

A. Introduction
There have been multiple refinements in the terminology of the epithelial squamous neoplasia until the introduction of the term “Ocular surface squamous neoplasia” (OSSN) by Lee and Hirst in 19951. OSSN is an umbrella term and refers to a spectrum ranging from mild/moderate/severe dysplasia to carcinoma in situ to invasive squamous cell carcinoma involving the conjunctiva and/or cornea2-4.
OSSN is the most common tumor of the ocular surface. According to the epidemiological studies, the worldwide incidence of OSSN is 0.02 to 3.5 cases per 100,000 people. Incidence increases with decreasing latitude, being higher in countries located close to the equator. OSSN predominantly occurs in the elderly age group (6thto 7thdecade) and in male gender 5-9.
B. Etiology and pathogenesis10-27
The presumptive risk factors implicated in the etiology of OSSN include:
- Excessive exposure to ultraviolet radiation
- Heavy cigarette smoking
- Immunosuppressive conditions: Human Immunodeficiency Virus (HIV) infection; Acquired Immunodeficiency Syndrome (AIDS), Chronic use of immunosuppressants; Post-organ transplantation
- Xeroderma pigmentosum
- Ocular surface injury
- Exposure to chemicals
- Vitamin A deficiency
- Human Papilloma Virus (HPV) infection
- Increased p53 expression
- Mutations in limbal stem cells
C. Clinical presentation
Symptoms:
Ocular surface squamous neoplasia is mostly unilateral and is seen in middle-aged and older male patients. Rarely, it is bilateral, and in the case of bilaterality, it is most commonly associated with immunosuppression or xeroderma pigmentosum 28, 29.
Patients with OSSN tend to present with the mass on the ocular surface, redness, foreign body sensation, watering, and pigmentation in the eye. Sometimes, it can be asymptomatic and an incidental finding during a routine eye examination. A defective vision occurs if the cornea is involved.
Signs
Clinically, OSSN has a myriad presentation, making the diagnosis challenging at times. It typically presents as a fleshy sessile lesion adjacent to the limbus in the inter-palpebral region involving the cornea and/or bulbar conjunctiva. The tarsal conjunctiva and fornix are less frequently involved. Mutations in limbal stem cells have been postulated to be the reason for the limbal location of OSSN. However, the origin of tarsal-based OSSN and the role, if any, of epithelial stem cells at the eyelid margin remains unknown.
The lesion may be flat or elevated. The thickness of the lesion is not directly related to the invasive nature of squamous cell carcinoma. Even reasonably thick tumors can be noted to be limited to epithelium. They can be localized or diffuse, and typically associated with varying degrees of surface keratin, feeder conjunctival blood vessels feeding and draining the lesion and intrinsic vascularity. They are usually pearly grey to pinkish-red in color, depending on the vascularity of the lesion. They can be sometimes associated with varying patterns of pigmentation resulting in an erroneous diagnosis of melanoma 30, 31. (Figure 1A).
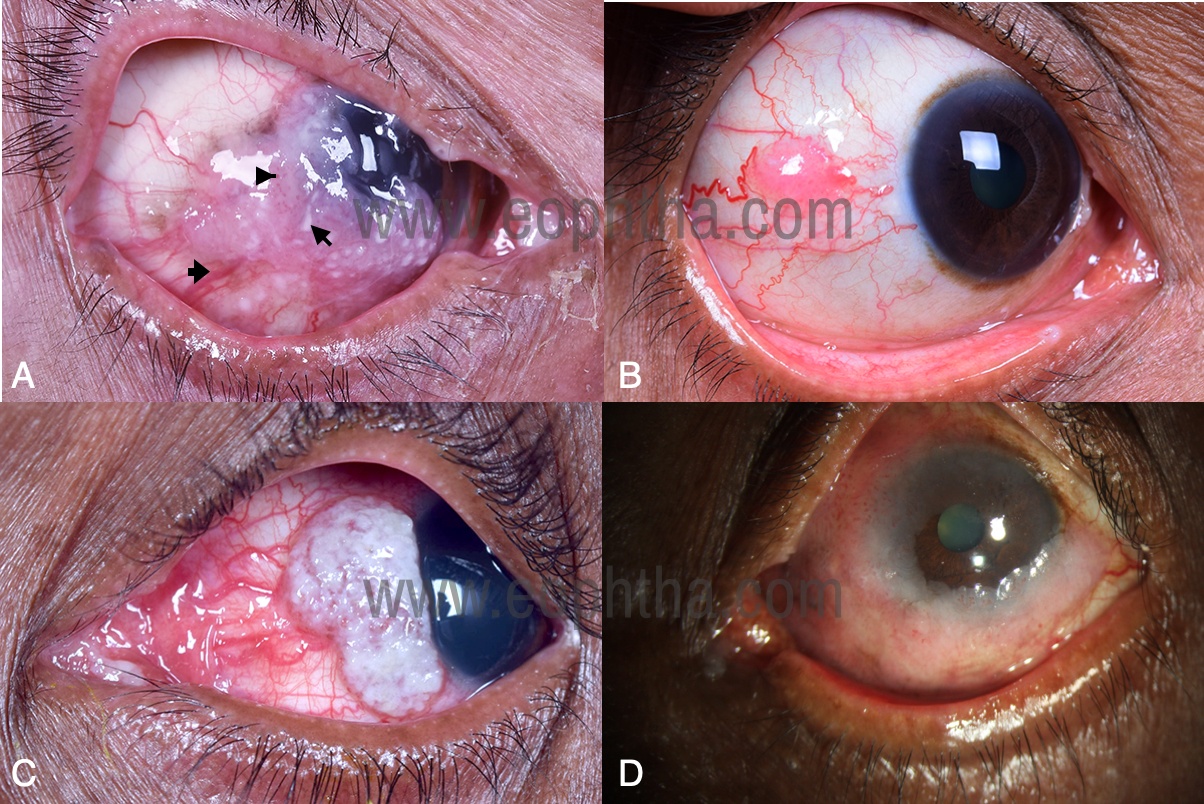
Figure 1: Clinical features of ocular surface squamous neoplasia (OSSN)A. OSSN with surface keratin (long arrow), feeder conjunctival blood vessels (short arrow), and intrinsic vascularity (arrowhead).B. Small OSSN measuring 5 mm in basal diameter and involving 1 clock hourC. Large OSSN measuring 13 mm and 5 clock hours of limbus D. Diffuse OSSN measuring > 15mm basal diameter with > 6 clock hours of limbal involvement
Tumor size is measured by the greatest linear diameter and by surface area. For rectangular areas, the surface area of the tumor is computed by multiplying the length by the breadth of the lesion. For circular areas such as the corneal surface, the surface area is estimated based on the normal corneal area of 120mm2.
Based on the number of clock hours of limbal involvement or maximum basal diameter, the tumor can be classified as (Figure 1B to 1D)
- Small (<5mm basal diameter or
- Large (6-15mm basal diameter or >3-6 clock hours of limbal involvement)
- Diffuse (> 15mm basal diameter or > 6 clock hours of limbal involvement)
Giant OSSN is another name for the diffuse type, defined as a single tumor greater than 15mm in greatest diameter (half the distance of horizontal eyelid aperture) or involvement of 180 degrees of the limbus (6 clock hours or half the limbal circumference).
