62
- Extra microscope draping for intraocular surgery. ESCRS EuroTimes. Available at: https:// www.eurotimes.org/covid-19-video-extra-microscsopedraping for intraocular surgery. [Last Accessed July 20, 2020].