
LASIK is the most widely used technology for the correction of most spherocylindrical ametropias because of its safety and its predictability that leads to excellent outcomes for both the patient and the surgeon. Over the years there has been a progressive refinement of the technique. Customised correction of refractive errors using wavefront technology has revolutionised the way we plan and execute the treatment of refractive errors there are two specific reasons why customised treatment is transforming the entire LASIK arena. The first is that wavefront technology allows us to treat or not the only second order aberrations such as sphere and cylinder but also a higher order aberrations such as coma and spherical aberrations which exist in normal individuals as well as post refractive surgery patients. A major shift in the thought process of refractive surgery is that the LASIK surgeon now seeks to enhance vision beyond what nature itself and designed. With the advent of adaptive optics it would seem possible to enhance and correct not only the eye is aberrations but also improve contrast significantly. For some tasks this improvement can be significant.
Let us first of all define what is customisation Chambers 21st Century dictionary defines Customize as (verb) adapt, convert, modify, tailor, alter, adjust, suit, fit, transform colloq. fine-tune . Thus customised correction seeks to optimises the clarity of the eyes optical system and attempts to correct not only the sphere ,the cylinder and astigmatism ,but also the aspherical and asymmetrical anomalies which may exist. This is an ideal technique for not only correcting decentred ablations, corneal scarring , following injury, penetrating keratoplasty and even following inappropriate catarct surgery. .
There are various factors which one needs to considered before applying the proceedure
Age as a criteria
Experience has shown that the agent is an important factor to be considered when applying customisation procedures. Many studies have shown that my occupations over the age of 40 to 50 are much more susceptible to hyperopic overcorrection. In addition reports have shown that treating younger patients with myopia more aggressively and reciprocally hyperopia leads to higher patient acceptance. The reason why that is so is that the young eyes generally have a large range of accommodation so a slight hyperopic overcorrection does not really affect the ability to see clearly. On the other hand it is always preferable to over correct older persons more aggressively for hyperopia and less for myopia so as to leave them slightly myopic since the obviously have limited accommodative amplitudes. Over correcting an older myopic can blur both distance and near while a slight under correction would provide a functional near vision for many tasks .
Size of the LASIK flap
Flaps are usually designed on to match the intended the size of the ablation. Thus one would prefer a larger flap for hyperopic ablations as compared to myopia. Very often when treatment is expected to be difficult and the surgeon can assume that he is going to retreat this patient having a slightly larger flap is far better as it allows more room in case a hyperopic pretreatment needs to be superimposed on and over a myopic primary treatment. It is important for the surgeon to know as to what is flap thickness is, vis a vis, the microkeratome he utilises. But in our and definitive study utilising the ACS microkeratome it was found that the mean corneal thickness measured 124.8+/- 18.5 um , indicating that the flaps are thinner than predicted by the manufacturers plate depth measurement. While another study showed progress of thinning/thickening of the flap in the direction towards the hinge.
Larger estimating errors also require a larger transition zone to ensure smooth transition and avoid relegation. It also makes sense to utilise a cross cylinder ablation in eye is with a large amounts of myopic or mixed and astigmatism as it significantly reduces the quantum of cylinder to be corrected in each Meridian by almost 50% and thus is very tissue saving.
Factors to be considered for customised correction
Customisation based on corneal topography
Corneal surface aberrations and irregularities can be easily calculated from corneal abberation data derived from corneal topographic measurements using a computerised topographer . Using this technique is very useful when the aberrations is as essentially corneal in origin typically corneal scars or excess/irregular astigmatism induced following penetrating keratoplasty It has an excellent potential for enhancing visual ability as it seeks to reduce the induced aberrations which impinge on the ability to see clearly. It is also ideal for decentred ablations with the irregular induced astigmatism. Interestingly it is the penetrating keratoplasty patient can see 6/6 and read N5 , in theory, with excellent vision albeit with glasses, but who in reality is acutely unhappy with the distortion of the induced residual astigmatism and higher order abberations. The rationale of corneal based customisation is that it significantly improves the quality of life and brings great benefit to these patients . Often an examination of the Ocular wavefront abberometry maps of these eyes will show a fair quantum of higher order aberrations which are responsible for inducing the blurred vision and which if eliminated , significantly improves contrast.