Multifocal OSSN
Multifocal OSSN is rare and is reported in 4% to 26% of cases. Multifocal tumors are described by the presence of 2 tumors separated by a minimum of 5 mm distance in between them. They are aggressive in nature with the most common systemic association being HIV or AIDS. They are more prone to intraocular invasion necessitating the need for orbital exenteration 32, 33.
D. Morphological variants of ocular surface squamous neoplasia:
The major clinical variants of OSSN are: (Figure 2)
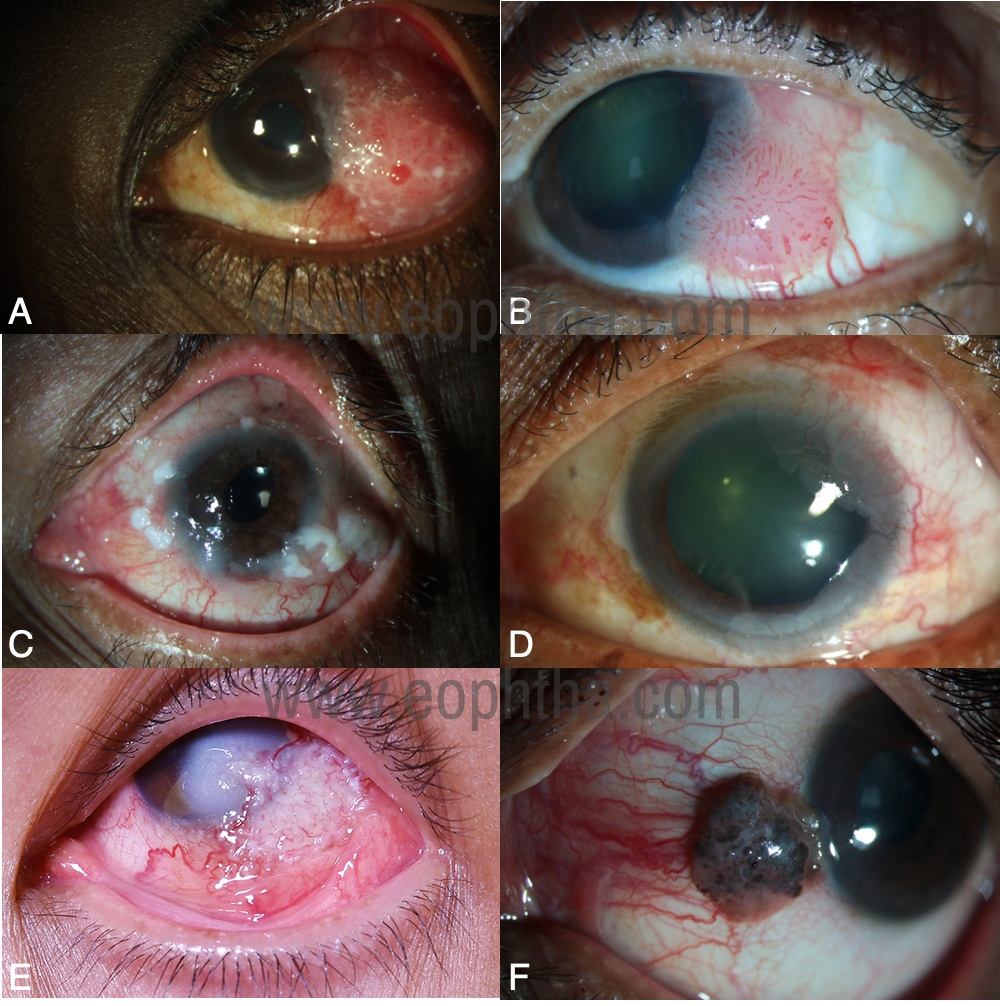
Figure 2: Morphological variants of ocular surface squamous neoplasia (OSSN)A. Nodular variant B. Papillary variant C. Gelatinous variant D. Placoid variant E. Noduloulcerative variant F. Pigmented variant.
- Nodular variant: They are typically circumscribed, raised, rapidly growing with an increased tendency for local invasion and metastasis to regional lymphnodes.
- Papilliform variant: As the name suggests, it has multiple fine finger-like configurations. They are fleshy, strawberry-like, with a stippled red appearance corresponding to its fibrovascular core and typical hairpin configuration of the associated conjunctival blood vessels. They are usually devoid of keratin.
- Placoid variant: These types are usually circumscribed and flat. They are relatively longstanding and less aggressive.
- Gelatinous variant: They are circumscribed and slimy in appearance with a tuft of superficial blood vessels.
- Noduloulcerative variant: They are rare and characterized by localized ulceration/necrosis of the conjunctiva without any distinct visible conjunctival mass. They have diffuse inflammation with localized corneoscleral thinning and often complain of pain. Any such lesion with keratin should raise a suspicion of noduloulcerative variant of OSSN.
- Pigmented variant: They are associated with varying patterns of pigmentation 34.
- Corneal OSSN: Corneal OSSN typically have ground glass sheet or frosted appearance with sharply defined fimbriated borders or pseudopodia like configuration and heaped up edges, best noted on retroillumination. Sometimes, they have an adjacent neoplastic pannus for metabolic support to these abnormal cells. They are usually translucent greyish-white avascular or minimal vascular lesions limited to the corneal epithelium. These lesions are typically indolent, slow-growing, and prone to recurrence 35.
E. Diagnostic modalities
1. Slit-lamp examination: The diagnosis of OSSN can be made clinically by detailed evaluation depending on the location- quadrantic, tumor epicenter, extent (conjunctiva, cornea, eyelid, caruncle, sclera, intraocular, orbit), number of clock hours of limbal involvement, maximal tumor basal diameter, a morphologic variant of tumor, associated features of keratin, feeder vessels, intrinsic vascularity, and regional lymphadenopathy. Inspection of all conjunctival surfaces with eversion of the lids by slit-lamp biomicroscopy is mandatory (Table 1).
|
The details of the examination should include:
|
Table 1: Complete examination in a case of ocular surface squamous neoplasia
2. Rose Bengal stain: Rose bengal stain is a quick and inexpensive method that assists in the diagnosis of OSSN. However, as it stains the dead, degenerating and any devitalized tissues, it is not specific for OSSN. (Figure 3A).
