_(1).jpg)
There is no substitute to good history obtained at the start of the examination
As history gives us a direction to look for, and find pertinent signs aiding in diagnosis and management. The various presenting complaints could range from abnormal head posture, deviation noticed by parents or friends, intermittent eye closure, double vision and so on. Some important points to be noted in patients with squint include,
- Family history of squint and wear of glasses (amongst parents, siblings and distant relatives)
- Personal history starting from birth history- Factors such as prematurity and birth weight, nature of delivery (normal/forceps/cesarean)
- Deviation – the age at which it was noticed, the direction of deviation (inward/ outward/ other) the eye deviated, constant or intermittent nature of deviation. Further, if deviation becomes more obvious when the child is inattentive, tired or ill. The diurnal or cyclic pattern if any also has to be noted.
- Any history ofconvulsion, illness or trauma preceded the deviation
- History of diplopia- Confirm if diplopia is uniocular or binocular. Note the nature of diplopia(horizontal/vertical/torsional), in the specific direction of gaze or all positions of gaze, more for distance or near and presence of diurnal variation if any
Examination
1. Inspection of head position.
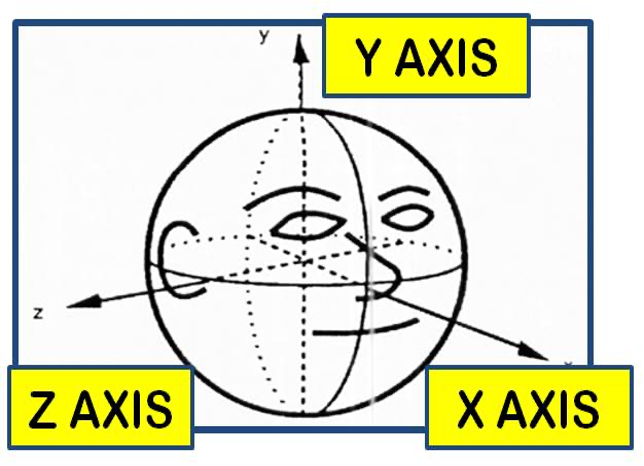
Abnormal head position in any state in which head is not held upright and patient adopts a posture which could be chin up or down( along X-axis ), faces turn to the right or left( along Y-axis ) and head tilt to left or right( along Z-axis) as in fig 1.
Causes of Abnormal head posture/compensatory/anomalous head posture(AHP) :
Ocular causes- Paretic/paralytic strabismus, Nystagmus, A or V pattern strabismus
Non-Ocular causes- contracture /fibrosis of sternocleidomastoid, unilateral hearing loss or psychogenic torticollis
How to check the head posture
Observe the patient as he is entering the clinic and while taking history. Make sure the patient is sitting upright during the examination. Observe for head posture directly in front of the patient, when the patient is looking at near target as well as for distant target. ( Ask him to read near and distant chart). Keep monitoring throughout the consultation. Also, ask for old photographs to rule out any congenital causes.
Differentiate abnormal posture due to ocular cause- when the patient is asked to close his eyes and straighten his head, he holds it upright.
Measuring the abnormal head posture: can be done using an orthopedic goniometer, arthrodial protractor or modified cervical range of motion devices(CROM). A simple yet practical way of measurement can be done using two-scale and protractor.
For face turn: the bridge of the nose is taken as a reference along the anteroposterior axis. Examiners must stand behind the patient and look from up. One arm of the scale placed along the direction of fixation and other along the patient’s anteroposterior axis of the patient ( parallel to )bridge of the nose.
For chin-up/down: examined from one side, one arm of the scale placed along direction of fixation and the other along the anteroposterior axis of face.
For head tilt: examined from the back of the patient, one scale placed vertically, perpendicular to the floor and other along the patient’s face vertical axis ( long axis of the face)
PEARLS: In presence of abnormal head posture, correct the head posture passively before doing cover tests or prism cover tests to measure deviation in primary gaze.
