
Ocular accommodation is an integral visual function that optimizes the visual perception through the focusing ability of the crystalline lens. This closed-loop system constantly interacts with the oculomotor system for finer focusing and alignment of the eyes under naturalistic binocular viewing conditions.
This write-up is intended to provide an overview of the commonest anomalies of accommodation encountered by an eyecare practitioner through case-based learning. For detailed reading, the readers are requested to refer to Scheiman & Wick.1The table below provides an overview of the commonest clinical signs, and symptoms seen in different anomalies of accommodation. 1, 2
|
ANOMALIES OF ACCOMMODATION |
DIAGNOSTIC CRITERIA |
ETIOLOGY |
PRIMARY SIGNS |
SYMPTOMS |
|
Accommodative insufficiency (Not due to sclerosis of the crystalline lens) |
Accommodation amplitudes (AA) lesser than expected for the patient’s age |
Usually idiopathic, can result from certain systemic medications |
Decreased AA for age (2D lesser compared to Hofstetter’s minimum expected amplitudes for the age), Difficulty with minus lenses, Increased lag of accommodation |
Asthenopia, Blurred vision at near, Difficulty reading, poor concentration and/or Headaches |
|
Ill sustained accommodation |
The AA is normal but fatigue occurs with repeated accommodative stimulation |
Accommodative adaptation or slow accommodation, excessive near work |
Difficulty with minus lenses, reduced accommodative facility |
Blurred vision after prolonged near work, Asthenopia |
|
Accommodative infacility |
Slow or difficult accommodative response to dioptric changes in stimulus |
Idiopathic, excessive near work |
Reduced accommodative facility (difficulty with both plus and minus lenses) |
Intermittent blurring at distance after extensive near viewing and vice versa |
|
Spasm of accommodation |
Ciliary muscle spasm that produces excessive accommodation |
Fatigue, systemic or cholinergic drugs, ocular trauma, head injury, brain tumours, Psychogenic factors, Overstimulation of the parasympathetic nervous system or a poorly functioning sympathetic counterpart |