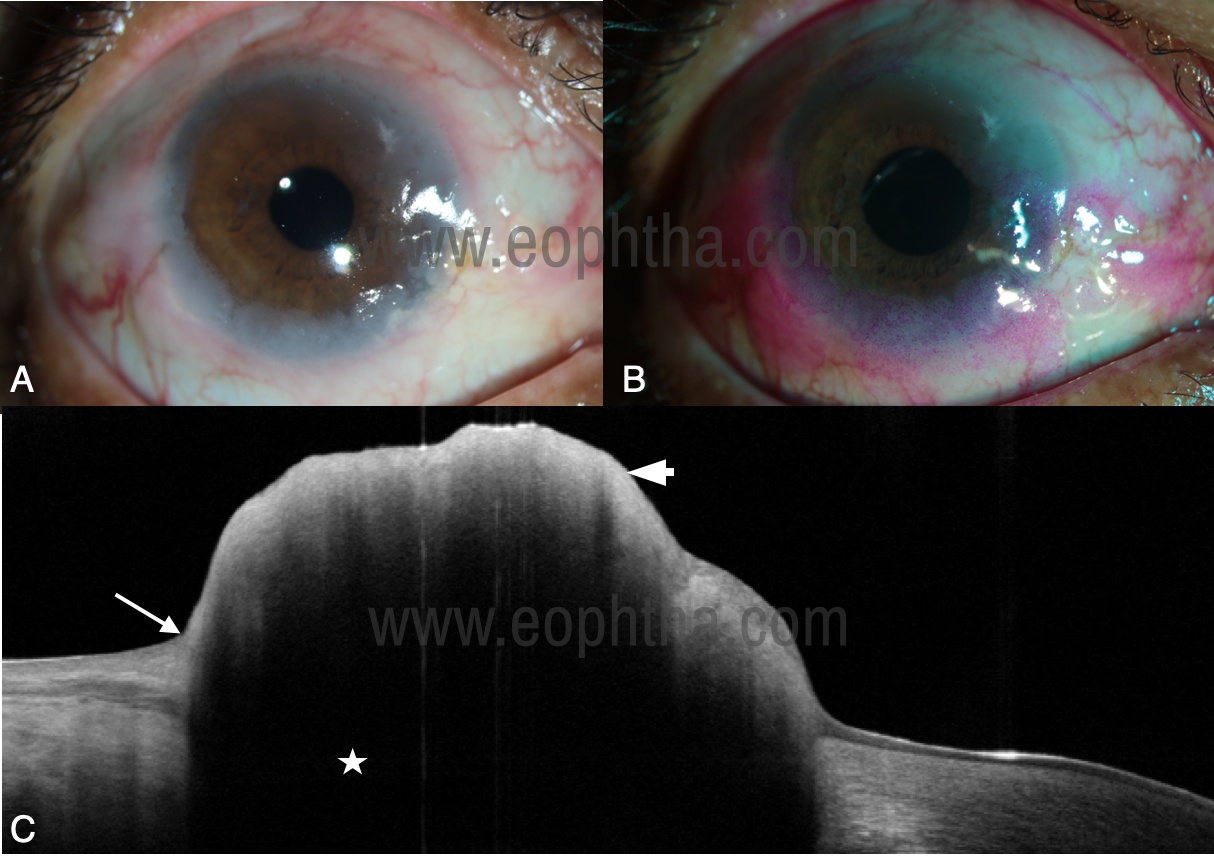
Figure 3: Diagnostic modalities of ocular surface squamous neoplasia (OSSN) A. Diffuse ocular surface OSSN B. The lesion appears more prominent with distinct margins after Rose Bengal stain C. Anterior segment optical coherence tomography of OSSN showing an abrupt transition from normal to the abnormal epithelium (arrow), thickened and hyperreflective epithelium (arrowhead), back shadowing (star).
3. Fluorescein stain: Fluorescein stain is useful to delineate the tumor margins especially on the corneal surface.
4. Anterior segment Optical coherence tomography (AS-OCT): AS-OCT plays a potentially critical role by providing a non-invasive means of diagnosis, follow-up of patients post-treatment, and differentiation of OSSN from other ocular surface diseases mimicking this condition. It acts as an “optical biopsy” for the diagnosis of these lesions in a novel way 36. On ultrahigh-resolution AS-OCT, the characteristic features of OSSN are delineated (Table 2) (Figure 3B). The advantages include
- Diagnosis of the ocular surface squamous neoplasia
- Monitoring the changes in the tumor during the treatment
- Follow-up after completion of the treatment
- For detection of subtle tumor recurrences
- Differentiating OSSN from other ocular surface diseases.
|
AS-OCT features of OSSN:
|
Table 2: Distinctive features of ocular surface squamous neoplasia on ultrahigh-resolution anterior segment optical coherence tomography (AS-OCT)
5. Exfoliative cytology: Exfoliative cytology is used for the cytological characteristic studies by obtaining the sample from one or more appropriate areas with a small cytobrush. It helps in the diagnosis of neoplastic epithelial cells as they have poor cell to cell adherence and tend to desquamate, but the drawbacks include
a) The difficult technique to practice
b) Discomfort to the patients
c) Less reliability on the interpretation of the lesion with problems of cellular overlap
d) It is unable to discern the localization of the lesion or the degree of tumor invasion.
6. Impression cytology: It is a simple, inexpensive, and non-invasive method to diagnose and monitor the disease clinically using cellulose acetate filter paper sheets (CAP) 37-39. It aids in studying the cell to cell relationship, but the drawbacks include
- It cannot grade the epithelial dysplasias
- It cannot assess the micro-invasive growth
7. Confocal microscopy: It is a non-invasive method and can be reliable in the grading of dysplasia which helps in the diagnosis of OSSN and clinical monitoring in response to treatment 40. The disadvantages include
- It is difficult to use
- It has limited field of view
8. Ultrasound biomicroscopy (UBM): It is a non-invasive method that helps in determining the thickness of the lesion and the extent of the intraocular invasion when present. Intraocular extension of the tumor is diagnosed based on the presence of cells in the anterior chamber, gonioscopy, dilated fundus examination, UBM, and ocular USG in cases with media opacity.
9. Orbital imaging: Orbital imaging by computed tomography and magnetic resonance imaging is recommended in cases with forniceal involvement to rule out any orbital extension.
Systemic evaluation is important regarding the immunosuppressive status for further management. All the tumors should be graded according to American Joint Committee Classification (AJCC) based on the status of the tumor, lymph node, and metastasis of the lesion 41.
F. Differential diagnoses
As OSSN includes wide spectrum of clinical variants, it mimics the other ocular surface lesions 42-44. The lesions are listed in Table 3 & 4. (Figure 4)
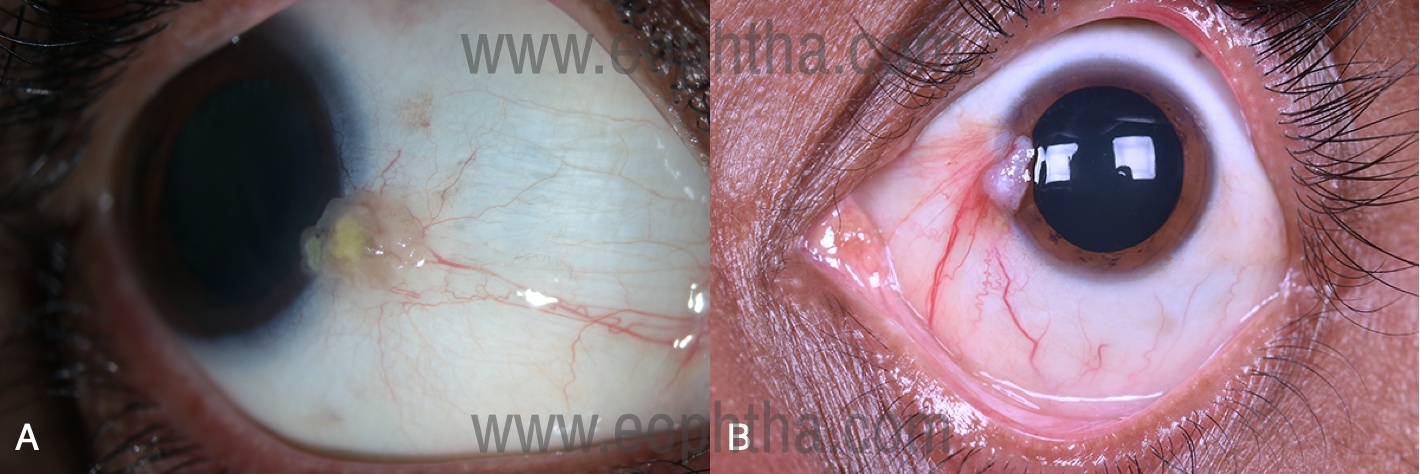
Figure 4: Mimickers of ocular surface squamous neoplasia (OSSN) A. Actinic keratosis of conjunctival epithelium B. Ocular surface squamous neoplasia at the head of the pterygium, a rare coexistence.
