


Inflammatory choroidal neovascular membranes (CNVM) cause an acute and significant visual loss 1,2. Mostly affecting eyes with posterior or panuveitis, the chronic recurrent nature of inflammation further worsens the visual prognosis in these eyes, such as serpiginous like choroiditis, punctuate inner choroidopathy (PIC), multifocal choroiditis, Vogt-Koyanagi-Harada (VKH) disease, presumed ocular histoplasmosis syndrome, toxoplasma retinochoroiditis, etc,.3,4 . The angiogenic stimulus in inflammatory CNVM is driven by local inflammation and/or a degenerative breach in retinal pigment epithelium (RPE)-Bruch’s membrane complex4. An active intraocular inflammation induces the release of several inflammatory mediators including cytokines, chemokines, vascular endothelial growth factor (VEGF) and complement activation, which in turn promote retinal and choroidal neovascularization. Majority of inflammatory CNVM are classic (on fundus fluorescein angiography), and type 2 on spectral domain optical coherence tomography (SD-OCT) 5-8. While most of the studies report sub-foveal location as the commonest5-7, peripapillary CNVMs were the most common in our series (45.2%)8, and in a study by D’Souza et al (53.3%)9.
Treatment options for inflammatory CNVM
Both the diagnosis and treatment of inflammatory CNVM are challenging. Various treatment options for inflammatory CNVM include corticosteroids (local and systemic), laser photocoagulation, anti-VEGF agents, immunosuppressive agents, photodynamic therapy (PDT), and surgical removal of the membrane. There is no consensus on treatment algorithm due to the lack of randomized trials, and the first line of treatment depends upon the clinicians’ discretion based on their experiences.
Corticosteroids: In the pre-anti-VEGF era, corticosteroids were the first and only conservative therapeutic option available for inflammatory CNVMs10. They not only stabilized the visual acuity, but also controlled the inflammation-causing posterior uveitis. They act by inhibiting pro-inflammatory factors and also induce transcription and suppression of prostaglandin and interleukin synthesis11-13. Corticosteroids also interfere with the effects of VEGF11-13. Steroids (systemic or intravitreal injections) have been used as monotherapy, or combined with PDT, or with anti-VEGF therapy, or immunosuppressive agents for treating inflammatory CNVM14. Some practitioners continue to use them as the first line of treatment for inflammatory CNVM in non-infectious uveitis owing to their rapid and strong anti-inflammatory properties.
Photodynamic therapy: Though effective for sub-foveal CNVM, PDT offers only visual stabilization (and not an improvement) and has a high recurrence rate of CNVM due to PDT-induced local inflammation15. Though it has been found more effective for CNVM associated with uveitis than CNVM in age-related macular degeneration (AMD), the use of PDT as a monotherapy for inflammatory CNVM has largely decreased with the growing literature on the safety and efficacy of anti-VEGF therapy.
Immunosuppressive therapy: Immunosuppressants can limit angiogenesis owing to their anti-inflammatory property, and have been shown effective in the treatment of extrafoveal, juxtafoveal and subfoveal CNVMs16-18. Resolution or stabilization of the CNVM lesions have been reported with cyclosporine and mycophenolate mofetil. Combination therapy of systemic immunosuppression with PDT or with anti-VEGF agents is also a useful treatment option19. Successful use of intravitreal methotrexate (single injection) has been reported in a case of multifocal choroiditis with inflammatory CNVM unresponsive to previous three anti-VEGF injections20.
Surgical excision: This was considered several decades ago for large CNVMs or when laser photocoagulation was the only therapeutic option available. This treatment is not considered in the current practice.
With a high rate of complications and recurrence rates with the majority of these treatment modalities, anti-VEGF therapy is emerging as the popular and primary treatment for inflammatory CNVM. Further, the demonstration of VEGF expression in the excised CNVMs in eyes with uveitis justifies its use for treating these membranes by directly targeting their pathogenetic pathway21.
