
Question
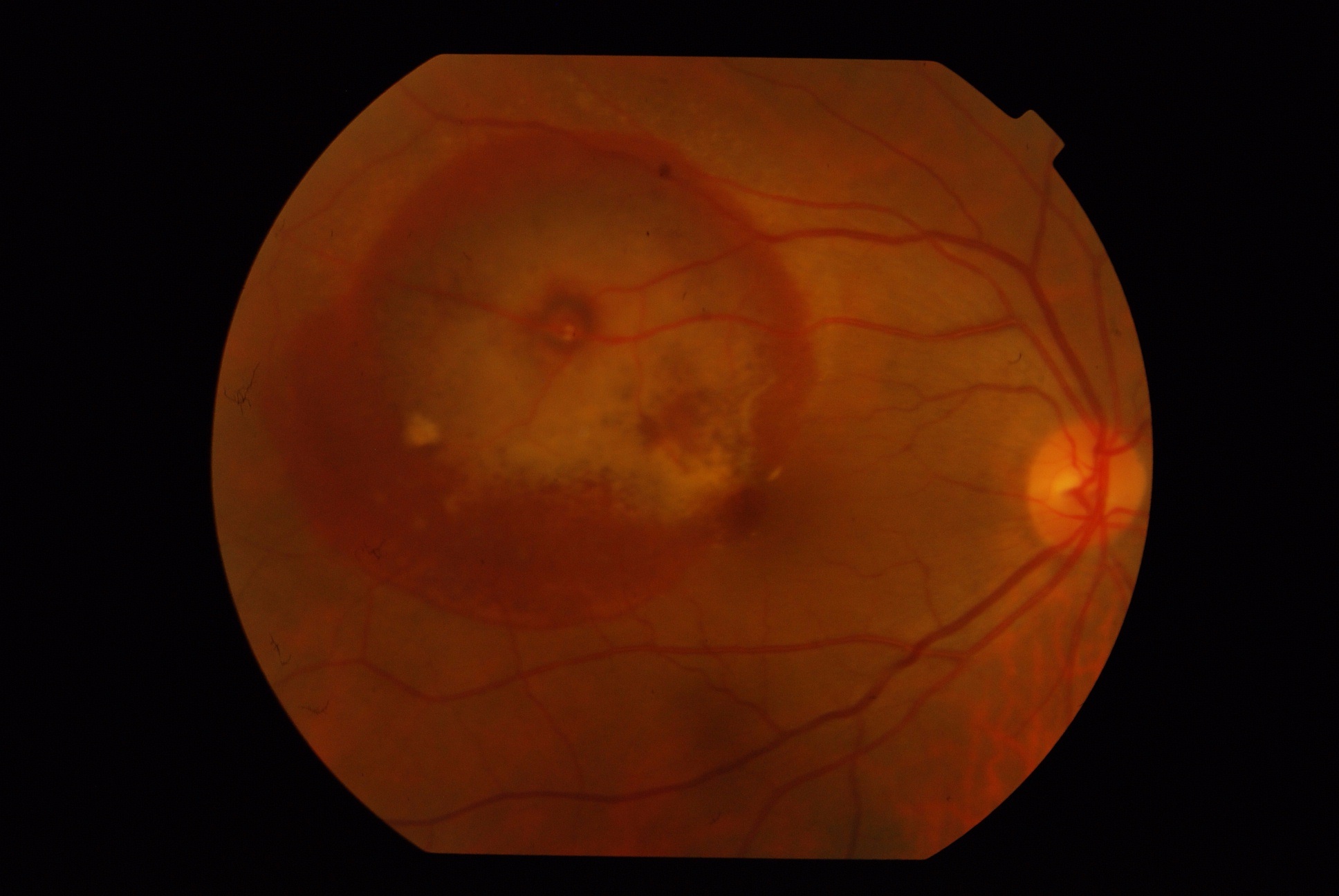
A 52-year-old female presented with sudden onset blurring of vision in OD for 2 weeks. She is a known case of hypothyroidism on regular treatment. There is no other systemic illness. The best-corrected visual acuity in OD was 6/36(p) N12 and 6/6 N6 in OS. The anterior segment is unremarkable. The fundus is as shown:
-
What is the most probable diagnosis?
