

1. Embryology
Understanding the embryological development of the cornea helps us appreciate the reasons for a Descemet's membrane (DM) detachment during surgery.
After the lens vesicle separates from the surface epithelium, a wave of mesenchyme forms the primary corneal stroma. A second wave then forms the endothelium, which secretes the DM. The DM, hence, has a potential plane of separation from the corneal stroma, which we use to our benefit in DMEK surgery and which works against us in an inadvertent DM detachment.
Throughout the life of an individual, the DM thickens as the posterior non-banded layer is secreted by the endothelium. The anterior fetal banded layer tends to remain the same. However, in most instances, the separation happens between the DM and the cornea stroma1.
The thickness of the DM varies between 10 and 15 microns, increasing with age. DM does not regenerate after any damage2.
2. Cataract Surgery and DM Detachment
A post-cataract DM detachment occurs in 0.26% of extracapsular cataract extraction surgeries, 0.1% of manual small incision cataract surgeries, and 0.04% of phacoemulsification procedures3.
The DM detachment can occur at any stage of surgery, often while introducing instruments into the eye, or when hydrating the wounds at the end of the procedure. It is especially common in eyes with a dense arcus and shagreen, with endothelial disease, and is often bilateral - leading to speculation that some patients may be predisposed to this complication. Such corneas, with peripheral thickening and Hassal Henle bodies, are especially at risk, partly because of a thickened DM and weak endothelial adhesion, but also because of reduced visibility from the dense arcus, which precludes a view of the inner lip of the incision when instruments are introduced4.
3. Preventing DM Detachment during Surgery
Using blunt instruments to create corneal incisions predisposes to this problem, as the tip of the keratome or slit knife may then push on the elastic DM, separating it from the stroma instead of perforating it. The same can happen if the eye is significantly hypotonic at the time of incision creation, as some resistance from the intraocular pressure allows the knife to penetrate the tissues easily.
When introducing instruments into the eye, it is essential to ensure that the anterior chamber is formed. With the availability of OVDs, it is easy to form the chamber first before introducing a Simcoe's cannula, phacoemulsification probe, or irrigation aspiration cannula into the eye. It permits the surgeon to depress gently on the posterior lip of the wound at the time of entry into the eye, to avoid catching and stripping the cut edge of the DM at the roof of the entry tunnel. The infusion on the instrument should only be turned on after the probe enters the AC, and the infusion port clears the inner lip of the incision, as the fluid exiting the irrigation ports can strip the DM during the introduction through the tunnel. Gentle hydration of the ports after surgery is mandatory, taking care to nestle the opening of the cannula against the stroma in the walls of the corneal opening and not at the entry into the eye to avoid DM stripping. In predisposed eyes, using a superior scleral incision can be considered, as it is easier to manage a superior DM detachment if it occurs4.
4. Types of DM Detachment
Depending on the separation of the DM from the posterior stroma Mackool et al. classified DM detachment into planar and non-planar. When the separation is 1mm or less, it is termed a planar detachment and can resolve spontaneously. DM detachments are also categorized as - peripheral or central, superior or inferior, and single or multiple. Delayed onset DM detachments have also been described. These often occur in the setting of tears in the DM at the sites of corneal incisions. As these untreated tears fibrose in the postoperative period, they can separate from the corneal stroma, and a detachment can occur5.
5. Assessing the DM Detachment
A DM detachment must be suspected when unexpected corneal edema is noted on the day after surgery. In the presence of significant edema, it is not unusual for an underlying DM detachment to be missed unless specifically looked for. If suspected, dilating the pupil may help, as some of the features of a DM detachment may be better seen on retro illumination against the red fundal glow seen in a dilated pupil6.
When assessing a DM detachment, the following features are essential - configuration, material causing the detachment, presentation of the DM, and area of detachment. These features help in surgical planning and in predicting the prognosis for surgical repair6.
A hammock configuration is a separation starting at the corneal ports of entry - due to injections during hydration. The fluid enters the aforementioned potential plane, separating the DM sheet to varying extents. The opening in this type of detachment is, therefore, at the site of the port. A detachment with a tear is often from the phaco wound. It may be associated with a DM separation due to the entry of fluid into the DM-stromal interface. The most severe kind is a complete tear separating the detachment into two or more flaps and is due to physical trauma resulting from contact of instruments or the nucleus of the lens during extraction, with the endothelium5.
The interface material can be air, saline, viscoelastic or blood, and influences the surgical plan. A careful exam is performed that maps the detachment - noting fibrosis, scrolling, and areas of DM loss. Detailed drawings are made in the notes documenting all the above findings to help during surgical repair.
An anterior segment OCT can help differentiate - loose flap with a tear, hammock, attachment to iris, and scrolling. To improve visibility during the assessment, deturgescing the cornea with hypertonic saline or glycerol can help. Various classification and management protocols based on different AS-OCT criteria have been proposed including those by Jacob et al., Sharma et al. and the HELP algorithm by Kumar et al. The gist of these different protocols can be distilled to the fact that noting the type, extent, and location of the DM detachment is necessary to decide on management6,7.