Prefers more myopic correction than objective refraction, lead of accommodation in dynamic retinoscopy, esodeviation at near, variable visual acuity |
Impairment of distance vision |
Case 1:
A 19-year-old college student reported with complaints of eyestrain associated with reading and playing video games. The symptoms begin after 10-20 minutes of near work and is associated with pain around the eyes. His unaided visual acuity was 6/6, N6 in both the eyes and he has never used glasses so far. The rest of the eye health examination was normal and the patient’s medical history was unremarkable.
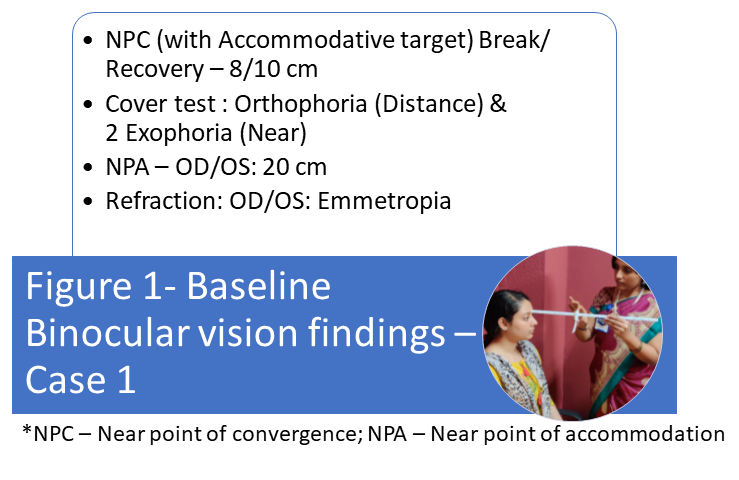
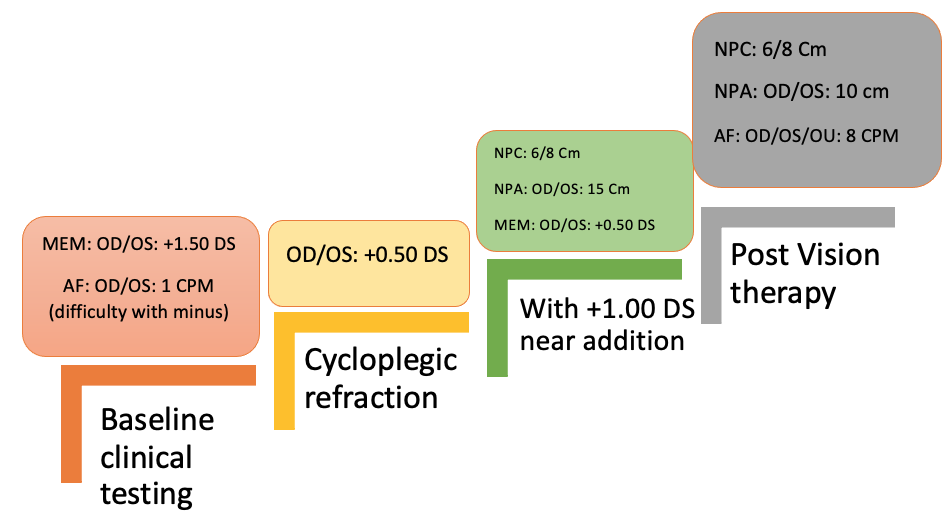
Figure 2 *MEM – Monocular estimate method dynamic retinoscopy; AF: Accommodative facility (with +/-2.00 DS accommodation flippers)
The baseline binocular vision assessment (Figure 1) points out the fact the near points of accommodation are below the age-expected norms.3,4 Though the near point of convergence appears borderline, given the fact that the accommodation amplitudes are reduced, the accommodation parameters need to be investigated in detail prior to making the diagnosis. The further assessment also indicated an increased lag of accommodation assessed using the MEM retinoscopy and difficulty with minus lenses in accommodative facility testing. Based on the relative accommodation findings, a near addition of +1.00 DS was prescribed as a primary management option followed by in-office vision therapy. The patient reported significant improvement in asthenopic symptoms, with concurrent improvement in clinical parameters (Figure 2). The near addition was later weaned off with home vision therapy provided as maintenance therapy.5
Case 2:
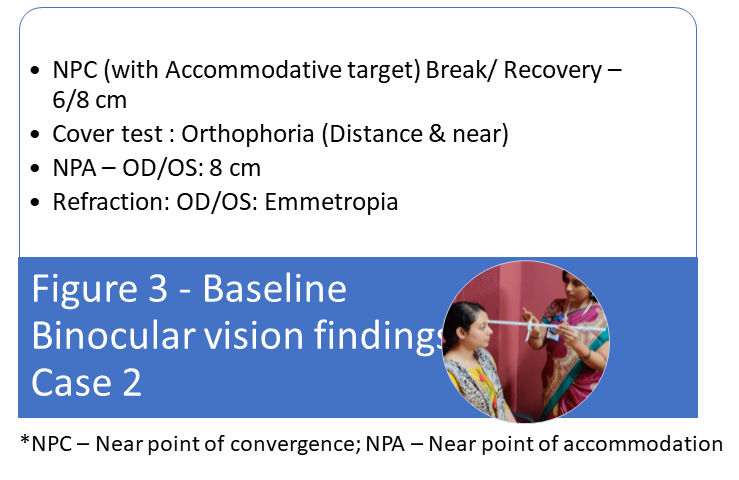
A 29-year-old software professional reported with complaints of intermittent blurring of distance vision followed by 30 minutes of near work. His unaided visual acuity was 6/6, N6 in both the eyes, and his refraction was insignificant to be contributing to the symptoms. The rest of the eye health examination was also normal and the patient’s medical history was unremarkable.
