

Ocular surface anatomy
The ocular surface, in a strict sense, consists of the cornea and its major support tissue, the conjunctiva. In a wider anatomical, embryological, and also functional sense, the ocular mucosal adnexa (i.e. the lacrimal gland and the lacrimal drainage system) also belong to the ocular surface. The ocular surface occupies approximately 2.2 cm2 of the human body surface area [1]. The homeostasis of this small area is, however, extremely important for clear vision and comfort. The cornea is one of the most densely innervated structures in the body and hence, surface changes can result in significant discomfort apart from vision loss. The clarity and tectonic integrity of the cornea are maintained by a number of mechanisms, and one of the most important of these is the intactness of the surface epithelium. The limbus provides a constant source of epithelial cells to maintain the normal turnover of the corneal surface but can be impacted by multiple noxious influences including trauma, infection, immunological processes, degenerative changes, and loss of innervation. If methods to restore the integrity of the corneal epithelium fail, then in some select instances, the use of healthy conjunctival epithelium as a replacement can result in good outcomes, promoting comfort and maintaining the integrity of the ocular surface. This procedure is primarily used to bring symptomatic relief and has no effect on visual prognosis.
1. The rationale for use of conjunctival flaps and types of flaps
The intactness of the corneal surface depends not only on the supply of a healthy epithelium, but also on the integrity of the underlying basement membrane and stroma, as these serve as the base for a healthy epithelium. When there is stromal ulceration that in unresponsive to medical treatment, as in chronic infections, or neurotrophy, the use of a conjunctival flap promotes healing. The various mechanisms postulated for the use of these flaps include:
- Reduce collagenolysis by limiting exposure of the ulcerated surface to tears and leucocytes
- Reduce blink related trauma
- Protecting the surface from exposure and drying.
- Providing nutrition to the corneal surface from the vascularized flap, which transects the superficial vessels entering the cornea via the peritomy site.
Various types of flaps can be used - broadly they can be free grafts or pedicle grafts. Most of the procedures utilize pedicle grafts as this allows the graft to have its own blood supply. These can in turn be partial, covering one part of the corneal surface, or total, covering the entire corneal surface. The latter approach has been termed the Gundersen flap.
2. History
Although Trygve Gundersen is widely credited with the eponymously named procedure of conjunctival hooding or total conjunctival flap, which he described in his article published in 1958, the use of conjunctival flaps predates this. Their application was described by Schöler J in 1877; by Krebs in 1878; by Kuhnt in 1883; by Meyer in 1892, and by Kuhnt from 1889 to 1906. Van Lint, writing in 1912, is generally credited with popularizing their use, but he used them primarily to reinforce cataract sections. Some of these approaches - used to cover corneal injuries and disease, utilized a purse string suture to drag the conjunctiva over the cornea, or a non-dissection method of mobilizing the forniceal conjunctiva, and were not intended as permanent methods of cover. These are no longer in use today.
3. Indications for performing a conjunctival flap
The original indications for the procedure, according to Gunderson [2], include :
- Herpetic ulcers
- Fascicular keratitis
- Neuroparalytic keratitis
- Relapsing erosions
- Bullous keratopathy
- Marginal ulcers including Mooren’s ulcer
- Filamentary keratitis
- Painful blind eyes.
Over time, other indications have included corneal infections that are unresponsive to medical therapy, especially in situations where access to donor corneal tissue is limited or unavailable. They are also used to treat corneal perforations in a similar situation, where the procedure is used as a temporary measure to preserve the eye until further definitive surgery can be performed. With improvement in medications including antibiotics and anti-inflammatories, an improved understanding of corneal disease processes, availability of adjuncts like amniotic membrane, cyanoacrylate glue, and better access to donor corneal tissue, many of these indications can now be managed using other modalities.
Current indications for conjunctival hooding include:
- Painful blind eyes with bullous keratopathy
- Improvement of cosmesis in disfigured eyes prior to cosmetic lens fitting.
- Recalcitrant and recurrent herpetic stromal ulceration in a non-seeing eye or if the visual axis is not involved.
- As an emergency measure in Non-responding infectious keratitis or small corneal perforations.
4. Surgical procedure
The procedure of using the conjunctiva to cover the entire cornea – Gundersen’s flap, can be performed using orbital infiltration anesthesia. A 6-0 silk or vicryl corneal suture is used to pull the globe in an inferior direction, to allow access to the superior bulbar conjunctiva. The normal depth of the superior fornix is about 16 mm [3]. A superior rectus bridle suture is avoided to prevent tears in the superior conjunctiva. The corneal size in the vertical meridian is measured using Vernier calipers. It is usually 11-12 mm [4]. Once the superior bulbar conjunctiva is exposed, marks are made circumferentially, parallel to the superior limbus using a gentian violet marker. The marks are made after drying the conjunctival surface,11 to12 mm from the limbus, matching the measured corneal size. Although not mandatory, a local infiltration of anesthetic (2% Lignocaine) in the subconjunctival plane to balloon up the conjunctiva can be done to aid in dissection. Care is taken to avoid penetration of the needle in the area that will be used for the flap as small perforations can enlarge in the postoperative period. It is also important to inject the solution in the correct plane. Injection into the Tenon’s fascia results in ballooning, thereby making dissection difficult.