Apart from the characteristics of the DM detachment itself, it is essential also to note additional findings like the extent of corneal edema that can preclude visualization during surgery, the presence and stability of an intraocular lens, the integrity of the posterior capsule and the presence of vitreous in the anterior chamber, and any iris defects or synechiae. Assessment of the health of the posterior segment after complicated cataract surgery helps determine the visual prognosis.
6. Factors affecting Surgical Planning
The detachment area, its relation to the wound, and areas of attachment must be mapped carefully preoperatively, as these will serve as portals of entry during the surgery. Areas, where the DM is detached, are poor sites for entry ports as manipulation through these areas will worsen the DM detachment. Areas of maximal separation are noted, as the venting incisions can be sited here, to allow removal of the material within the DM detachment.
A single, hammock type, superior separation, presenting early, has a good prognosis. Fibrotic, torn membranes with loss of DM and interface viscoelastic have a more guarded prognosis. Peripheral, planar detachments, with a clear central cornea, can be observed6.
7. Surgical Repair of the DM Detachment
Surgery is best performed under periorbital anesthesia, as repeated anterior chamber entry, pressurizing the chamber, and the duration of surgery make topical anesthesia suboptimal. To improve visibility during surgery, hypertonic saline or glycerol, dilating the pupil for the red reflex, using a light pipe, and removing the corneal epithelium, can help.
Accessing the AC requires paracenteses, which are sited in areas of attached DM, typically perpendicular to the area of detachment, and sometimes, multiple ports are required. After making the paracentesis, a small air bubble is injected into the anterior chamber. Venting incisions are made to evacuate fluid from the interface after removing corneal epithelium at the site, to avoid the possibility of epithelial ingrowth. The site of venting incision is chosen at the site of maximal separation, and away from the visual axis. Careful entry using a sharp knife is made into the cavity of the detachment and is stopped at the first sign of egress of fluid. The air in the anterior chamber serves to facilitate this maneuver since the escape of air through the vent implies a full-thickness incision in the cornea. If there is a DM scroll, small amounts of air or saline can be used with a 30G cannula or stroking maneuvers on the surface can be used to unfurl the DM; direct manipulation is best avoided8.
A choice of tamponading agents is available. For hammocks, air is used, while detachments with tears will require a long-acting agent, like 20% SF6 or 14% C3F8. When there are tears, hanging membranes and fish mouthing at the wound, full-thickness 10-0 nylon sutures, with buried knots are used, avoiding the visual axis. After the use of a tamponading agent, proper head positioning is important, and a pupillary block is avoided with an inferior iridotomy, dilating the pupil, and burping air at the slit lamp, when necessary2,9.
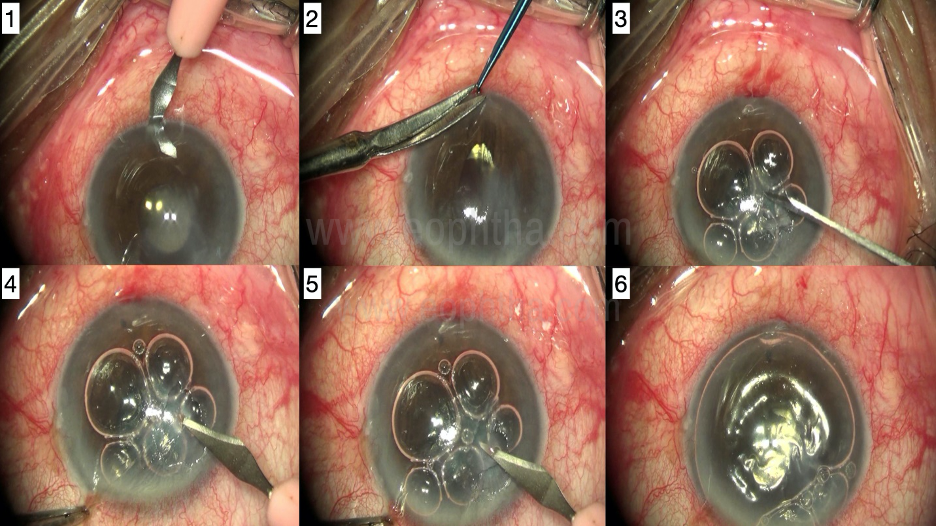
Figure 1 - DM detachment repair - Technique
- Inferior paracentesis - at the site where the DM is attached
- Inferior peripheral iridotomy to minimize the chance of pupillary block postoperatively
- Removing corneal epithelium at the site of venting incision
- Venting incision away from the visual axis, at the site of maximum separation of the DM (noted during preoperative slit-lamp evaluation)
- Fluid egress at the site of venting incision indicating entry into the pocket of DM detachment
- Complete air fill at the completion of the procedure
8. Postoperative Care
In the first few hours after surgery, proper positioning of the patient's head is essential to allow the air to tamponade and promote the attachment of the DM.