Inspection of facial symmetry
Look for any facial asymmetry. Eg.- face can look asymmetrical in congenital SO palsy and have specific features in cranisynostoses( eg: plagiocephaly)
Inspection of eyes
Observe the width and direction of lid fissure which may give a clue to the presence of pseudostrabismus or pulley heterotopy
Look for features of epicanthic folds, telecanthus, hypertelorism, negative or positive angle kappa.
e. g.- Epicanthic folds cause pseudo-esotropia, hypertelorism causing pseudo exotropia. Negative angle kappa( in high myopes) causing pseudo exotropia
Mongoloid( up slanted palpebral fissure) and antimongoloid slants (down slanted fissure) can give an impression of A or V pattern strabismus simulating pseudo inferior oblique (IO) or superior oblique (SO) overaction or underaction.
Sensory examination
The Sensory evaluation should always precede motor evaluation. In the practical examination set up, it may be difficult to evaluate the sensory system in detail, so the basic tests like Worth 4 dot test and stereoacuity by titmus fly test can be done. The aims of sensory evaluation are to find the grade of binocular single vision in the patient and to note the presence of sensory anomalies if any. Tests for stereopsis should be done at the beginning of strabismus evaluation. Various tests for stereopsis can be classified as qualitative or quantitative tests
The qualitative test includes the LANG PENCIL TEST
The test is done by either holding the pencil horizontally or vertically by the examiner and the patient hold another pencil and brings its tip to approximate one held by the examiner. If he is able to do then stereopsis is present.
Further, the quantitative tests can be grouped as ;
Tests needing polarised or red-green glasses
- Titmus fly test
- Randot tests – TNO and Randot E test
Tests not requiring glasses
- Frisby test
- Lang test I and II
- Synotophore with stereopsis slides
All the above are tests denote stereopsis at near. Those for testing distance stereopsis include AO vectograph, Mentor BVAT system. During examination, Stereopsis testing is not done if the patients complaints of diplopia . In other cases , quick estimate of stereopsis is obtained with randot or titmus test and the amount of stereopsis according to picture recognized is given on the back cover of each chartbook. Rest of tests for sensory evaluation can be classifies as :
- Based on principle : Diplopia or Haploscopic principle
- Based on specific anomalies to be tested
- Based on nature of test : qualitative or quantitative
Based on principle behind the tests :
- Diplopia tests ( foveal - extrafoveal stimulation )
- Use one fixation target seen by both eyes
- Dissociated by red green glasses or striations on lenses
- Examples : Bagolini striated lens test, Worth 4 dot test, Red filter test, Maddox rod test
- Haploscopic principle ( fovea - foveolar stimulation)
- have two fixation targets, one for each eye, and the targets can be moved separately to align with each fovea
- Either by use of mirrors or glasses
- Examples : Synoptophore , Bielschowsky after image test, Lancaster Red green test
What can be done easily during examination is worth 4 dot test
Patient wears the RED and GREEN glasses ( red in front of right eye by convention ) and sees the worth 4 lights on snellen chart ( Worth 4 dot test at distance ) and worth 4 torch [ Worth 4 dot test at near(33cm)] . And patient has to use red green glasses and see these light source and describe the number of lights that they can see.
Worth 4-dot targets have 2 green, one red and one white lights
Results:
- Two red lights - Left suppression
- Three green lights - Right suppression
- Four lights - Orthophoria or Manifest strabismus with ARC
- Five lights – Diplopia or alternate suppression
Hirschberg’sTest
This is one of the light reflex tests for strabismus where we observe the first purkinje image formed by the torch light in front of the patient.
How to perform the Hirschberg’s test- make patient sit comfortably and erect. Correct any abnormal head posture if present. Sit directly in front of patient and show a point light source from a distance and note for corneal reflex. Normally corneal reflex is central and slightly nasal in both eyes( positive angle kappa). Change in corneal reflex position gives an approximate idea about squint.