-
How will you manage the case (investigations and treatment both)
Answer:
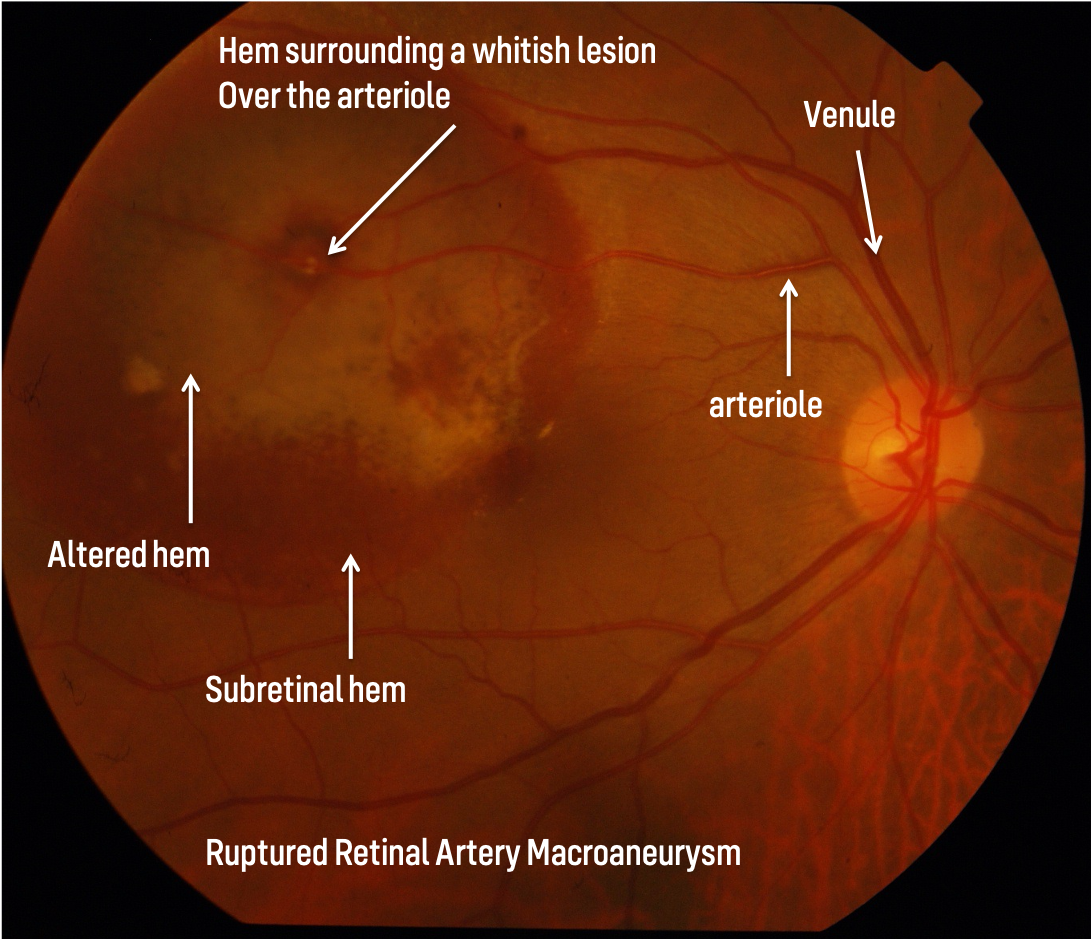
RAM is generally acquired retinal aneurysmal dilation typically occurring within the first 3 bifurcations of the central retinal artery most commonly seen in elderly hypertensive females.