There are often questions asked as to the role of optimised LASIK as compared to wavefront guided LASIK. Optimised LASIK essentially utilises a software which gives the best possible result by optimising the placement of the excitement of device LASIK gives good results when the astigmatism is regular and there is a reasonable quantum of consistency between refraction and astigmatism and that noted on corneal topography. For eyes with low powers and with low quantum of astigmatism perhaps optimisation gives excellent results. Usage of a optimisation technique diminishes the quantum of lower order aberrations of the eye and results in good vision. To summarise if aberrations on the corneal surface irregular, investing when his is irregular, if examination of corneal topography maps is mediation in quantum of astigmatism in the upper and lower quadrant or indifferent accordance then corneal wavefront guided LASIK perhaps gives the best results
In many ways Corneally wavefront guided Lasik has a fair number of advantages.
- No accommodation influence.
- No limitation due to pupil size and therefore large treatment-zones are possible.
- Aberrations which are measured belonging to the cornea .Excimer laser ,basically , treats on cornea where the origin of these measured aberrations is.
- The extensive majority of the aberrations are originated to the corneal shape. For normal eyes about 80% of the aberrations should be based on the corneal surface where the largest change between the refractive index, going from one medium (air) to another (tear film), is observed.
- Many topographers have the advantage of providing repeatability tests . These give the information of the quality and the ability to have reproducible multiple measurements taken at one examination allowing the topographer technician to get the best pictures.
There are however some disadvantages attached to doing only a corneally wavefront guided Lasik.
- If during the measurement always the same mistakes are made, all measurements will be consequently wrong.
- The repeatability test might display a good result, because all measurements are similar and all are done with the same fault. Therefore the repeatability test is just one of the tests and circumstances which must be considered.
- The spherical (refraction) will not be measured. The system measures the corneal data very precisely but neither the length of the eye is known nor the other optical parts like the lens or the vitreous.
The measured cylinder only represents the corneal component. This does not necessarily mean the patient adapts to this cylinder because other optical measurements are not taken.
There is a word of caution. It must be clearly understood that :-.
- Intra ocular aberrations are not measured with the corneal topographer.
- Compensation from ocular aberrations cannot be seen.
- To reduce measurement artifacts acquire the images by using the joystick together with the footswitch.
- The measurement should be taken within 3 seconds to get a regular, stable tear film and to avoid the break-up of the tear film.
- Medications which are influencing the tear film should not be used prior to the measurement.
- The pupil should not be dilated. Otherwise a shift of the pupil centre at a large and at a small pupil size might effect the treatment.
- A daily calibration of the system with an artificial target is needed.
- Correct fixation of patient and correct conus positioning is necessary
- Important: Pupil must be detected correctly (no artifacts) to perform Corneal Wavefront because its treatment is based on pupil
Customisation based on Wavefront measurements :
Measurement of ocular abberations can be done in many ways. a Shack Hartman wavefront sensor, a Tscherning wavefront sensor, a spatially resolved refractiometer or even some of the many new systems (Tracey) coming on the market. These techniques measure the eye is a wavefront aberrations including second (sphere and cylinder), asymmetric or coma like( third, fifth order), symmetric or spherical like aberrations (fourth ,six )order. While all the systems utilise a ray tracing in one form or another, each system has developed a unique manner of accessing the displacement of a ray of light from its ideal position which defines the slope of the wavefront and then by computation ,the actual wavefront. The difference between the actual wavefront and an ideal wavefront defines the aberrations of an eye. Assessing the aberrations of the eye they find the form of an ideal or a customised laser treatment

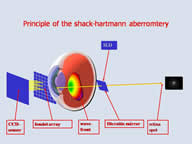

Click the picture to enlarge
Advantages of Optical wavefront guided Lasik using the Hartman Shack abberometer.