Westcott scissors are used to make a circumferential incision in the conjunctiva following the Gentian violet marks made previously. The conjunctival flap is carefully dissected towards the superior limbus. Care is taken to avoid including the Tenon’s tissue when dissecting the conjunctival flap. A tenon’s rich flap may contract both during and after surgery leading to graft retraction, corneal exposure and poor cosmesis. During the dissection, while an assistant can help by holding the superior edges of the flap with non-toothed forceps to tent up the tissue allowing the surgeon to dissect more easily, it is important that the movements are coordinated. Excessive or inadequate force used to retract the tissue in the area of dissection may cause button-holing of the flap, which is best avoided. When the dissection reaches the superior limbus, a perforation is made in the attachment of the conjunctiva to the limbus at 12 o’clock, by using a slit knife from the conjunctival epithelial side, or by cutting through with the tip of the scissors from the conjunctival stromal side. This incision is then continued all around the limbus for 3600 keeping the peritomy flush with the limbus.
The next step would be to carefully remove the corneal epithelium. Attention is then paid to removing the corneal and limbal epithelium completely. Retention of epithelial nests on the cornea results in poor flap adhesion. The presence of limbal epithelium can result in cysts under the conjunctival flap. Once this has been accomplished, the superiorly dissected conjunctival flap is brought down and stretched over the denuded corneal surface, taking care to avoid button-holing the flap. Relaxing incisions in the two ‘handles’ of the flap may be required, to allow the flap to lie over the corneal surface without tension. The flap is then sutured to the limbal zone using 4 to 5 interrupted 10-0 nylon sutures. Sutures are used to secure the inferior edge of the conjunctival flap to the underlying episclera at the limbus and the edge of the conjunctival peritomy to restore the continuity of the conjunctiva. The sutures used can be 10-0 nylon or 6-0 vicryl. The use of fibrin glue has also been recently described [5]. This saves time and effort, but increases the cost of the procedure. If sutures are used, the knots need not buried and can be removed between 4 and 6 weeks following surgery on an Out-Patient basis under topical anesthesia. An inferior forniceal injection of antibiotic-steroid can be used, but is not mandatory. It is best avoided if the indication for flap surgery is a corneal infection. A pad is used to protect the eye in the immediate post-operative period. The surgical procedure for a conventional Gunderson Conjunctival flap is outlined in Figure 1.
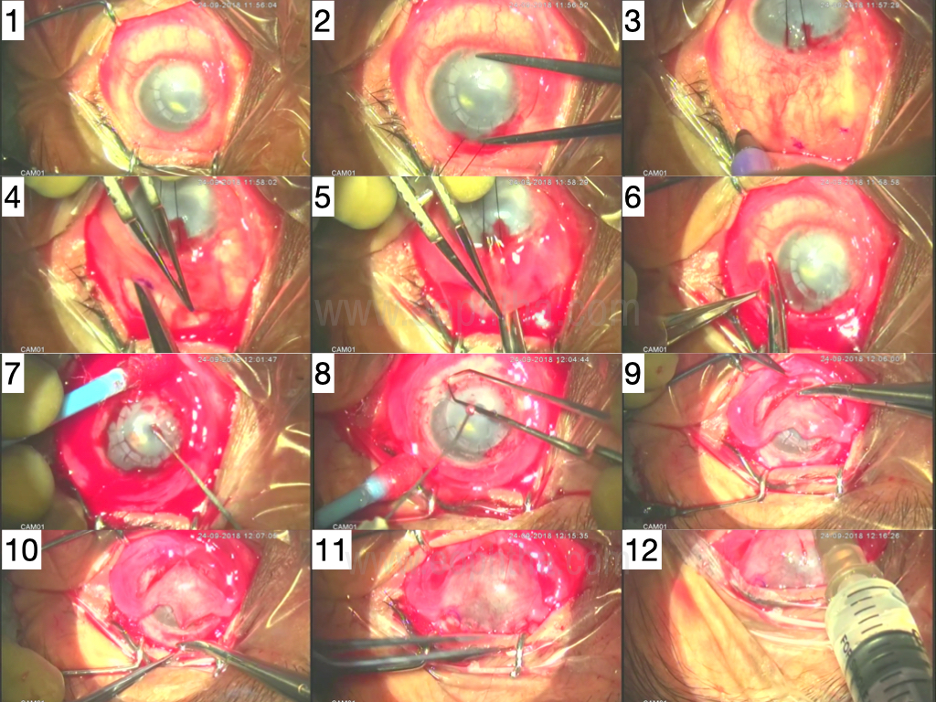
Figure 1 Composite picture of the surgical technique
- Failed graft with painful corneal edema - eye with no visual potential
- Measuring the vertical corneal size with calipers as 11 mm
- The eye moved down with a 6-0 silk suture at 12 o’clock cornea and marks made in the superior bulbar conjunctiva 11 mm from the limbus
- Incising the conjunctiva along the marks using Westcott scissors and dissecting toward the superior limbus
- Perforating the conjunctiva at the superior limbus using the Westcott scissors
- Completing a 3600 peritomy, close to the limbus
- Removing the corneal and limbal epithelium with a hockey stick knife
- Achieving hemostasis using wet field cautery
- Positioning the flap over the cornea and inferior sutures incorporate the inferior edge of the flap, the limbal episclera and the edge of the bulbar conjunctiva
- The superior edge of the flap sutured to the superior libel episclera
- Appearance at conclusion with complete coverage of the cornea without tension on the flap
- Inferior forniceal injection of antibiotic - steroid.