|
Differential diagnosis of OSSN:
|
Table 3: Differential diagnoses of ocular surface squamous neoplasia (OSSN)
|
Differential diagnoses |
Salient features |
|
Squamous papilloma |
Sessile or pedunculated with a punctate vascular pattern mimicking the papilliform variant of OSSN |
|
Pseudo epitheliomatous hyperplasia |
The benign reactive inflammatory proliferation of epithelial cells which manifests as an elevated leukoplakic pinkish lesion in the limbal area |
|
Actinic keratosis |
Develops in inter palpebral conjunctiva, often with frothy appearance mimicking conjunctival intraepithelial neoplasia |
|
Pyogenic granuloma |
Vasoproliferative inflammatory lesions composed of granulation tissue, usually following trauma or infection and may mimic OSSN |
|
Conjunctival malignant melanoma |
A pigmented lesion with a regular smooth surface, and lacks gelatinous and keratin components |
Table 4: Salient features of common differential diagnoses of ocular surface squamous neoplasia (OSSN)
G. Treatment
The treatment for OSSN is initiated based on clinical diagnosis. Incisional biopsy of the tumor is indicated only in cases of atypical presentation of OSSN.
The different modalities available for OSSN treatment include
- Wide surgical excision
- Cryotherapy
- Chemotherapy
- Immunotherapy
- Antiviral medications
- Topical or subconjunctival Anti-VEGF
- Radiotherapy
- Photodynamic therapy
- Extended enucleation
- Orbital exenteration
1. Wide excisional biopsy by ‘‘no-touch’’ technique:
The standard modality for the treatment of OSSN is wide surgical excision by “no‑touch” technique and adjunctive cryotherapy. The following are the principle steps of the surgery:
i) Wide excision with 4-mm margins for conjunctival/limbal component
ii) Alcohol keratoepitheliectomy with 2-mm margins for corneal component followed by
iii) Double freeze-thaw cryotherapy for surgical margins
iv) Hemostasis and
v) Amniotic membrane graft (AMG) or conjunctival autograft to cover the defect or direct conjunctival closure depending on the size of the ocular surface defect.
The excised tissue is then sent for histopathological examination. The further management depends on the histopathology of the margins and the base of the lesion.
a. If the surgical margin is positive for atypical cells:
Mild to moderate Dysplasia
- Observation unless patient is immunosuppressive
Severe Dysplasia/ CIN/ SCC
- Adjuvant chemotherapy
- Immunotherapy
- Repeat margin resection by 2mm
b. If Base is positive for atypical cells:
- Plaque brachytherapy
Simple Limbal Epithelial Transplantation (SLET)
During wide excision of OSSN, corneoscleral limbal dissection of 6 clock hours or more can cause limbal stem cell deficiency (LSCD). LSCD can occur in cases of OSSN owing to direct damage to the limbal stem cells by the
- Tumor (replaces normal limbal cells with neoplastic cells), or
- Iatrogenic damage owing to surgery involving dissection of the limbus or
- Cryotherapy induced damage.
LSCD manifests in the postoperative period as pseudopterygium extending onto the cornea or pannus formation within 2 months.
The conservative treatment strategies for LSCD include:
a. Intensive Lubrication,
b. Bandage contact lens, and
c. Debridement of conjunctival epithelium over the cornea.
The surgical treatment of LSCD includes:
a. Conjunctival-limbal autografting,
b. Keratolimbal autografting,
c. Ex vivo cultivated limbal epithelial transplantation (CLET), and
d. Simple limbal epithelial transplantation (SLET)
SLET is popular now in partial and total LSCD. Concomitant SLET after surgical excision of OSSN prevents LSCD in cases requiring extensive corneoscleral limbal dissection.
The procedure of SLET:
Limbal tissue is obtained from healthy limbus from the ipsilateral or contralateral eye. Conjucntivolimbal-corneal epithelial defect is reconstructed with amniotic membrane graft (AMG) and the donor limbal tissue is cut into small pieces. Limbal tissue explants are placed in the perilimbal tissue over the AMG and secured with fibrin glue. A bandage contact lens (BCL) is placed over the cornea and limbal tissue explants. BCL is then removed after 1 week 45, 46.
2. Immunotherapy
In 1994, Maskin published the first case of topical Interferon alpha 2b (INF α2b) for a multifocal limbal carcinoma in situ (CIN). Later, Karp et al popularized the use of INF α2b for OSSN. Since then, most investigations showed favorable results with varying doses of INF α2b for conjunctival and corneal CIN.
INF α2b is a type 1 interferon consisting of 165 amino acid residues with arginine in position 23. This glycoprotein is produced by recombinant DNA technology and resembles interferon secreted by leukocytes. It exhibits antineoplastic and antiviral effects. In solid tumors, INF α causes prolongation of the cell cycle time of malignant cells, inhibits biosynthetic enzymes and apoptosis, interacts with other cytokines, and increases the immunomodulatory and antiangiogenic effects.
The mechanism of action of INF α2b in OSSN is unclear but may include inhibition of angiogenesis and/or inhibition of human papilloma virus replication. However, recent studies have shown that the presence of human papilloma virus is not required for a favorable response with INF α2b. The US Food and Drug Administration has approved INF α2b for the treatment of AIDS-related Kaposi sarcoma, hairy cell leukemia, malignant melanoma, aggressive follicular non-Hodgkins lymphoma, chronic hepatitis B and C, and condyloma acuminata. INF α2b has been used off-label in the treatment of OSSN since the first publication in 1994. Good response to treatment with complete tumor regression is achieved in 85% to 100% OSSN cases with INF α2b 47-54.
Indications:
INF α2b is used for
- Immunoreduction (to reduce the tumor size) or
- Immunotherapy (as sole treatment for tumor regression) or
- Immunoprevention (to prevent tumor recurrence in those with histopathology evidence of residual tumor at margins post-excisional biopsy).
Dosage:
1. Corneal OSSN: Topical INF α2b eye drops (1 MIU/cc) 4 times/day for immunoreaction/immunotherapy.
2. Conjunctival or conjunctivo-limbal-corneal lesions- combination of topical INF α2b eye drops (1 MIU/cc) 4 times/day and perilesional INF α2b injection (3 to 10 MIU/cc) once a month for immunoreduction/immunotherapy.
3. Positive surgical margins on histopathology: Topical INF α2b eye drops (1 MIU/cc) 4 times/day for immunoprevention.
Procedure for Topical administration of INF α2b:
Topical drops are prepared under sterile conditions and instructed to store the drug in a refrigerator (20 to 80c) and advised to apply one drop 4 times/day.
The procedure of subconjunctival injection:
1. Instill 0.5% topical proparacaine 5 minutes before the procedure.
2. A subconjunctival injection of a portion of 3 to 10 MIU/ml of recombinant INF α2b in a 1-ml prefilled syringe is performed. The needle entry is immediately adjacent to the tumor base through normal conjunctiva and directed toward the tumor, remaining below the mass without entry into the tumor.