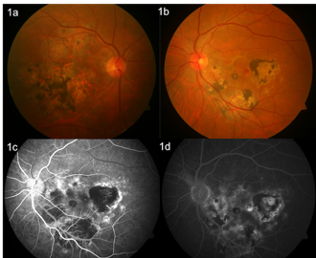
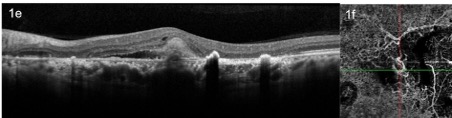
Figure 1: A case of bilateral healed choroiditis (a,b) with inflammatory CNVM in left eye (b). Fundus fluorescein angiography showed mixed fluorescence corresponding to scars in early (c) and late frames (d) with a subtle hyperfluorescence in the fovea in late frame (d) corresponding to the CNVM. SD-OCT scan showed type 2 CNVM with subretinal fluid (e), and OCTA showed the abnormal vascular network (f).
Anti-VEGF therapy for inflammatory CNVM
D’Souza et al reported the long-term successful outcome of inflammatory CNVM with anti-VEGF therapy in terms of visual and anatomical improvement, and low recurrence and complication rates9. Irrespective of the status of uveitis (active or inactive) and the cause of intraocular inflammation, anti-VEGF therapy was highly effective as a therapeutic approach for inflammatory CNVMs. Roy et al reported the outcome of inflammatory CNVM to anti-VEGF therapy in Indian eyes22.
When compared with laser photocoagulation or PDT, prompt response to intravitreal injections, safety, efficacy, and lack of collateral tissue damage to retina and choroid are the major advantages of anti-VEGF therapy6. Both bevacizumab and ranibizumab have been individually (or in combination) effective. The mean number of injections is much less as compared to CNVM in AMD, as reported by Adan et al (mean 1.3 injections)23, D’Souza et al (mean injections 2.6 + 1.2)9, and Fine et al (mean 2.3 injections, range 1-6)24. With no randomized comparative trial, there is no consensus on injection protocol, and the intravitreal injections have been widely used for inflammatory CNVM on PRN basis.
Complications following anti-VEGF therapy are very few and may include submacular fibrosis or hemorrhage, subfoveal RPE rip, ocular hypertension, choroidal detachment, reactivation of intraocular inflammation, or spread of chorioretinal atrophy9,25,26. Recurrence is uncommon and responds favorably to a repeat anti-VEGF agent.
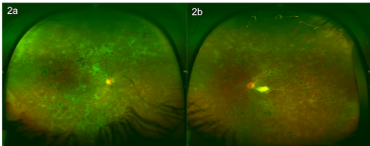
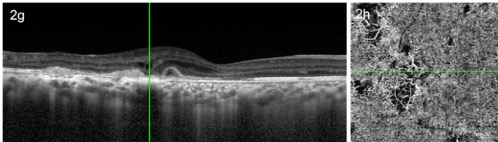
Figure 2: A case of healed serpiginous like choroiditis with extensive scarring (a,b), presented with right eye blurred vision. Fundus fluorescein angiography showed areas of mixed fluorescence in early frames due to scars in both eyes (c,d). The late frames showed a small area of hyperfluorescence in the fovea in the right eye (e), suggesting a CNVM, while the left eye showed a brightly hyperfluorescent lesion near the disc, corresponding to the scar (f). SD-OCT showed a subretinal CNVM complex with intra-retinal and subretinal fluid (g). OCTA showed the abnormal CNVM complex (h).
Challenges in inflammatory CNVM
An inflammatory CNVM can develop in the presence or absence of concurrent active intraocular inflammation. In an eye with active uveitis, the clinical symptoms and signs of active intraocular inflammation take precedence over the signs of inflammatory CNVM, hence, leading to its missed or a delayed diagnosis. In eyes with chronic inflammation, the pre-existing fundus pigmentary changes complicate the presenting manifestations of inflammatory CNVM. However, the advances in ocular imaging tools have largely overcome the clinical challenges in their diagnosis.