- Refraction measurements (sphere, cylinder and axis) are possible and very precise. Especially cylinder and axis has put out to be very precise.
- The influence of higher order aberrations to the sphere and the cylinder can be brought into conjunction. This is the determination of the sphere and cylinder according to the "Seidel" calculation
- Measurements of the refraction at patients with irregular eyes (e.g. re-treatments)are mostly possible and more accurate than other objective methods.
- The complete optical system is measured - all refractive errors are therefore computer , not only the cornea.
There are some disadvantages of Ocular wave front guided Lasik
•Although the aberrometer fogs the target by +1.5 diopter; with the intention to guide the patient to a far view; the measurement depends on accommodation.
•Restricted pupil size leads to a restricted application of a working zone.
•In dark pupils extreme caution to extrapolate dilated data to application.
There are a few points of caution which need to be exercised with Ocular Wave front ablations.
Extreme caution with the pupillary zone. Max. optical treatment zone is related to the pupil diameter (max. diameter which is analyzed by the system). As far as possible no medication before measurement as the use of a cycloplegic will lead to an improper calculation. If the pupil is too small, 2.5% Neosynephrine would seem to give the best result with the least optical problems. Also one must remember that this is a pure aberrometer measurement, you d’ont know the location of the aberrations. They might be related to the cornea, to the lens or other optical parts of the eye.
Pupillary diameter is a constant: An important point often forgotten is that it is vital that refraction between manifest and measured ocular refraction should be compared at thesame pupil diameter(RZ = refractive zone). Commonly during the determination of the manifest refraction the pupil diameter is around 4 mm (photopic conditions). If this manifest refraction should be compared to the wavefront aberration a similar analyzing diameter (e.g. 4 mm) should be used at the aberrometer. No pachymetric measurements is permitted with corneal contact directly prior to measurement with these diagnostic systems. This might affect the result.
Contact lens discontinuance is mandatory before any measurement , be it corneal wavefront or ocular wavefront . : Soft contact lenses are best discontinued at least two weeks prior . Hard 4 weeks prior to the measurement.
Combining ocular and corneal wave frontAblations.
If the wave aberrations of the complete eye and the cornea are available the relative abberations of the different ocular surfaces to the retinal image quality can be successfully evaluated. The wavefront aberration of the internal ocular optics can be estimated simply by direct subtraction of the ocular and corneal aberrations. However in practice since the ocular and corneal aberrations are obtained with two different instruments a problem arises on how to determine the correct reference entering four registration. Customarily the pupil is selected however in normally adumbrated eyes even very small misalignment would probably introduce errors which may be difficult to estimate.
The simplest application of this combined procedure is to carry out each one separately. In a post-keratoplasty case with gross corneal irregular astigmatism, a corneal topography-based LASIK done as a primary procedure, subsequently followed by ocular wavefront guided LASIK total three months later would give excellent results . Many results have shown that wavefront guided LASIK cannot remove all the higher order aberrations on an average but it can certainly reduce aberrations compared to conventional ablations .
References
- Marcos S. Aberrations and visual performance following standard laser vision correction. J Refract Surg 2001; 17:S596–S601.
- Holladay JT, Dudeja DR, Chang J. Functional vision and corneal changes after laser in situ keratomileusis determined by corneal sensitivity, glare testing, and corneal topography. J Cataract Refract Surg 1999; 25:663–669.
- Alessio G, Boscia F, La Tegola MG, et al. Topography-driven photorefractive keratectomy: results of corneal interactive programmed topographic ablation software. Ophthalmology 2000; 107:1578–1587.