3. Note the ballooning of the lesion and the surrounding conjunctiva after injection.
4. The total amount of INF α2b depends on the location (bulbar conjunctiva versus tarsal conjunctiva) and the total surface area of the tumor.
Side effects:
i) Flu-like symptoms with fever/ Myalgia
ii) Follicular conjunctivitis
iii) Superficial punctate keratitis
Follow-up:
During the treatment with INF α2b, once a month follow-up is recommended since the topical medications should be freshly prepared and dispensed to the patient; and the injection should be given monthly till the desired response is achieved. Tumor details should be recorded during each visit. If the patient has a residual tumor, continue topical medication until complete tumor regression, and 3 months beyond complete tumor regression. All patients receiving INF α2b as immunoprevention are advised 3 cycles of topical INF α2b eye drops. After complete tumor regression, the patients are reviewed once in 3 months in the first year, and every 4 months in the second year.
Incomplete response:
If there are significant residua that are seen after 3 months of use of topical and/or injection INF α2b, an alternate therapy is offered to the patient.
3. Chemotherapy
Mitomycin C (MMC) and 5-Flurouracil (5-FU) are the most commonly used chemotherapeutic agents in OSSN treatment.
a. Mitomycin C: MMC is a DNA alkylating agent and disrupts the production of RNA by inhibiting the mitosis. It is an antimetabolite isolated from Streptococcus caespitosus. MMC is used in concentrations of 0.02% or 0.04%. The efficacy rate of MMC ranges from 80% to 100%. In general, patients may need a total of 3 cycles for the tumor to resolve 55.
Indications:
i) Primary therapy
ii) Tumor recurrences
iii) Adjuvant postoperative therapy for positive margins
Dosage:
Topical MMC is administered 4 times a day (4 days on and 3 days off) for 4 weeks followed by 2 weeks drug holiday to complete one cycle of treatment.
Side effects:
1) Epithelial surface toxicity: Conjunctival hyperemia, corneal punctate erosion
2) Limbal stem cell deficiency
3) Punctal stenosis
4) Blepharospasm
b. 5-Flurouracil: 5-FU is a pyrimidine analog of the purine base uracil that inhibits the enzyme thymidine synthase, and thus impairs DNA and RNA synthesis resulting in inhibition of proliferation of cancer cells. 5-FU is used in the concentration of 1%. The efficacy rate of 5-FU is 85% to 100%, but the long-term efficacy of this drug is not yet established. In general, patients may need a total of 4 to 5 cycles for the tumor to resolve completely 56-58.
Dosage:
Topical 5-Flurouracil (5-FU 1%) is administered 4 times daily for 1 week, followed by 3 weeks off.
Side effects
1) Transient lid edema and erythema
2) Conjunctival hyperemia
3) Superficial keratitis,
4) Filamentary keratitis and
5) Superficial stromal melting, rarely
4. Antiviral drugs
Cidofovir is a monophosphate nucleotide analog that impairs DNA synthesis.
Dosage:
Topical cidofovir (2.5 mg/ml) is administered 3 times daily followed by 1 week after the tumor regression.
Side effects:
1) Conjunctival erythema
2) Punctal stenosis
5. Topical or sub-conjunctival anti-VEGF
Topical and subconjunctival injections of anti-vascular endothelial growth factor (VEGF) are efficacious in the reduction of the size and vascularity of OSSN, but there is no complete disappearance of the tumor. Bevacizumab and Ranibizumab are the anti-VEGF’s that have been used for OSSN treatment 59.
6. Retinoic acid
Retinoic acid, a synthetic analog of vitamin A, plays a role in cellular growth and differentiation of epithelial cells used in combination with interferon for the OSSN treatment.
7. Radiotherapy
In selected cases of invasive disease of OSSN, plaque brachytherapy or proton-beam radiotherapy can be used in an attempt to salvage the eye.
a. Plaque brachytherapy: Strontium 90, Ruthenium 106, Iodine 125 are the common radioactive materials used for plaque brachytherapy.
Indication:
Adjuvant postoperative therapy for the positive base of the tumor
Dosage:
Strontium 90: 20 to 180 Gy to the tumor surface
Ruthenium 106 and Iodine 125: 40 to 65 Gy to the tumor bed
Complications:
1) Post irradiation conjunctivitis
2) Dry eye
3) Symblepharon
4) Corneal perforation
5) Cataract
6) Scleral ulceration
b. External beam radiotherapy (EBRT)
External beam radiotherapy is limited to the recurrent lesions extending to the orbit. It is rarely used as a primary treatment and is usually used as an adjunctive treatment.
8. Enucleation and orbital exenteration:
Enucleation is performed in cases with the intraocular extension of OSSN or in cases of extensive OSSN not amenable to excisional biopsy. Orbital exenteration may be needed in cases with orbital tumor extension or diffuse conjunctival OSSN not amenable for enucleation 60, 61. (Figure 5).
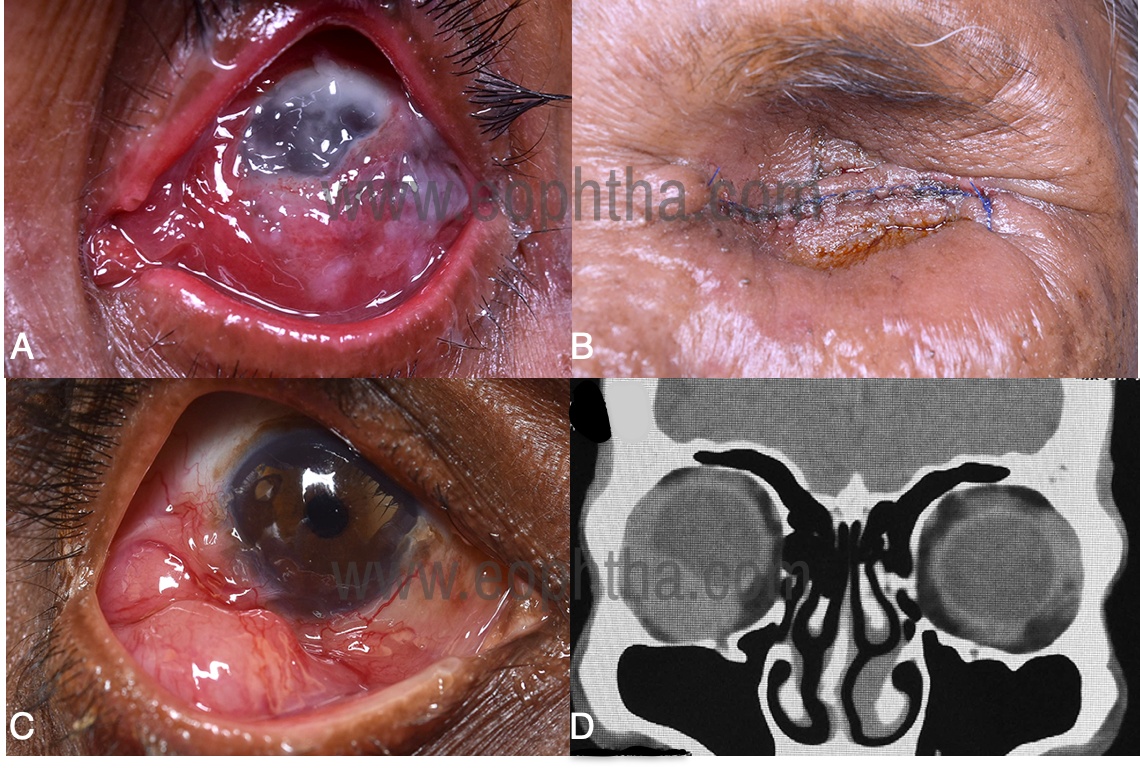
Figure 5: Extensive ocular surface squamous neoplasia (OSSN) A. A 71-year-old female with diffuse conjunctival congestion with a gelatinous lesion involving the left eye along with intraocular tumor extension B. The patient underwent eyelid-sparing orbital exenteration. C. A 60-year-old male presented with a large nodular OSSN in the lateral and inferior quadrant of the right eye D. Computed tomography of the orbit revealed a homogenous isodense mass in the lateral and inferior quadrant of anterior and mid-orbit causing superomedial displacement of the globe, suggestive of orbital tumor extension.