A similar approach, as described above, is used for partial conjunctival hooding, but a superficial keratectomy is created to produce a bed for the conjunctival flap as the edge of a partial flap lying on the surface of the cornea is likely to be constantly contacted by the edge of the lid during blinking. The edge of the corneal bed is marked with an appropriately sized trephine and a lamellar corneal dissection is performed to create the bed. The flap is secured by 10-0 nylon sutures and the knots are buried, taking care to avoid the pupillary area if possible.
6. Postoperative care
The patient is examined the following day with the pad in place. The same is removed in the OPD and examination is performed to ensure the absence of infection and ensure that the flap is intact and viable. Postoperative care includes the use of topical steroid drops for 4 weeks, starting at 4 times daily and tapering 1 drop per week, and the use of an antibiotic eye ointment, 3 times a day for a week, tapered over 2 further weeks. The use of the antibiotic ointment helps to reduce suture irritation, especially in the first postoperative week. A final visit is performed at 1 month after surgery, when any remaining sutures are removed.
7. Complications
Complications are rare if the flap is performed using good technique. The most commonly encountered complication is a flap button-hole. If small, the area of the button-hole can be secured to the underlying cornea with an interrupted 10-0 nylon suture, although it is best avoided, to prevent further flap trauma. Postoperatively, a hematoma under the flap is occasionally seen and if small can be observed. If the hematoma is large, evacuation is done in order to allow the graft to adhere to the underlying stromal surface. Retraction of the graft with exposure of the underlying corneal stroma is seen if the flap size is inadequate. This occurs if the relaxing incisions fashioning the handles were inadequate, if the sutures are loose or cut through, or if there was excessive Tenon’s in the graft causing contraction. Graft melt occurs usually when the procedure is performed in an uncontrolled corneal infection, or if the handles are compromised resulting in inadequate blood supply to the graft.
8. Outcomes
If performed well, a conjunctival flap remains a gratifying procedure with excellent outcomes. The flap allows for pain relief in bullous keratopathy as the flap adheres to the underlying corneal stroma and unlike the corneal epithelium and does not allow the formation of bullae. In eyes with an irregular corneal surface that precludes the safe use of a cosmetic contact lens or shell, the conjunctival flap provides a robust surface that can support the daily insertion and removal of a cosmetic device without the risk of injury or infection. In a recalcitrant herpetic stromal ulcer, the presence of the flap allows the stromal disease to remit and healing to proceed. Figure 2 shows the post-operative outcome in a well-done conjunctival flap with adequate surface cover and acceptable cosmesis.

Figure 2 - Postoperative picture of a conjunctival hood
9. Disadvantages
There are very few disadvantages to the procedure, the chief being the inability to visualize the underlying cornea and anterior chamber, at least in the early postoperative period. However, in a patient with bullous keratopathy, this is not important as there is no active underlying corneal or anterior chamber disease. Inclusion of Tenon’s fascia or inadequately sized peripheral flap handles can cause temporary ptosis of the upper lid.
10. Alternate approaches
Amniotic Membrane transplantation can be performed in patients with painful bullous keratopathy associated with either inadequate conjunctival cover or a bleb. Amniotic membrane can provide an adequate replacement option to counter the pain from the erosions. Anterior stromal puncture can also be considered to manage this problem, but both of these procedures do not offer a robust solution as a conjunctival flap. In recurrent stromal keratitis with melt, the use of cyanoacrylate glue or amniotic membrane transplantation can be considered.
References
- Niederkorn JY, Kaplan HJ (eds): Immune Response and the Eye. Chem Immunol Allergy. Basel, Karger, 2007, vol 92, pp 36-49.
- Gundersen T, Pearlson HR. Conjunctival flaps for corneal disease: their usefulness and complications. Trans Am Ophthalmol Soc. 1969;67:78–95.
- Jutley G, Carpenter D, Hau S, Booth D, Jasim HA, Tay E, et al. Upper and lower conjunctival fornix depth in healthy white caucasian eyes: a method of objective assessment. Eye. 2016 Oct;30(10):1351–8.
- Sridhar MS. Anatomy of cornea and ocular surface. Indian J Ophthalmol. 2018 Feb;66(2):190–4.
- Chung H-W, Mehta JS. Fibrin glue for Gundersen flap surgery. Clin Ophthalmol. 2013;7:479–84.