- Alessio G, Boscia F, La Tegola MG, et al. Topography-driven excimer laser for the retreatment of decentralized myopic photorefractive keratectomy. Ophthalmology 2001; 108:1695–1703.
- Applegate RA, Nuñez R, Buettner J, et al. How accurately can videokeratographic systems measure surface elevation? Optom Vis Sci 1995; 72:785–892.
- Knorz MC, Jendritza B. Topographically-guided laser in situ keratomileusis to treat corneal irregularities. Ophthalmology 2000; 107:1138–1143.
- Knorz MC, Neuhann T. Treatment of myopia and myopic astigmatism by customized laser in situ keratomileusis based on corneal topography. Ophthalmology 2000; 107:2072–2076.
- Alió JL, Belda JI, Osman AA, et al. Topography-guided laser in situ keratomileusis (TOPOLINK) to correct irregular astigmatism after previous refractive surgery. J Refract Surg 2003; 19:516–527.
- Huang D. Physics of customized corneal ablation. In: MacRae SM, Krueger RR, Applegate RA, eds. Customized corneal ablation: the quest for supervison. Thorofare, NJ, Slack; 2001:51–56.
- Huang D, Arif M. Spot size and quality of scanning laser correction of higher-order wavefront aberrations. J Cataract Refract Surg 2002; 28:407–416.
- Krueger RR. Technology requirements for customized corneal ablation. In: MacRae SM, Krueger RR, Applegate RA, eds. Customized corneal ablation: the quest for super vision. Thorofare, NJ, Slack; 2001:133–147.
- Mrochen M, Seiler T. Influence of corneal curvature on calculation of ablation patterns used in photorefractive laser surgery. J Refract Surg 2001; 17:S584–S587.
- Pallikaris IG, Kymionis GD, Panagopoulou SI, et al. Induced optical aberrations following formation of a laser in situ keratomileusis flap. J Cataract Refract Surg 2002; 28:1737–1741.
- Mrochen M, Donitzky C, Wüllner C, et al. Wavefront-optimized ablation profiles: theoretical background. J Cataract Refract Surg 2004; 30:775–785.
- Gatinel D, Hoang-Xuan T, Azar DT. Volume estimation of excimer laser tissue ablation for correction of spherical myopia and hyperopia. Invest Ophthalmol Vis Sci 2002; 43:1445–1449.
- Martinez CE, Applegate RA, Klyce SD, et al. Effects of pupillary dilation on corneal optical aberrations after photorefractive keratectomy. Arch Ophthalmol 1998; 116:1053–1062.
- Oliver KM, Hemenger RP, Corbett MC, et al. Corneal optical aberrations induced by photorefractive keratectomy. J Refract Surg 1997; 13:246–254.
- Oshika T, Klyce SD, Applegate RA, et al. Comparison of corneal wavefront aberrations after photorefractive keratectomy and laser in situ keratomileusis. Am J Ophthalmol 1999; 127:1–7.
- Moreno-Barriuso E, Merayo Lloves J, Marcos S, et al. Ocular aberrations before and after myopic corneal refractive surgery: LASIK induced changes measured with laser ray tracing. Invest Ophthalmol Vis Sci 2001;42:1396–1403.Thibos LN. The prospects for perfect vision. J Refract Surg 2000; 16:S540–S546.
- Williams D, Yoon GY, Porter J, et al. Visual benefit of correcting higher order aberrations of the eye. J Refract Surg 2000; 16:S554–559.
- Seiler T, Mrochen M, Kaemmerer M. Operative correction of ocular aberrations to improve visual acuity. J Refract Surg 2000; 16:S619–S622.
McLellan JS, Marcos S, Prieto PM, et al. Imperfect optics may be the eye’s defence against chromatic blur. Nature 2002; 417(6885):174–176.- Brunette I, Bueno JM, Parent M, et al. Monochromatic aberrations as a function of age, from childhood to advanced age. Invest Ophthalmol Vis Sci 2003; 44:5438–5446.