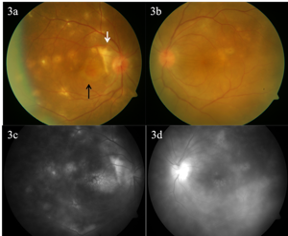
Figure 3: Fundus photograph showing multifocal choroiditis with panuveitis in both eyes (a, b), with a peripapillary choroidal neovascular membrane in the right eye (white arrow) and a subretinal hemorrhage in macula (black arrow). Fluorescein angiography shows hyperfluorescence corresponding to active lesions in both eyes with cystoid macular edema (c, d).
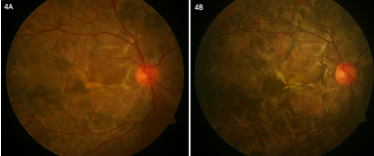
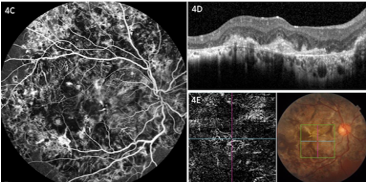

Figure 4: Fundus photograph at four years follow up of a case of serpiginouslike choroiditis (SLC) treated with oral corticosteroids and anti-tuberculous therapy, showing healed lesions (A). Fundus photograph when patient presented with blurring of vision (vision decreased from 6/36 to counting fingers at two meters) (B), fluorescein angiography was inconclusive showing mixed fluorescence (C), SD-OCT showed few pockets of intraretinal fluid (D), and OCTA showed an abnormal vascular network suggestive of inflammatory CNVM (E). Following a single intravitreal injection of ranibizumab, the vision improved to 6/36. Fundus photograph (F) showed scars of SLC, SD-OCT (G) showed resolution of intra-retinal fluid, and OCTA (H) showed decreasing CNVM complex.
How do we treat inflammatory CNVM?
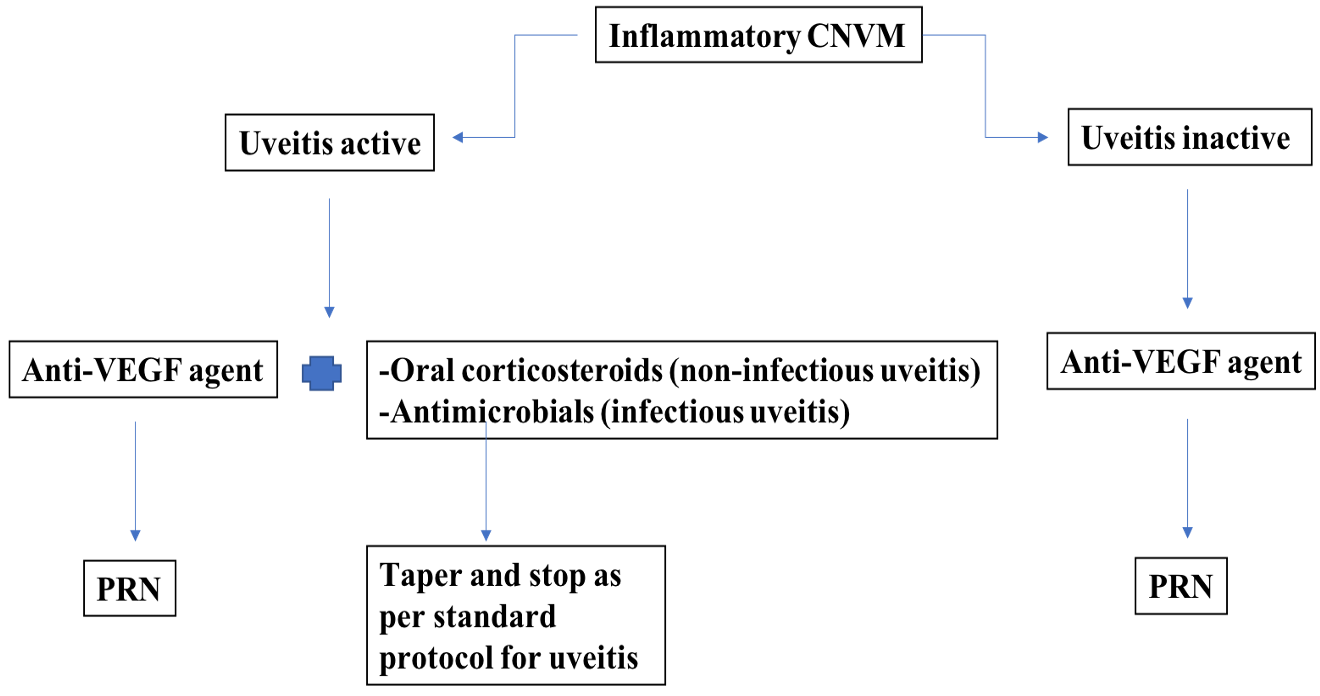
In our previously published report of inflammatory CNVM, we treated the majority of the eyes (78%) with intravitreal bevacizumab (1.25 mg in 0.05 ml), followed by oral corticosteroids (9.6%), and transpupillary thermotherapy (1.4%). We kept 10.9% eyes under close observation and added immunosuppressive agents in 6.8% eyes8. But these treatment modalities were administered to patients seen between 1998 and 20138. In the current era of anti-VEGF therapy, intravitreal injections (ranibizumab) are our first choice of treatment, both in infectious and non-infectious uveitis. Ancillary testing with relevant ocular imaging is performed, which often includes color fundus photography, fluorescein angiography, SD-OCT and OCT angiography (figures 1-3). If the eye has concomitant