

Introduction
Ideally a cataract surgery should result in the placement of an intraocular lens (IOL) within the capsular bag. However, this desirable outcome might be averted due to either preexisting zonular deficit or intraoperative posterior capsular tear, resulting in aphakia. This necessitates the need for an alternate means of IOL implantation. The surgeon can exercise the options of an anterior chamber IOL or iris fixated IOL or a scleral fixated IOL. Developments in IOL designs and modifications in implantation techniques have rendered them safe and efficacious. Recent studies have reported no significant differences in the postoperative visual recovery or complications rate between the 3 approaches.1 However, each option should be analyzed not only in accordance with surgeon’s experience but also with patient’s age, local, and systemic comorbidities.2
Scleral fixated IOL (SFIOL) involves sutured/sutureless fixation of the IOL to the sclera. SFIOL’s position closely approximates the normal anatomic position of a within-the-bag IOL. It does not hinder pupillary dilation unlike an iris-claw IOL. Moreover, the occurrence of untoward events such as corneal endothelial decompensation, pupillary block, angle-closure, and ocular inflammation is lesser in comparison to anterior chamber and iris fixated IOL’s.1-4 These factors make SFIOL a favored IOL over the other two. However, it is surgically more challenging and needs a certain amount of dexterity and skill. (See table 1) In this article, we highlight the principles, various techniques, modifications, and outcomes of scleral fixated IOLs.
Indications of scleral‑fixated intraocular lens surgery
Careful selection of patient for scleral fixated IOL will go a long way in ensuring success of the surgery. SFIOL can be performed as a primary procedure or as a secondary procedure at a separate sitting for various complicated situations involving trauma, distorted anterior segment or previous multiple vitreoretinal procedures. It is beneficial for young patients with iris tissue loss, glaucoma, angle abnormalities, corneal endothelial loss, and corneal opacities. However, it is best avoided in patients with extensive limbal scarring, scleral thinning, coloboma choroid, microphthalmos or microcornea, pre-existing filtering blebs, bleeding disorders, and retinal detachment. Similarly, elderly patients who develop intraoperative PC rupture will benefit from an ACIOL if they have a healthy endothelial cell count, no glaucoma or angle abnormality and an intact vitreous face.5,6 It is preferable to minimize tissue dissection and handling in such cases.
Indications:
- Intraoperative posterior capsular rupture
- Planned intracapsular cataract extraction or lensectomy
- Intraoperative zonular dehiscence
- Traumatic cataract with preexisting posterior capsular defect
- Traumatic subluxation of the lens
- Pseudoexfoliation with phacodonesis
- Primary congenital ectopia lentis
- Ectopia lentis associated with disorders such as Marfan’s syndrome, Weil-Marchesani syndrome, Homocystinuria, Sulphite oxidase deficiency, Hyperlysinaemia.
Contraindications:
- Uveitis
- Co-existing retinal detachment (RD)
- Extensive lattice degeneration with a family h/o RD or major retinal diseases
- Uncontrolled glaucoma
- Extensive limbal scarring
Preoperative Considerations:
Several techniques and numerous modifications of SFIOL have been described by various researchers. However, some basic considerations remain constant.
Timing of surgery:
The SFIOL can be done as a primary procedure in a planned manner in cases with known zonular or posterior capsular defect. But in the setting of a complicated cataract surgery, the SFIOL can be implanted primarily at the same sitting or secondarily at a second sitting later. The advantage of a primary SFIOL would be early rehabilitation of the patient, avoidance of a second surgery and avoidance of possible medicolegal problems. Patient satisfaction is maintained. However, it increases the surgical time. The local anesthesia might be required to be supplemented. A secondary SFIOL procedure can be done in more controlled setting after a few weeks once the media have cleared and the cataract wound has healed. Studies have not shown any difference in the visual outcome or complication rates in either primary or secondary implantation.7,8 The decision should be based on the surgeon’s competence and comfort level, patient’s co-operation, and the need for SFIOL.
Sutured or suture-less fixation
The choice will depend on the surgeon’s comfort level in performing the procedure. The sutured method is more complex and necessitates some expertise from the surgeon. It is more durable and gives stable long term results. The suture-less fixation method is easier and can be done quickly. It avoids suture related complications such as suture erosion, endophthalmitis and late dislocation of IOL due to suture breakage. However, it is a fairly recent technique and lacks long term follow up.