1. Clinical Classification
a) HemorrhagicHemorrhage is the major component extending more than 1 DD with visual loss
b) ExudativeExudation is the major component responsible for visual loss
c) QuiescentEither there is no hemorrhage or exudation or there exists minimal hemorrhage and exudation with minimal or no visual loss
They can be further subdivided as predominantly hemorrhagic or exudative
2.Anatomical Classification
Fusiform(cuffed): circumferential widening of the arteriole
Saccular (blow out): an outpouching of the retinal arteriole
Indefinable: where the exact anatomy was not identified
Some Salient points
-
Occurs within the first three bifurcations, either at the AV crossing or directly at the branch
-
Generally unilateral and solitary, Bilaterality is seen in 10 %, multiple RAM noted in approximately 15-20%
-
The most common systemic association is hypertension, 75% of patients with RAM have hypertension
Differential Diagnosis
In predominantly hemorrhagic type
The subretinal hem can mimic AMD-related CNVM; absence of drusens and examination of other eye may give a clue. An FFA/ICG helps to confirm
If presenting with mounds of subretinal hem with vitreous hemorrhage, PCV is another differential. Again an ICG/ FFA will be helpful in the diagnosis. Another important differential to be kept in mind in an elderly patient presenting with subretinal mounds is choroidal melanoma. USG, MRI of the concerned eye is the most valuable tool in such cases. Valsalva retinopathy is another condition where hemorrhage can be present in any of the retinal layers just as RAM. A history of Valsalva, laterality( generally bilateral), FFA helps in the diagnosis. Other differentials include diabetic retinopathy, Vein occlusion sequelae, . In these cases examination of the other eye, FFA helps in the diagnosis