H. Histopathology of OSSN
1. Dysplasia
Dysplastic lesions exhibit mild, moderate, or severe degrees of cellular atypia that may involve various thicknesses of the epithelium, starting from the basal layer outwards. They show the modification of epithelial cell organization with various degrees of loss of the normal cellular polarity. Usually, the most superficial layers are uninvolved. In cases with severe dysplastic changes, it may be difficult to distinguish the lesion from carcinoma in situ 61, 63.
a. Mild dysplasia: atypical cells occupying the lower 1/3rd of the epithelium
b. Moderate dysplasia: atypical cells extending to the middle 1/3 of the epithelium
c. Severe dysplasia: atypical cells involving the near full thickness of the epithelium
2. Carcinoma in situ (CIN)
CIN may exhibit all the histological features similar to Squamous cell carcinoma. However, it usually remains confined to the epithelium, respecting the basement membrane. CIN usually shows a total loss of normal cellular maturation, affecting the full thickness of the epithelium. The cells are large and usually elongated. Keratinized cells may be identified and mitotic figures can be present in all layers 64-67.
3. Invasive Squamous Cell Carcinoma (SCC)
Invasive SCC shows features similar to CIN, but the basement membrane of the epithelium is breached and the subepithelial tissue of the conjunctiva is invaded. Most of the conjunctival SCC’s are well-differentiated with surface keratinization and various degrees of cellular pleomorphism. These lesions show hyperplastic and hyperchromatic cells, dyskeratosis, keratin pearls, loss of cellular cohesiveness, and atypical mitotic figures. In pigmented OSSN, the pigmentation owing to abnormal proliferation of melanocytes in the lesions are noted.
There are 3 types of invasive conjunctival SCC with rather aggressive behavior. Because of the aggressiveness of these variants, which often invade the eyeball and the orbital tissue, and even metastasize to lymphatics and distant sites, they should be histopathologically differentiated from less aggressive conventional SCC 68-82.
1. Spindle cell variant exhibits spindle shaped cells that may be difficult to distinguish from fibroblasts.
2. Adenoid (Aggressive) variant is characterized by extracellular hyaluronic acid but no intracellular mucin.
3. Mucoepidermoid variant contains squamous and mucus-secreting cells (stained positively with stains for MPS).
Corneal OSSN
The origin of corneal OSSN is controversial which could be the possible potential of the corneal epithelium to undergo dysplastic and cancerous changes, or the origin of corneal OSSN is at the limbus. Histologically, the corneal OSSN is similar to those in the limbus and conjunctiva. Usually, Bowman’s layer is intact and has a tendency to recur because of inadequate scraping, but with current methods of treatment, this rarely occurs 83, 84.
I. Prognosis
The overall prognosis in OSSN is good with little tendency to metastasize and a low mortality rate. Modern treatment strategies are effective with local recurrence rates reported to be 5% and regional lymph node metastasis at <2%. Aggressive variants like muco-epidermoid and spindle cell carcinoma and OSSN in immunocompromised patients have a worse prognosis 85-88.
References
- Lee G.A., Hirst L.W. Ocular surface squamous neoplasia. Surv Ophthalmol. 1995;39:429–450.
- Pizzarello L.D., Jakobiec F.A. Bowen’s disease of the conjunctiva: a misomer. In: Jakobiec F.A., editor. Ocular adnexal tumors. Aesculapius; Birmingham, AL: 1978. pp. 553–571.
- Honavar SG. Ocular surface squamous neoplasia: Are we calling a spade a spade? Indian J Ophthalmol 2015;65:907-9.
- Shields J.A., Shields C.L. 2nd ed. LWW press; Philadelphia: 2008. Eyelid, conjunctival and orbital tumors. (An atlas and text book).
- Karcioglu Z.A., Wagoner M.D. Demographics, etiology, and behavior of conjunctival squamous cell carcinoma in the 21st century. Ophthalmology. 2009;116:2045–2046.
- Lee G.A., Hirst L.W. Incidence of ocular surface epithelial dysplasia in metropolitan Brisbane. A 10-year survey. Arch Ophthalmol. 1992;119:525–527.
- Sun E.C., Fears T.R., Goedert J.J. Epidemiology of squamous cell conjunctival cancer. Cancer Epidemiol Biomarkers Prev. 1997;6:73–77.
- Templeton A.C. Tumors of the eye and adnexa in Africans in Uganda. Cancer. 1967;20:1689–1698.
- Karcioglu Z.A., Wagoner M.D. Demographics, etiology, and behavior of conjunctival squamous cell carcinoma in the 21st century. Ophthalmology. 2009;116:2045–2046.
- Armstrong B.K., Kricker A. The epidemiology of UV induced skin cancer. J Photochem Photobiol. 2001;63:8–18.
- Ng J., Coroneo M.T., Wakefield D., Di Girolamo N. Ultraviolet radiation and the role of matrix metalloproteinases in the pathogenesis of ocular surface squamous neoplasia. Invest Ophthalmol Vis Sci. 2008;49:5295–5306.
- Jacyk W.K. Xeroderma pigmentosum in black South Africans. Int J Dermatol. 1999;38:511–514.
- Hertle R.W., Durso F., Metzler J.P. Epibulbar squamous cell carcinomas in brothers with xeroderma pigmentosa. J Pediatr Ophthalmol Strabis-mus. 1991;28:350–353.
- Brooks B.P., Thompson A.H., Bishop R.J., Clayton J.A., Chan C.C., Tsilou E.T. Ocular manifestations of xeroderma pigmentosum. Long-term follow-up highlights the role of DNA repair in protection from sun damage. Ophthalmology. 2013.
- Robbins, Cotran . 7th ed. Saunders; Philadelphia: 2004. Neoplasia. Pathologic basis of disease.
- Manderwad G.P., Kannabiran C., Honavar S.G., Vemuganti G.K. Lack of association of high-risk human papillomavirus in ocular surface squamous neoplasia in India. Arch Pathol Lab Med. 2009;133:1246–1250.
- Koss L.G. Cytologic and histologic manifestations of human papillomavirus infection of the female genital tract and their clinical significance. Cancer. 1987;60:1942–1950.
- Guthoff R., Marx A., Stroebel P. No evidence for a pathogenic role of human papillomavirus infection in ocular surface squamous neoplasia in Germany. Curr Eye Res. 2009;34:666–671.
- Eng H.L., Lin T.M., Chen S.Y. Failure to detect human papillomavirus DNA in malignant epithelial neoplasms of conjunctiva by polymerase chain reaction. Am J Clin Pathol. 2002;117:429–436.