Choice of IOL
The IOL type depends on the technique. In case of a sutured IOL, special one-piece, rigid, non-foldable IOL with eyelets on the haptic for passing the suture is chosen. It has a larger optic size of 6 mm and larger overall diameter of 13.5 mm. It gives good centration. Slight backward tilt of the haptics places it well in the sulcus, reduces iris chafing. In case of suture-less technique, a 3 piece foldable lens is used. Although it is easy to insert through a small incision and the haptics are easy to manipulate, it is a smaller sized IOL which is not meant to be stretched between limbus to limbus.
|
Type of IOL |
Advantages |
Disadvantages |
|
ACIOL |
Very easy to perform Does not require special instrumentation Can be done at the same sitting Requires less operative time |
High risk for corneal endothelial damage and decompensation Chance of angle damage, PAS, glaucoma high Risk of hyphema Requires intact iris diaphragm |
|
Iris fixated IOL |
Slightly more difficult to perform than ACIOL but easier than SFIOL Less operative time No special instrumentation needed Can be done at the same sitting |
Requires intact iris diaphragm Pupillary dilation hampered Difficulty in visualizing fundus Risk of corneal endothelial damage in the long term |
|
SFIOL |
IOL in physiologic position in the sulcus Less damage to corneal endothelium Less risk of glaucoma or inflammation Pupillary dilation not affected |
Technically challenging to perform Increased operative time May require a second sitting for SFIOL implantation Requires specialized vitrectomy instruments and machine Risk of retinal detachment in the long term Late dislocation can occur Risk of suture erosion, endophthalmitis present |
Suture considerations
A non-absorbable suture is used to fix the SFIOL. A double-armed, 10-0 polypropylene (prolene) suture with both straight needles is the preferred choice. However, there are some concerns as to suture degradation and late dislocation of IOL reported in approximately 27.9% of eyes after a mean 50 ± 28 months.9 To overcome this problem, 9-0 prolene can be used instead of 10-0 prolene. Of late, CV- 7 or CV-8 polytetrafluoroethylene (Gore-Tex) suture is being used for fixation. It is quite strong and durable. It is expected to last very long but long term data is still awaited. Other advantages are that it is a thick flat suture which is easy to handle. The needle is not required and suture can be passed through the eyelets of the IOL easily.
Anterior vitrectomy V/s Pars plana vitrectomy approach
Both approaches are employed. It depends on the operating surgeon’s preference. A posterior segment surgeon would prefer a complete pars plana vitrectomy. The visual outcomes are similar in both the approaches but the chances of late complications such as retinal detachment are higher with the anterior vitrectomy approach.10 Also, with a pars plana approach, the surgeon is better equipped to deal with complications such as dislocated lens matter.
Surgical principles:
A surgeon can choose many ways to fix a SFIOL, but some principles must be followed to ensure success of the surgery.
- The IOL should be placed correctly in the sulcus.
- The haptics should be placed and fixed exactly 180 degrees apart.
- The corneal center and the points for haptic fixation should in a straight line.
These principles are essential to have a well-centered SFIOL without any tilt. Variations can be done in the methods of passing the suture. Originally described technique was called ab interno wherein the sutures were passed from inside the eye to exit out of the eye at the ciliary sulcus. However this is a blind procedure of passing the sutures and is more suitable with an open sky approach with a concomitant penetrating keratoplasty procedure. It is associated with risks of retinal detachment, hemorrhage, and unpredictable placement of the lens haptics.11 The preferred method is called ab externo in which needles are inserted from outside to inside after marking the ciliary sulcus. This gives a more stable and reproducible final IOL position.12 The number of points of fixation can also differ from 2 points, 3 points or 4 points. The sutures can either be tied to the haptics or looped around the haptic or passed through the hole in the haptic in various manner. There are also many variations of burying the suture ends and knot at the fixation site. Some surgeons prefer partial-thickness scleral flaps, some make scleral pockets or grooves while some leave the suture on the scleral surface but bury the knot alone. These prevent suture erosion, exposure and reduce the risk of endophthalmitis due to exposure. Hoffman described a technique of making scleral pockets starting from the limbal side without conjunctival dissection to prevent scarring.13 Some authors use a technique of multiple passes of the suture through the sclera without any knots to prevent the problem of knot erosion.14
In recent times, the sutureless technique also has witnessed many modifications. In this method the haptics can be inserted into a short scleral tunnel under partial-thickness scleral flaps or simply left in the sclera without any grooves or flaps.
It would be impossible to describe all the variations in the SFIOL surgery. We elaborate below on the basic few techniques in each category. The readers are suggested to read review articles detailing these techniques and watch the educational surgical videos available in public domain.
Surgical Techniques of Sutured SFIOLS
In 1991, Lewis popularized the concept of ab externo suture passes, docking of the straight needle on a 10-0 polypropylene suture into a 28-gauge hollow needle, 180 degrees away and made use of scleral flaps to cover the suture knots.12 This technique is still being used. The surgical steps are as follows:
Two-point fixation with polypropylene suture
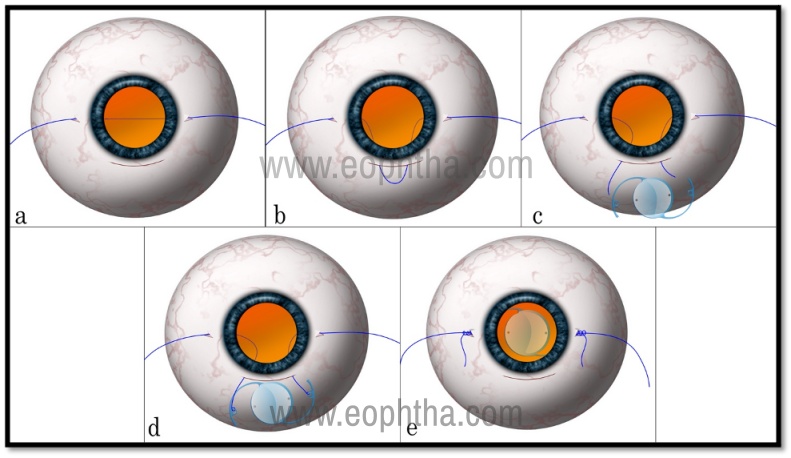
Figure 1: Two Point fixation of sutured SFIOL using 10-0 polypropylene suture. Panel (a) shows the 10-0 prolene suture spanning the ocular cavity from 3 to 9 o’clock passed under partial-thickness scleral flaps. The suture is pulled out from the superior section (b). It is cut in the middle (c) and the ends are tied to the IOL haptics (d). The IOL is inserted inside, the sutures are tied in the bed of the flaps (e).