Eg.- If corneal reflex is shifted nasally- exotropia , if reflex is temporal then eye is esotropic , if reflex is lower then eye is hypertropic. Every millimeter shift equals to an approximate amount of 7 degree of deviation or 15 prism diopters of deviation .
Examination of ocular motility
Both ductions and versions are examined and should be noted for both eyes
How to check for Extraocular movements:
Make the patient sit comfortably in the erect position and sit exactly in front of the patient and using a target or torchlight, depending upon the vision make the patient to look in all nine gazes. And note for any underactions and overactions and note it. Check versions and then and check for ductions for each of the eyes by occluding other eyes.
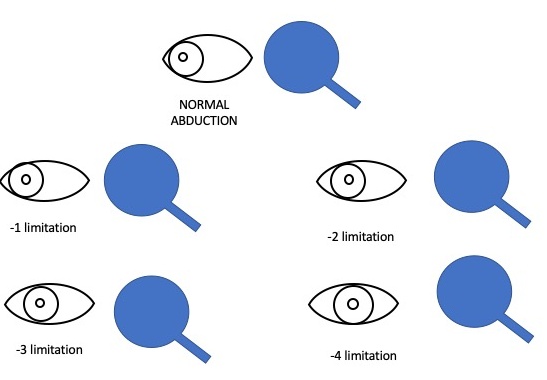
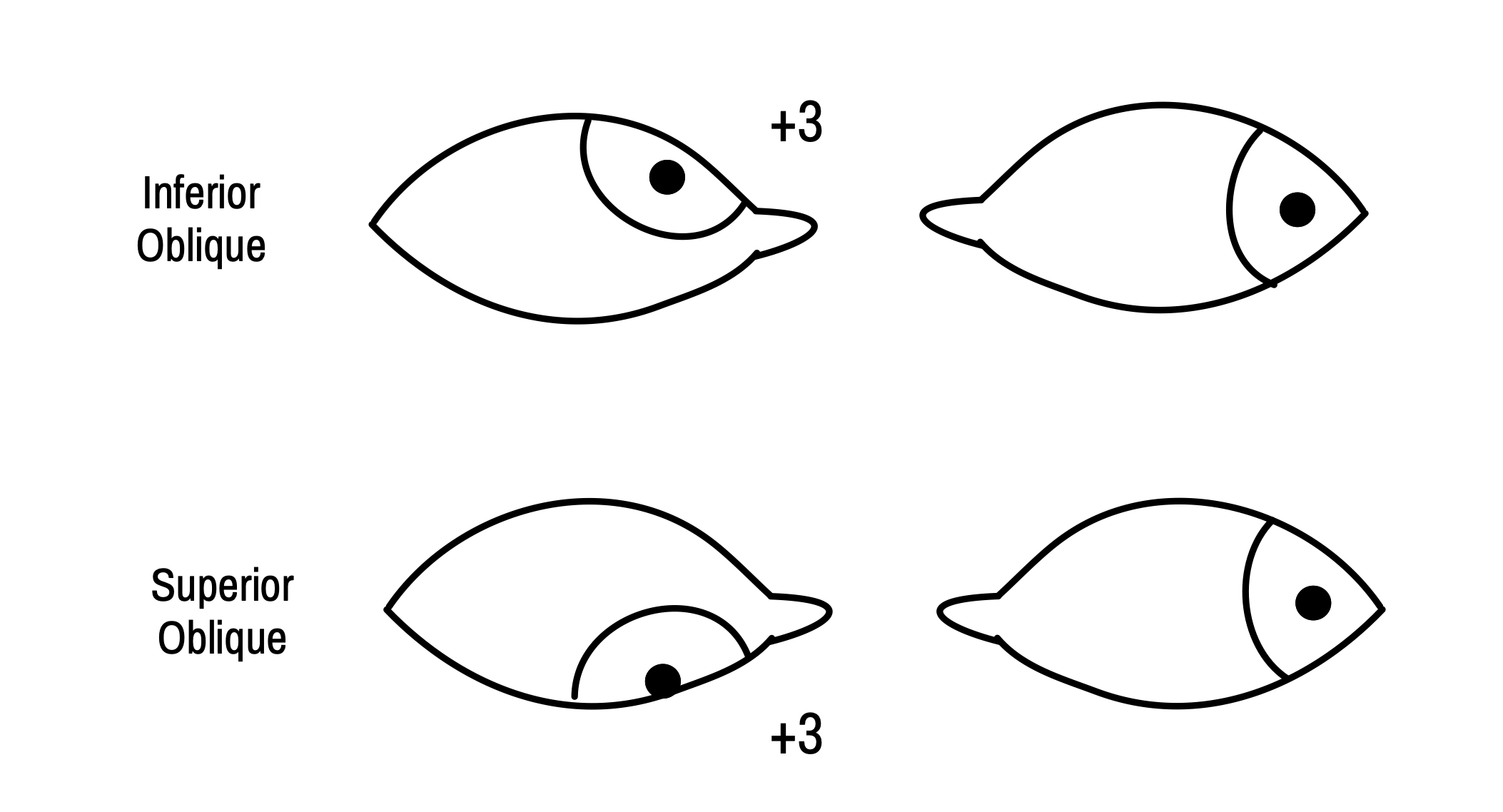
In maximal adduction, an imaginary vertical line through the lower lacrimal punctum should coincide with a boundary line between the inner third and the outer two-thirds of the cornea. If abduction is normal, the corneal limbus should touch the outer canthus. For the action of obliques, abducting eye should be fixing, while we look for freely moving adducting eye and grade them for their actions. An imaginary line is drawn tangentially from the lower limbus of both eyes and the angle between them is taken to grade the actions of muscle.
How do we describe the ocular movements in exams?