- Scott I.U., Karp C.L., Nuovo G.J. Human papillomavirus 16 and 18 expression in conjunctival intraepithelial neoplasia. Ophthalmology. 2002;109:542–547.
- Chauhan S., Sen S., Sharma A., Dar L., Kashyap S., Kumar P. Human papillomavirus: a predictor of better survival in ocular surface squamous neoplasia patients. Br J Ophthalmol. 2012;96:1517–1521.
- Thomas J.O. Acquired immunodeficiency syndrome-associated cancers in Sub-Saharan Africa. Semin Oncol. 2001;28:198–206.
- Weinstein J.E., Karp C.L. Ocular surface neoplasias and human immunodeficiency virus infection. Curr Opin Infect Dis. 2013;26:58–65.
- Spitzer M.S., Batumba N.H., Chirambo T. Ocular surface squamous neoplasia as the first apparent manifestation of HIV infection in Malawi. Clin Experiment Ophthalmol. 2008;36:422–425.
- Guech-Ongey M., Engels E.A., Goedert J.J., Biggar R.J., Mbulaiteye S.M. Elevated risk for squamous cell carcinoma of the conjunctiva among adults with AIDS in the United States. Int J Cancer. 2008;122:2590–2593.
- Pradeep T.G., Gangasagara S.B., Subbaramaiah G.B. Prevalence of undiagnosed HIV infection in patients with ocular surface squamous neoplasia in a tertiary center in Karnataka South India. Cornea. 2012;31:1282–1284.
- Shields C.L., Ramasubramanian A., Mellen P.L., Shields J.A. Conjunctival squamous cell carcinoma arising in immunosuppressed patients (organ transplant, human immunodeficiency virus infection) Ophthalmology. 2011;118:2133–2137.
- Honavar SG, Manjandavida FP. Tumors of the ocular surface: A review. Indian J Ophthalmol 2015;63:187- 203.
- Dandala PP, Malladi P, Kavitha. Ocular Surface Squamous Neoplasia (OSSN): A Retrospective Study. Journal of Clinical and Diagnostic Research 2015;9:10-3.
- Viswamithra P, Bhaskara N. Ocular surface squamous neoplasia. J NTR Univ Health Sci 2014;3:185-8.
- Cicinelli MV, Marchese A, Bandello F, Modorati G. Clinical Management of Ocular Surface Squamous Neoplasia: A Review of the Current Evidence Ophthalmol Ther 2018;7:247–62.
- Meel R, Dhiman R, Vanathi M, Pushker N, Tandon R, Devi S. Clinicodemographic profile and treatment outcome in patients of ocular surface squamous neoplasia. Indian J Ophthalmol 2017;65:936-41.
- Krishnaraj J, Das SS, Vendhan KE. Ocular surface squamous neoplasia (OSSN). International Journal of Ocular Oncology and Oculoplasty 2016;2:19-30.
- Shields C.L., Manchandia A., Subbiah R., Eagle R.C., Jr., Shields J.A. Pigmented squamous cell carcinoma in situ of the conjunctiva in 5 cases. Ophthalmology. 2008;115:1673–1678.
- Basti S., Macsai M.S. Ocular surface squamous neoplasia: a review. Cornea. 2003;22:687–704.
- Kieval J.Z., Karp C.L., AbouShousha M., Galor A., Hoffman R.A., Dubovy S.R. Ultra-high resolution optical coherence tomography for differentiation of ocular surface squamous neoplasia and pterygia. Ophthalmology. 2012 Mar;119(3):481–486.
- Gelender H., Forster R.K. Papanicolaou cytology in the diagnosis and management of external ocular tumors. Arch Ophthalmol. 1980;98:909–912.
- Nolan G.R., Hirst L.W., Wright R.G. Application of impression cytology to the diagnosis of conjunctival neoplasms. Diag Cytopathol. 1994;11:246–249.
- Tole D.M., McKelvie P.A., Daniell M. Reliability of impression cytology for the diagnosis of ocular surface squamous neoplasia employing the Biopore membrane. Br J Ophthalmol. 2001 Feb;85(2):154–158.
- Xu Y., Zhou Z., Xu Y., Wang M., Liu F., Qu H. The clinical value of in vivo confocal microscopy for diagnosis of ocular surface squamous neoplasia. Eye. 2012 Jun;26(6):781–787.
- Ibrahim O, Sayed-Ahmed, Palioura S, Galor A, Carol L. Karp. Diagnosis and Medical Management of Ocular Surface Squamous Neoplasia.Expert Rev Ophthalmol 2017;12:11–19.
- Wagner R.F., Jr. Grande DJ. Pseudo epitheliomatous hyperplasia vs. Squamous cell carcinoma. J Dermatol Surg Oncol. 1986;12:632.
- Winer L.H. Pseudoepitheliomatous hyperplasia. Arch Dermatol Syph. 1940;42:856.
- Mittal R., Meena M., Saha D. Actinic granuloma of the conjunctiva in young women. Ophthalmology. 2013 Apr 16.
- Kaliki S, Ali Mohammad F, Tahiliani P, Sangwan V. Concomitant Simple Limbal Epithelial Transplantation After Surgical Excision of Ocular Surface Squamous Neoplasia. Am J Ophthalmol 2017;174:68–75.
- Walia AS, Kumar S, Srivastava B, Bhaisare V, Sharma V, Agarwal D et.al. Treatment of ocular surface squamous neoplasia (ossn) with surgical excision & adjunctive topical mitomycin c therapy.National Journal of Medical and Dental Research. 2016;4:324-8.
- Kaliki S, Bejjanki KM, Desai A, Mohammed A. Interferon Alfa 2b for Ocular Surface Squamous Neoplasia: Factors Influencing the Treatment Response. Seminars in Ophthalmology 2019;(7-8):1-8.
- Kaliki S, Sharma A, Vempuluru V. Interferon Alfa-2b for Pigmented Ocular Surface Squamous Neoplasia: A Report of 8 Lesions. Cornea 2020; (1).
- Shields CL, Kaliki S, Kim HJ, et al. Interferon for ocular surface squamous neoplasia in 81 cases: outcomes based on the American Joint Committee on Cancer classification. Cornea 2013;32(3):248-56.
- Kaliki S, Singh S, Iram S, Tripuraneni D. Recombinant interferon alpha 2b for ocular surface squamous neoplasia: An efficient and cost-effective treatment modality in Asian Indian patients. Indian J Ophthalmol 2016;64(10):702-709.
- Shah SU, Kaliki S, Kim HJ, Lally SE, Shields JA, Shields CL. Topical interferon alfa-2b for management of ocular surface squamous neoplasia in 23 cases: outcomes based on American Joint Committee on Cancer classification. Arch Ophthalmol 2012;130(2):159-64.
- Kim H.J., Shields C.L., Shah S.U., Kaliki S., Lally S.E. Giant ocular surface squamous neoplasia managed with interferon alpha-2b as immunotherapy or immunoreduction. Ophthalmology. 2012;119:938–944.
- Maskin S.L. Regression of limbal epithelial dysplasia with topical interferon [letter] Arch Ophthalmol. 1994;112:1145–1146.
- Karp C.L., Moore J.K., Rosa R.H., Jr. Treatment of conjunctival and corneal intraepithelial neoplasia with topical interferon alpha-2b. Ophthalmology. 2001;108:1093–1098.
