
A 60-year male presented with C/O diminution of vision in the Right Eye. The patient is not a known case of any known systemic illness, although gives a vague c/o chest pain and the occasional headache.Examination revealed a vision of 4/60 with an IOP of 16mmHg as measured by GAT. The right Eye reveals the unremarkable anterior segment with minimal lenticular changes. Vitreous cavity quiet with fundus as shown. The left eye reveals a normal anterior and posterior segment.
Question
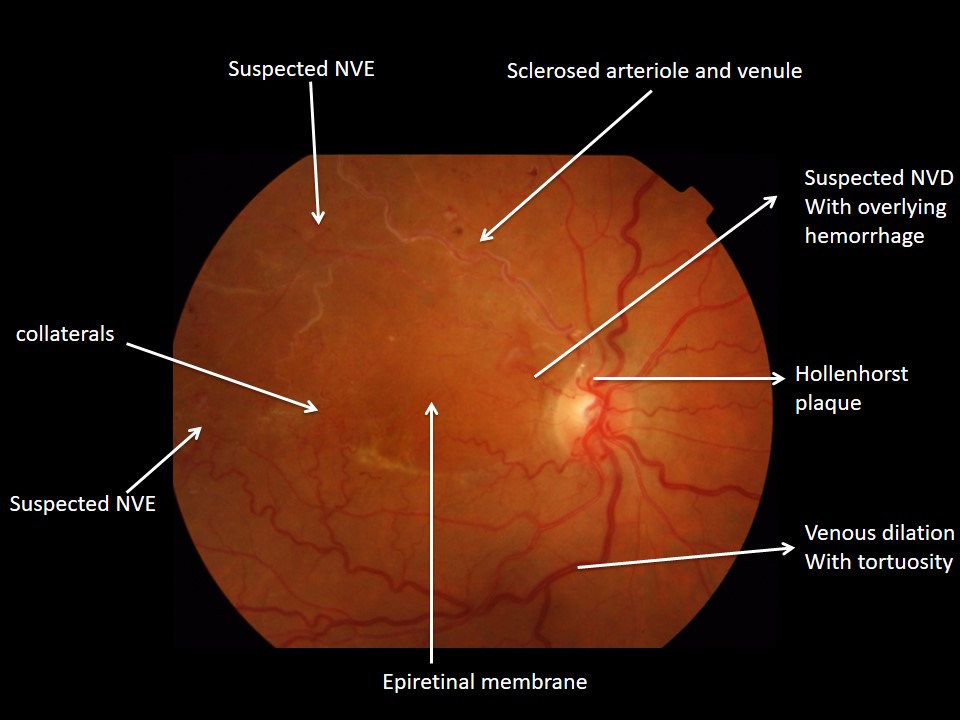
- What are the positive findings as depicted in the fundus photo.?
- What are the investigations you would ask for?
- How will you manage this case?


Answer
Ocular
1) FUNDUS FLUORESCEIN ANGIOGRAM:disruption of retinal layers. These in turn will again help in educating the patient in terms of visual gain he is expected to gain In this case if one had to choose between FFA and OCT, FFA would be a better option.
Management
Managing this case is again in collaboration with a physician/ cardiologist
Ocular
1) After confirming the NVE, NVD on FFA, Laser would be the treatment of choice.
a) Which laser: 532 green laser is the laser of choice
b)Where to hit: laser is given to the entire retina at least 2 disc areas away from NVE. The laser should be given in 2-3 sittings. Remember DO NOT LASER THE COLLATERALS.
c) After completing the entire laser patient needs to be followed up after 2-3 months to assess the involution of NV. The need for an additional laser will depend on subsequent follow-up.
2) Role of anti-VEGF. There is no role INITIALLY for anti-VEGF. Only when the entire laser is over and if the neovascularization persists, one can think of antiVEGF
Another scenario of using antiVGF is when the OCT shows e/o of gross macular edema. In that scenario, an antiVEGF can be combined with Laser.
3) Role of Surgery.
Again no role for surgery initially.
Only if the epiretinal membrane increases significantly or if at some point a tractional retinal detachment occurs, surgery can be contemplated.
Non-Ocular
Since this patient gives a vague complaint of chest pain, and the retina shows evidence of vascular occlusion a systemic workup is imperative.
First and foremost check his blood pressure.
1) Basic hematological investigations consisting of Hemoglobin, ESR, fasting and postprandial glycemic index, lipid profile, renal function tests are essential.
2) A referral to a cardiologist is very important in this case to rule out any systemic pathology specially requesting a carotid doppler.