Investigations
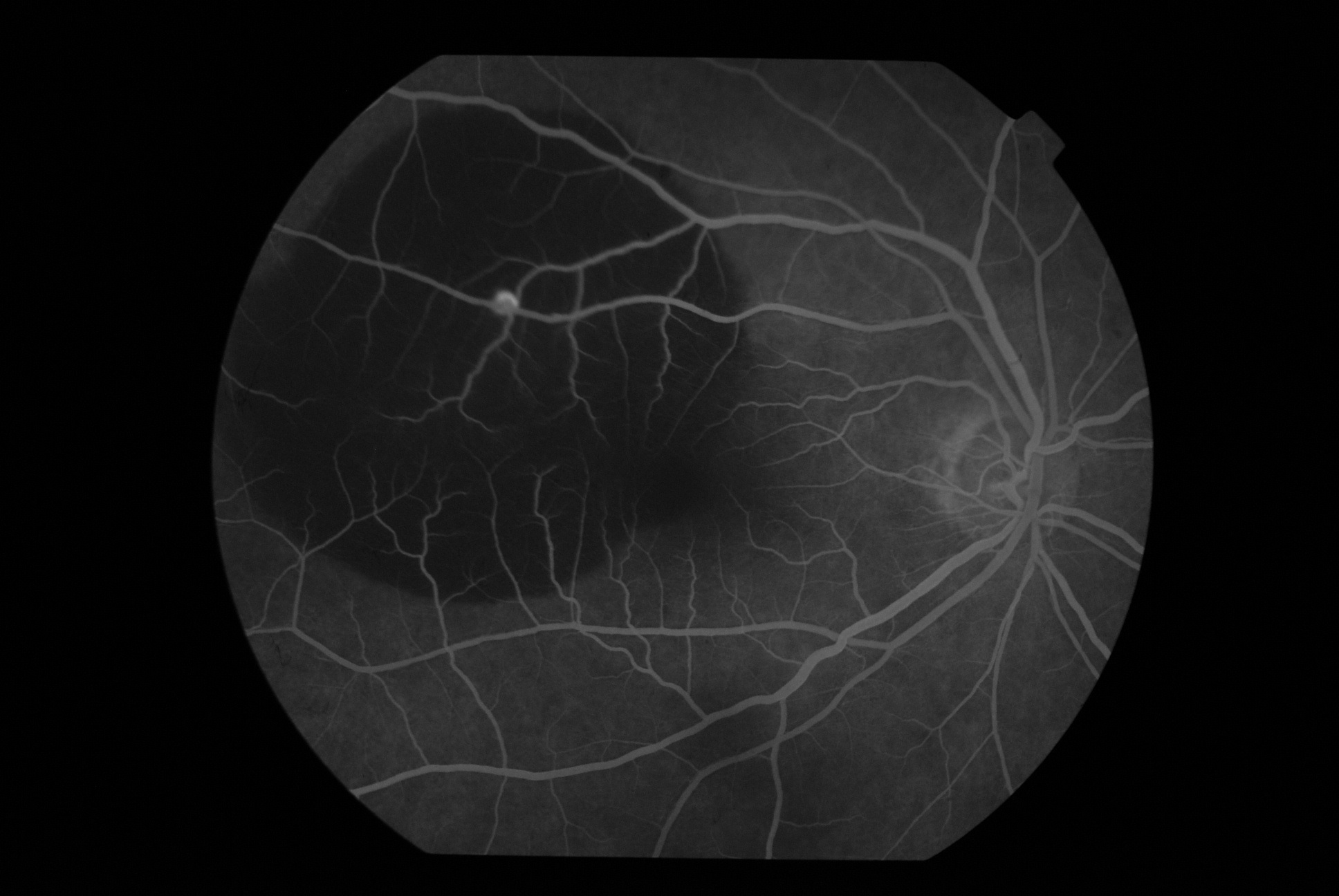
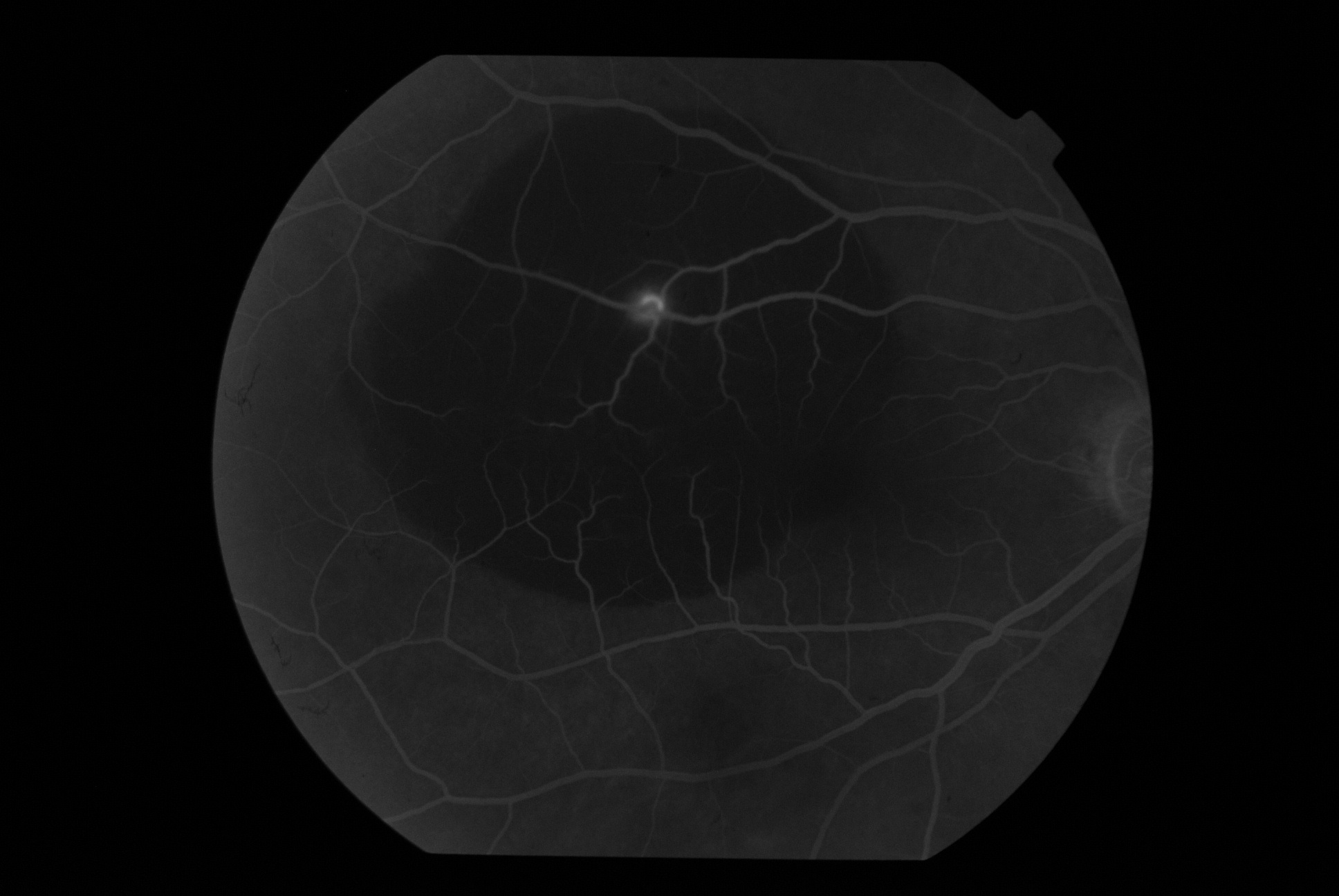
FFA features: it’s the investigation of choice for confirming the clinical entity
1) Saccular RAM show minimal early filling with filling mostly in the middle and late phases
2) Fusiform RAM has rapid early filling. The difference in the filling is because of the difference in the aperture of the neck of the aneurysm
3) RAM may not show uniform filling on FFA. This is because of intraluminal clot formation.
4) FFA may show secondary changes in the form of capillary non-perfusion, collaterals.
5) A characteristic Z shaped kinked appearance is secondary to fibrotic changes in a RAM
6) Sometimes FFA may be inconclusive secondary to blocked fluorescence of hemorrhage. In this scenario, an ICG may help in the diagnosis
OCT: Generally used to diagnose and follow up associated macular edema. Newer SD-OCTs has an excellent resolution which not only helps in diagnosis but also in prognostication of the case
-
If OCT shows complete filling of the lumen; generally indicates a resolved RAM
-
If OCT shows residual fluid collection in the lumen, it generally indicates persistent blood flow necessitating further treatment
A thorough investigation to rule out any systemic factors is as important as ocular investigations. Recording the patient's blood pressure, having a lipid profile, ruling out diabetes are important investigations. A cardiologist referral for ruling out any pathology is also a must.