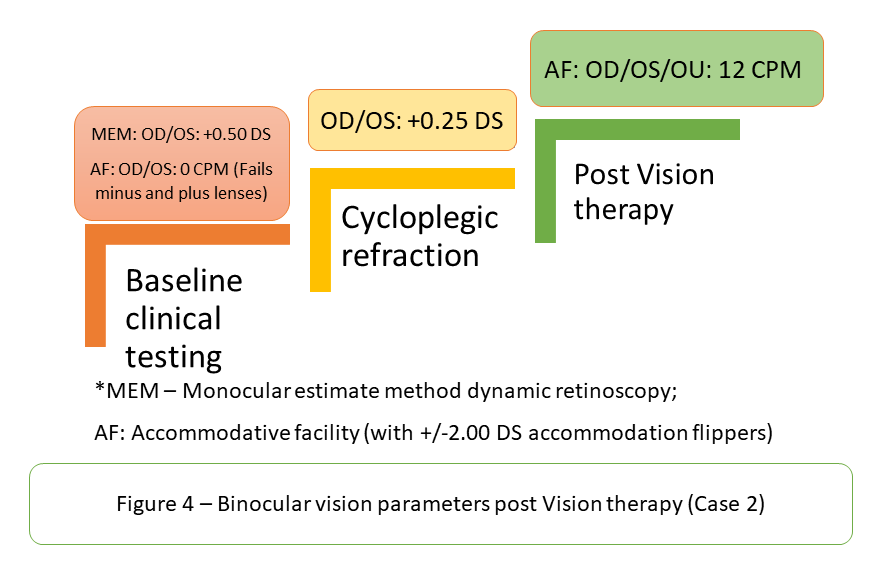
*MEM – Monocular estimate method dynamic retinoscopy; AF: Accommodative facility (with +/-2.00 DS accommodation flippers)
The baseline binocular vision assessment (Figure 3) indicates poorer accommodative facility and also difficulty in both stimulating and relaxing accommodation. This is typical of accommodative infacility, which has been reported to be the commonest binocular vision dysfunction.6 Visual hygiene measures such as frequent blinking, frequent breaks implanting the 20-20-20 rule, and vision therapy to improve accommodation parameters are efficient in improving accommodation infacility and restoring the accommodation parameters to normal ranges.
The objectives of vision therapy in accommodation anomalies aims at improving the amplitudes, response, and dynamics of accommodation using appropriate tools and techniques. The commonest vision therapy techniques used in the management of accommodation anomalies include but not limited to Hart chart, accommodation flippers and word rock card, and loose lens accommodation rock. 1 Providing optimal refractive correction, and near addition in required cases are the primary management options before initiating vision therapy.1 Following vision therapy, significant improvements were reported by the patient with respect to the asthenopic symptoms with concurrent improvements in parameters of the accommodation facility (Figure 4). The cases illustrated in this write-up depict the commonest presentations of anomalies of accommodation in a clinical set-up and proposes a conceptual framework for diagnosis and management from an evidence-based perspective.
References
- Scheiman M, Wick B. Clinical Management of Binocular Vision: Heterophoric, Accommodative and Eye Movement Disorders.4th ed. Philadelphia: Lippincott Williams & Wilkins; 2014.
- American Optometric Association. Care of the patient with accommodative and vergence dysfunction. 2nd ed. St. Louis (MO): American Optometric Association; 2006 (https://my.ico.edu/file/CPG-18---Accomodative-and-Vergence-Dysfunction.pdf)
- Hofstetter H.Useful age‐amplitude formula.Optom World1950;38:42–45.
- Hussaindeen JR, Rakshit A, Singh NK, Swaminathan M, George R, Kapur S, Scheiman M, Ramani KK. Binocular vision anomalies and normative data (BAND) in Tamil Nadu: report 1. Clin Exp Optom. 2017 May;100(3):278-284. doi: 10.1111/cxo.12475. Epub 2016 Oct 30. PMID: 27796049.
- Hussaindeen JR, Murali A. Accommodative Insufficiency: Prevalence, Impact and Treatment Options. Clin Optom (Auckl). 2020 Sep 11;12:135-149. doi: 10.2147/OPTO.S224216. PMID: 32982529; PMCID: PMC7494425.
- Hussaindeen JR, Rakshit A, Singh NK, George R, Swaminathan M, Kapur S, Scheiman M, Ramani KK. Prevalence of non-strabismic anomalies of binocular vision in Tamil Nadu: report 2 of BAND study. Clin Exp Optom. 2017 Nov;100(6):642-648. doi: 10.1111/cxo.12496. Epub 2016 Nov 18. PMID: 27859646.