In central detachments, a supine position without pillows is helpful, while in superior detachments, a reclining position in the bed allows better tamponade. Inferior detachments require hyperextension of the neck to allow the air in the chamber to tamponade the inferior DM, and it is often difficult for the patient to maintain this position for more than a few hours.
Usually, the attachment is achieved in the initial postoperative period, and if successful, the DM is attached on the first postoperative day. The air bubble in the AC is absorbed over varying periods, and if it occupies a significant portion of the chamber, positioning is maintained over the next few days.
In the case of long-acting gases in the anterior chamber, which are used in more complicated configurations of the detachment, they can take between 2 and 3 weeks to get absorbed, and flying in unpressurized aircrafts must be avoided during this time. With the use of any tamponading agent, pupillary block and increased intraocular pressure in the postoperative period is possible and must be carefully monitored.
Routine postoperative medications include topical antibiotics, steroids, and cycloplegic agents. If there is residual edema in the early postoperative period, hypertonic saline drops and ointment can help speed up the resolution of corneal clarity2.
9. Outcomes
If performed using the principles outlined, the success rates are 70 to 75%, especially in uncomplicated DM detachments3.
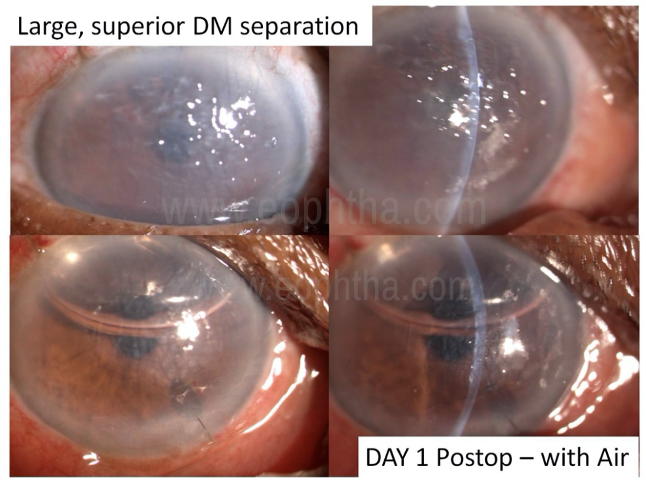
Figure 2 - Pre- and postoperative pictures of an eye with DM detachment, following surgical repair
10. Complications
During surgery, maneuvers can sometimes result in trauma, further separation, and tearing of the DM. The site of the venting incision can predispose to epithelial ingrowths, and the full-thickness corneal sutures used to secure hanging flaps of DM can serve as portals of entry, allowing the spread of infections in the cornea or the eye. Sometimes, especially in extensive detachments, despite following the principles of repair, the DM fails to reattach partially or wholly. In such situations, while further injections of air can be tried, recourse to corneal replacement surgery may be required2,3.
REFERENCES
- Murphy C, Alvarado J, Juster R. Prenatal and postnatal growth of the human Descemet's membrane.Invest Ophthalmol Vis Sci. 1984;25(12):1402-1415.
- Singhal D, Sahay P, Goel S, Asif MI, Maharana PK, Sharma N. Descemet membrane detachment.Surv Ophthalmol. 2020;65(3):279-293.
- Odayappan A, Shivananda N, Ramakrishnan S, Krishnan T, Nachiappan S, Krishnamurthy S. A retrospective study on the incidence of post-cataract surgery Descemet's membrane detachment and outcome of air descemetopexy. Br J Ophthalmol. 2018;102(2):182e6
- Benatti CA, Tsao JZ, Afshari NA. Descemet membrane detachment during cataract surgery: etiology and management.Curr Opin Ophthalmol. 2017;28(1):35-41.2
- Mackool RJ, Holtz SJ. Descemet membrane detachment. Arch Ophthalmol 1977; 95:459–463
- Sharma N, Singhal D, Nair SP, Sahay P, Sreeshankar S S, Maharana PK. Corneal edema after phacoemulsification. Indian J Ophthalmol 2017; 65:1381-9
- Jacob S, Agarwal A, Chaudhry P, et al. A new clinico-tomographic classification and management algorithm for Descemet's membrane detachment. Cont Lens Anterior Eye 2015; 38:327–333
- Ghaffariyeh A, Honarpisheh N, Chamacham T. SupraDescemet's fluid drainage with simultaneous air injection: an alternative treatment for Descemet's membrane detachment. Middle East Afr J Ophthalmol. 2011;18(2):189e91
- Sharma N, Gupta S, Maharana P, Shanmugam P, Nagpal R, Vajpayee RB. Anterior segment optical coherence tomography-guided management algorithm for Descemet membrane detachment after intraocular surgery. Cornea.2015;34(9):1170e4