First describe the versions ( cardinal positions only ) viz., dextroversion, dextroelevation, dextrodepression, levoversion, levoelevation, and levodepression. Then describe the ductions of each eye viz., adduction, abduction, elevation, and depression.
Describe if movements limited ( limited word preferred as we don’t know still if limitation due to paresis or restrictive pathology) and then say to what grade it is limited ( like limited adduction of -2 and so on)
Convergence need not be mentioned in exams as a routine
Further, the way it is represented is
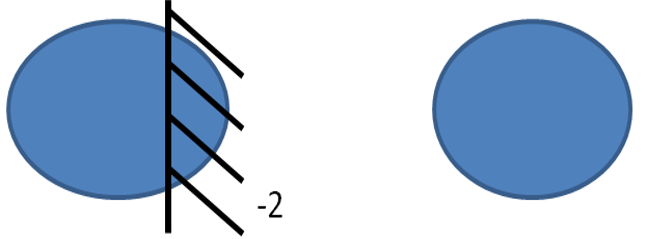
Depicting ADDuction of the right eye is limited to a grade of -2 .
Other wayof representation is
All above representing cardinal positions of gaze.
Motor evaluation of squint
This is done with cover test or cover- uncover test. It establishes whether orthophoria or a heterophoria is present, whether a deviation is latent or manifest, the direction of a deviation, the fixation behavior.
Cover test- done for manifest squint.
How to perform
The patient should be seated comfortably in an erect position with no abnormal head posture. ( correct the abnormal posture if present ) If the patient is using glasses, he should be wearing his full refractive correction. Then he is asked to look at the target (examined for both near with lang’s target or gulden’s fixation target and distance with any 6/12 VA symbol).
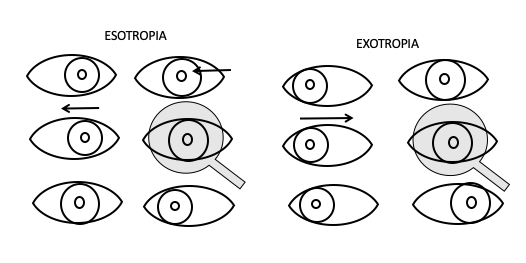
Examiner then covers the patients fixating eye with either his palm or occluder.