active uveitis (non-infectious), we also start (or escalate) systemic corticosteroids (usually oral prednisolone 1mg/kg/day)25. The immunosuppressive agents are usually continued in the maintenance dose. For active infectious uveitis with inflammatory CNVM, such as toxoplasmic retinochoroiditis, an anti-VEGF agent may be combined with intravitreal clindamycin plus dexamethasone. For inflammatory CNVM in tubercular uveitis, the anti-tubercular therapy is continued till its complete regimen. For eyes developing inflammatory CNVM without any active uveitis, an anti-VEGF agent is usually injected as monotherapy on PRN basis (figure 4). Recurrences are treated with repeat anti-VEGF agents.
References:
- Pai SA, Hebri SP, Lootah AM. Management of recurrent inflammatory choroidal neovascular membrane secondary to Vogt-Koyanagi-Harada syndrome, using combined intravitreal injection of bevacizumab and triamcinolone acetate. Indian J Ophthalmol 2012;60:551-2.
- O’Toole L, Tufail A, Pavesio C. Management of choroidal neovascularization in uveitis. Int Ophthalmol Clin 2005;45:157-77.
- Ahnood D, Madhusudhan S, Tsaloumas MD, Waheed NK, Keane PA, Denniston AK. Punctate inner choroidopathy: a review.Surv Ophthalmol.2017;62(2):113–126.
- Baxter SL, Pistilli M, Pujari SS, et al. Risk of choroidal neovascularization among the uveitides.Am J Ophthalmol.2013;156(3):468–477.e2.
- Perentes Y, van Tran T, Sickenberg M, Herbort CP. Subretinal neovascular membranes complicating uveitis: frequency, treatments, and visual outcome. Ocul Immunol Inflamm 2005;13:219 –24.
- Dhingra N, Kelly S, Majid MA, et al. Inflammatory choroidal neovascular membrane in posterior uveitis – pathogenesis and treatment. Indian J Ophthalmol 2010;58:3-10.
- Olk RJ, Burgess DB, McCormick PA. Subfoveal and juxtafoveal subretinal neovascularization in the Presumed Ocular Histoplasmosis syndrome: visual prognosis. Ophthalmology 1984;91:1592–1602.
- Bansal R, Bansal P, Gupta A, Gupta V, Dogra MR, Singh R, Katoch D. Diagnostic challenges in inflammatory choroidal neovascular membranes. Ocul Immunol Inflamm 2016;15:1-9.