Treatment
A RAM discovered incidentally: best to observe.
Hence an unruptured RAM without any evidence of exudation/hemorrhage/visual complaints can be observed. A RAM presenting with minimal exudation and with no macular involvement can again be either observed( although very closely) or else can be treated. RAM presenting with hemorrhage and exudation( macula involved) needs treatment. If a RAM is seen clinically and also on FFA, laser is the treatment of choice.
Laser application should be light, heavy white burn should be avoided in fear of causing arteriolar obstruction and subsequent complication. The laser can be either argon green, yellow. A recent laser modality called Micropulse laser has also been used.
RAM if presenting with subhyaloid hem can be treated with Yag Hyaloidotomy. Presentation with submacular hem needs treatment in view of the toxic nature of the blood. Pneumatic displacement with C3F8 with or without tPA is the treatment of choice. RAM presenting with macular edema and predominantly exudation can be treated with the combination of laser and anti-VEGF.
Presentation with dense vitreous hemorrhage ( with no e/o RD on USG) can be initially watched. ( during the initial wait, the patient is instructed to avoid undue exertion and undue head movements. This helps in settling down of the blood)
The observation time traditionally was a minimum of 2-3 months. In view of smaller gauge instruments ( 23,25,27), the period of observation is gradually declining with a safe margin of a minimum of 1 month. Vitrectomy can be performed at the end of the waiting period.