Covering one eye disrupts fusion. In the presence of heterotopia, when the eye which is fixating is covered, the opposite eye will move to take up the fixation, if Extraocular movement is free. The covered eye will also make a corresponding eye movement in accordance with Hering’s Law. There is exotropia if the eye moves from out to in towards nose and esotropia if the eye moves out temporally. If there is no movement, then this eye is covered and other eye’s movement is observed.
In the cover test, observe for movement of other eye and not the eye undercover
Cover test showing movement indicates TROPIA
Uncover test- done for latent squint.
When there is no movement of either eye in the cover test as explained above, then with the same cover test, observe the eye undercover for movement. If using translucent occlude then it’s easy to observe for movement of eye under cover indicating phoria. If the eye under cover is moving outward then it is exophoria ; if moves inward then esophoria. Alternatively you can observe the eye after removing cover . In the latter the interpretation is similar to cover test. Meaning with heterophoria, eye moves to take up the binocular fixation. If eyes move from out to in( temporal to nasal), its exophoria and if it moves from in to out its esophoria.
Movement of the eye under cover indicates PHORIA
Alternate cover test: done with covering either eye alternately without allowing both eyes to be open together at any point in time. This indicates both TROPIA and PHORIA
The prerequisites for doing the COVER –UNCOVER tests are :
- Central fixation in both eyes
- Reasonably good vision in both eyes( better than 6/36 to 6/24 in both eyes)
- No gross ocular movement limitations
Low vision or gross ocular limitation warrants use of Hirshberg test to note the ocular deviation if present
Measurement of squint
There are a various test for measurement of deviation as follows-
Alternate Prism bar cover test:
How to perform
Make the patient sit comfortably as above with his corrective glasses.
An alternative cover test is performed and prisms of increasing strength are placed till there is a complete absence of movement or there is a redressal movement of the uncovered eye opposite to the direction of deviation.
The apex of Prism is always placed towards the deviation of the eye. ( base out for esotropia, base in prisms for exotropia and so on)
There could be a combination of horizontal and vertical movements for which horizontal and vertical prisms can be stacked. It’s always advisable to neutralize the horizontal deviation following which vertical deviation is neutralized.
Further two horizontal prisms are not stacked together.
In paralytic strabismus, Deviation is measured with either eye fixating. The deviation with good eye fixing ( prisms in front of the paretic eye) is called primary deviation and paralytic eye fixing( prism in front of the good eye) is secondary deviation and one. It should be done for both near and distant targets as well as in all gazes so as to note incomitance or patterned squint if any.
Simultaneous Prism cover test: done mainly for small-angle strabismus. In this first approximate measurement of strabismus with corneal reflex is estimated. Then prism is placed in front of a non-fixating eye while simultaneously the other eye is covered and if the deviated eye shows the refixation movement then both prism and occlude are removed and the same is repeated with increased amount is prism till there is neutralization in form of no movement or slight redressal movement.
Krimsky test: both of the above tests can be done only if the vision of both eyes inpatient is good. In case of a very poor vision or deeply amblyopic eye, a crude method called prism reflex test was described by Krimsky. Light is shone from front and prism is placed in front of the eye till both the corneal reflex is at the centre.
In patients with complaints of diplopia, it is important to perform and document the diplopia charting.
How to do diplopia charting?
Ask the patient to be seated comfortably against a wall or clear background at a distance of 1 m. A streak of light is projected on the wall in 9 positions of gaze. The patient wearing red-green glasses interprets this streak of light as seen by him. If red and green light seen separately or single, if separated details as to if horizontal, vertical or torsional separation noted.
During exams, this way of recording may not be possible so the patient is shown a finger or a pen in all 9 positions of gaze and asked to tell if he sees double. If sees double, he is asked the direction of the second image and the same plotted.