- D’Souza P, Ranjan R, Babu U, Kanakath AV, Saravanan VR. Long-term visual and anatomical outcomes after intravitreal anti-vascular endothelial growth factor therapy. Retina 2018;38:1307-1315.
- Martidis A, Miller DG, Ciulla TA, Danis RP, Moorthy RS. Corticosteroids as an antiangiogenic agent for histoplasmosis-related subfoveal choroidal neovascularization.J Ocul Pharmacol Ther.1999;15(5):425–428.
- Rothova A. Corticosteroids in uveitis.Ophthalmol Clin N Am.2002;15(3):389–394.
- Edelman JL, Lutz D, Castro MR. Corticosteroids inhibit VEGF-induced vascular leakage in a rabbit model of blood-retinal and blood-aqueous barrier breakdown.Exp Eye Res.2005;80(2):249–258.
- Oliver A, Ciulla TA. Corticosteroids as antiangiogenic agents.Ophthalmol Clin N Am.2006;19(3):345–351.
- Agarwal A, Invernizzi A, Singh RB, Foulsham W, Aggarwal K, Handa S, et al. An update on inflammatory choroidal neovascularization: epidemiology, multimodal imaging, and management. J Ophthal Inflamm Infect 2018;8:13.
- Rogers AH, Martidis A, Greenberg PB, Puliafito CA. Optical coherence tomography findings following photodynamic therapy of choroidal neovascularization. Am J Ophthalmol 2002;134:566-576.
- Dees C, Arnold JJ, Forrester JV, Dick AD. Immunosuppressive treatment of choroidal neovascularization associated with endogenous posterior uveitis.Arch Ophthalmol.1998;116(11):1456–1461.
- Neri P, Manoni M, Fortuna C, Lettieri M, Mariotti C, Giovannini A. Association of systemic steroids and mycophenolate mofetil as rescue therapy for uveitic choroidal neovascularization unresponsive to the traditional immunosuppressants: interventional case series.Int Ophthalmol.2010;30(5):583–590.
- Kilmartin DJ, Forrester JV, Dick AD. Cyclosporine-induced resolution of choroidal neovascularization associated with sympathetic ophthalmia.Arch Ophthalmol.1998;116(2):249–250.
- Hogan A, Behan U, Kilmartin DJ. Outcomes after combination photodynamic therapy and immunosuppression for inflammatory subfoveal choroidal neovascularisation.Br J Ophthalmol.2005;89(9):1109–1111.
- Mateo-Montoya A, Baglivo E, de Smet MD. Intravitreal methotrexate for the treatment of choroidal neovascularization in multifocal choroiditis.Eye (Lond).2013;27(2):277–278.
- Shimada H, Yuzawa M, Hirose T, et al. Pathological findings of multifocal choroiditis with panuveitis and punctate inner choroidopathy. Jpn J Ophthalmol 2008;52:282-288.
- Roy R, Saurabh K, Bansal A, Kumar A, Majumdar AK, Paul SS. Inflammatory choroidal neovascularization in Indian eyes: Etiology, clinical features, and outcomes to anti-vascular endothelial growth factor. Indian J Ophthalmol 2017;65:295-300.
- Adan A, Mateo C, Navarro R, et al. Intravitreal bevacizumab (Avastin) injection as primary treatment of inflammatory choroidal neovascularization. Retina 2007;27:1180-1186.
- Fine HF, Zhitomirsky I, Freund KB, et al. Bevacizumab (Avastin) and ranibizumab (Lucentis) for choroidal neovascularization in multifocal choroiditis. Retina 2009;29:8-12.
- Menia NK, Rana N, Bansal R. Choroidal detachment following an intravitreal injection in a patient with Vogt-Koyanagi- Harada disease. Ocul Immunol Inflamm 2019 Oct 30:1-3. doi: 10.1080/09273948.2019.1677919.
- Ranjan R, Agarwal M. Rebound inflammation after an intravitreal injection in Vogt-Koyanagi-Harada syndrome.Ind J Ophthalmol. 2018;66:863-865.