- Shields C.L., Demirci H., Marr B.P. Chemoreduction with topical mitomycin C prior to resection of extensive squamous cell carcinoma of the conjunctiva. Arch Ophthalmol. 2005;123:109–113.
- Parrozzani R., Lazzarini D., Alemany-Rubio E. Topical 1% 5-fluorouracil in ocular surface squamous neoplasia: a long-term safety study. Br J Ophthalmol. 2011;95:355–359.
- Parrozzani R, Frizziero L, Trainiti S, et al. Topical 1% 5-fluoruracil as a sole treatment of corneoconjunctival ocular surface squamous neoplasia: long-term study. Br J Ophthalmol 2017;101(8):1094-1099.
- Venkateswaran N, Mercado C, Galor A, and Caroll karp. Comparison of Topical 5-Fluorouracil and Interferon Alfa-2b as Primary Treatment Modalities for Ocular Surface Squamous Neoplasia. Am J Ophthalmol 2019;199:216–22.
- Asena L, Dursun Altýnörs D. Topical Bevacizumab for the Treatment of Ocular Surface Squamous Neoplasia. J Ocul Pharmacol Ther. 2015;31:487–90.
- Oellers P., Karp C.L., Sheth A., Kao A.A., Abdelaziz A., Matthews J.L., Dubovy S.R., Galor A. Prevalence, treatment, and outcomes of coexistent ocular surface squamous neoplasia and pterygium. Ophthalmology. 2013;120:445–450.
- Shields J.A., Shields C.L., Gunduz K. The 1998 pan American lecture. Intraocular invasion of conjunctival squamous cell carcinoma in five patients. Ophthal Plast Reconstr Surg. 1999;15:153–160.
- Lewis J.S., Ritter J.H., El-Mofty S. Alternative epithelial markers in sarcomatoid carcinomas of the head and neck, lung, and bladder-p63, MOC-31, and TTF-1. Mod Pathol. 2005;18:1471–1481.
- Font R.L., Croxatto J.O., Rao N.A., editors. AFIP atlas of tumor pathology. ARP press; Washington, DC: 2006. Tumors of the conjunctiva and caruncle. (Series 4. Tumors of the eye and ocular adnexa).
- Wells J.R., Randleman J.B., Grossniklaus H.E. Clear cell carcinoma of the conjunctiva. Cornea. 2011;30:95–96.
- Margo C.E., Groden L.R. Primary clear cell carcinoma of the conjunctiva. Arch Ophthalmol. 2008;126:436–438.
- Connor D.H., Taylor H.B., Helwig E.B. Cutaneous metastasis of renal cell carcinoma. Arch Pathol. 1963;76:339–346.
- Cervantes G., Rodríguez A.A., Jr., Leal A.G. Squamous cell carcinoma of the conjunctiva: clinicopathological features in 287 cases. Can J Ophthalmol. 2002;37:14–19.
- Robinson J.W., Brownstein S., Jordan D.R., Hodge W.G. Conjunctival mucoepidermoid carcinoma in a patient with ocular cicatricial pemphigoid and a review of the literature. Surv Ophthalmol. 2006;51:513–519.
- Hwang I.P., Jordan D.R., Brownstein S., Gilberg S.M., McEachren T.M., Prokopetz R. Mucoepidermoid carcinoma of the conjunctiva: a series of three cases. Ophthalmology. 2000;107:801–805.
- Manderwad G.P., Gokul G., Kannabiran C., Honavar S.G., Khosla S., Vemuganti G.K. Hypomethylation of the DNMT3L promoter in ocular surface squamous neoplasia. Arch Pathol Lab Med. 2010;134:1193–1196.
- Cardesa A., Zidar N. Spindle cell carcinoma. In: Barnes L., Eveson J.W., Reichart P., Sidransky D., editors. World Health Organization classification of tumors. Pathology and genetics of head and neck tumours. IARC press; Lyon: 2005.
- Barnes L., Brandwein M., Som P.M. 2nd ed. Marcel Dekker; 2001. Surgical pathology of the head and neck.
- Ni C., Searl S.S., Kriegstein H.J., Wu B.F. Epibulbar carcinoma. Int Ophthalmol Clin. 1982;22:1–33.
- Iliff W.J., Marback R., Green W.R. Invasive squamous cell carcinoma of the conjunctiva. Arch Ophthalmol. 1975;93:119–122.
- Shields J.A., Eagle R.C., Marr B.P., Shields C.L., Grossniklaus H.E., Stulting R.D. Invasive spindle cell carcinoma of the conjunctiva managed by full-thickness eye wall resection. Cornea. 2007;26:1014–1016.
- Mittal R, Rath S, Vemuganti GK. Ocular surface squamous neoplasia - Review of etio- pathogenesis and an update on clinico-pathological diagnosis. Saudi J Ophthalmol. 2013;27:177-86.
- Xu Z, Taylor JA. Genome-wide age-related DNA methylation changes in blood and other tissues relate to histone modification, expression and cancer. Carcinogenesis 2014;35:356-64.
- Chauhan S, Sen S, Sharma A, Kashyap S, Tandon R, Bajaj MS et al. p16INK4a overexpression as a predictor of survival in ocular surface squamous neoplasia. Br J Ophthalmol 2018;102:840–7.
- Mishra DK, Veena U, Kaliki S, Kethiri AR, Sangwan VS, Ali MH. Differential Expression of Stem Cell Markers in Ocular Surface Squamous Neoplasia. PLoS ONE 2016;11:e0161800.
- Kao A.A., Galor A., Karp C.L., Abdelaziz A., Feuer W.J., Dubovy S.R. Clinicopathologic correlation of ocular surface squamous neoplasms at Bascom Palmer Eye Institute: 2001–2010. Ophthalmology. 2012;119:1773–1776.
- Newton R. A review of the etiology of squamous cell carcinoma of the conjunctiva. Br J Cancer. 1996;74:1511–1513.
- Roy A., Rath S., Das S., Vemuganti G.K., Parulkar G. Penetrating sclerokeratoplasty in massive recurrent invasive squamous cell carcinoma. Ophthal Plast Reconstr Surg. 2011;27:39–41.
- Panda A., Sharma N., Sen S. Massive corneal and conjunctival squamous cell carcinoma. Ophthalmic Surg Lasers. 2000;31:71–72.
- Rath S., Honavar S.G., Naik M.N., Gupta R., Reddy V.A., Vemuganti G.K. Evisceration in unsuspected intraocular tumors. Arch Ophthalmol. 2010;128(3):372–379.
- Mauriello A., Abdelsalam I., McLean J. Adenoid squamous carcinoma of the conjunctiva—a clinicopathological study of 14cases. Br J Ophthalmol. 1997;81:1001–1005.
- Tabin G, Levin S, Snibson G, Loughnan M, Taylor H. Late recurrences and the necessity for long-term follow-up in corneal and conjunctival intraepithelial neoplasia. Ophthalmology. 1997;104(3):485–92.
- McKelvie PA, Daniell M, McNab A, Loughnan M, Santamaria JD. Squamous cell carcinoma of the conjunctiva: a series of 26 cases. Br J Ophthalmol. 2002;86(2):168–73.
- Cervantes G, Rodriguez AA Jr, Leal AG. Squamous cell carcinoma of the conjunctiva: clinicopathological features in 287 cases. Can J Ophthalmol. 2002;37(1):14–9 (Discussion 19–20).