The chart is plotted as told by the patient( in turn as seen by the patient)
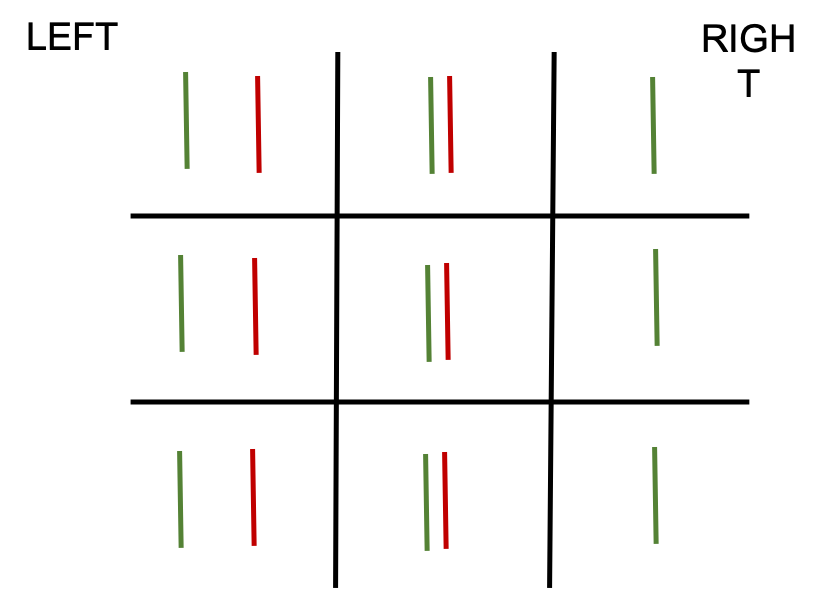
Examples— all are with red goggles in front of the right eye and green in front of the left eye
Rest of ocular examination has to be done as usual
Example
Let us now take the example of left lateral rectus palsy in a patient and describe the way it is to be done in exams
History as described before
Examination :
Important to document and describe CNS examination before ocular examination in all cases of cranial nerve palsy.
Head posture: left face turn
No facial asymmetry
Hirschberg test shows 15 deg left esotropia
Alternate prism cover tests show 30 prism diopters esotropia ( prism in front of the left eye, primary deviation ) 40 PD ( secondary deviation )
Measurement in left gaze around 40 PD esotropia and Orthophoria in right gaze
Measurement at near showed 18-20 PD esotropia
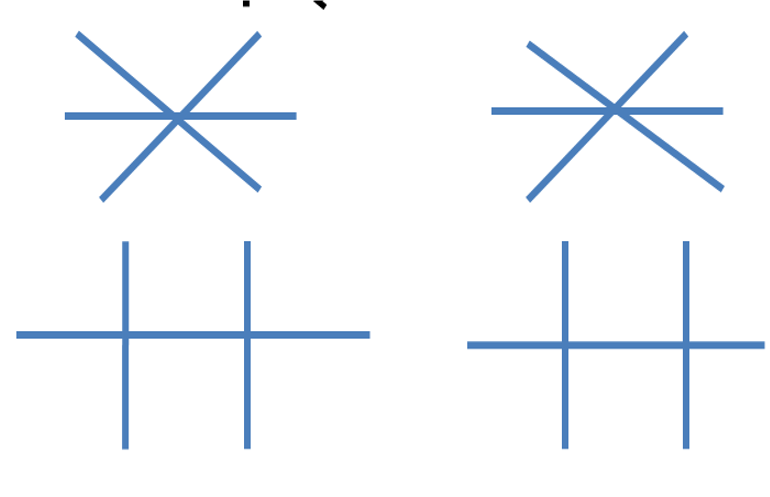
Ocular movement shows
Limitation of levoversion, levoelevation, and levodepression with limitation noted in left eye. Rest of versions i.e., dextroversion, dextroelevation, and dextrodepression are normal
Ductions appear normal in right eye. Abduction is limited in left eye of grade of -3 ,rest of ductions i.e., adduction, elevation and depression are normal
Diplopia chart as described above
Rest of ocular examination findings as routinely described