This technique is elaborated in figure 1. The main steps after lens removal and vitrectomy are as follows-
- The two points of fixation usually at 3 and 9 o’clock are marked on the cornea with the help of a radial keratotomy marker which is centered on the pupillary center.
- Partial-thickness scleral flaps or pockets about 3x3 mm are made at these points.
- Entry points for both needles are measured 1 mm posterior to the surgical limbus at the marked points. The straight needle of either 10-0 or 9-0 polypropylene suture is inserted at this point, a 26G hollow needle is inserted from the opposite side. The polypropylene needle is docked into the hollow needle and taken out from the opposite side.
- The suture traversing the eye is externalized with the use of a second instrument inserted through a superior corneal or corneoscleral incision.
- The suture is cut in the middle and each end is tied to one haptic of the IOL.
- The IOL is then introduced into the eye and maneuvered posterior to the iris with the haptics resting in the ciliary sulcus while the sutures are pulled out. Another suture bite is taken near each of the previous scleral entry points, in the bed of the flap and each suture is tied onto itself to secure the haptics to the sclera.
Four Point Fixation with polypropylene suture:
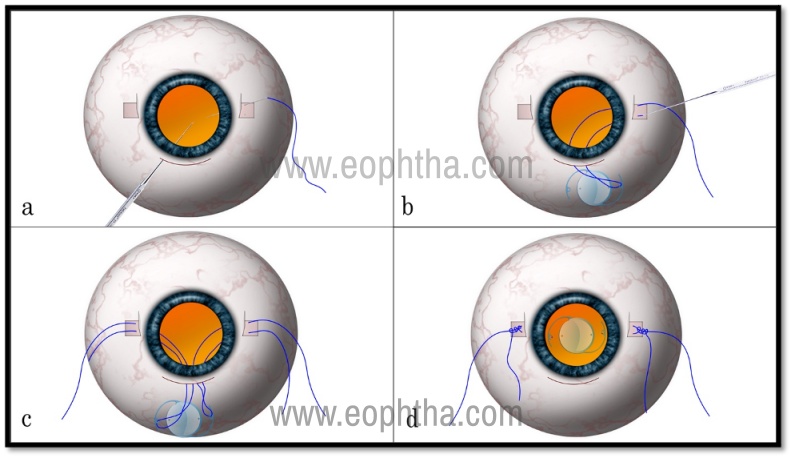
Figure 2: Four Point Fixation with 10-0 polypropylene suture. A straight needle of the 10-0 prolene needle is passed into the eye under the flap on one side and docked into a hollow 26G needle passed from the superior section and taken out (a). The needle is passed through the eyelet on the haptic to thread the IOL and turned back into the AC and taken out from under the flap by the same docking technique (b). The same procedure is repeated on the other side and the other eyelet is also threaded (c). The IOL is inserted inside and the sutures are tied to give a stable 4 point fixation (d).
This technique gives a wider fixation of the haptics, thus giving more stability to the SFIOL, less chances of tilt or astigmatism. The main steps are shown in figure 2.
- Partial-thickness scleral flaps or pockets are made 180 degree apart after marking the pupillary center and the radial positions at 3 and 9 o’clock meridia.
- The double-armed 10-0 polypropylene suture is cut in the middle and one needle is passed under the scleral flap 1mm behind the limbus and 1mm on one side of the radial mark. This is docked into a 26 G needle inserted through the superior corneoscleral tunnel and taken out.
- It is passed through one of the eyelets on the haptic of the IOL.
- Now the 26G needle is passed into the eye from under the flap of the same side, 1 mm from the limbus and 1mm from the radial mark on the other side. The 10-0 needle is turned back and inserted into the eye through the superior section and docked into the 26G needle and taken out under the flap.
- The same steps are repeated on the opposite side.
- The IOL is inserted in the eye, positioned in the sulcus while drawing the sutures tight. The sutures are tied and knots are buried. The scleral flaps can be sutured or glued.
Four-point fixation with GORE-TEX suture
Of late a soft, flexible, monofilament, non-absorbable suture made of polytetrafluoroethylene (ePTFE) biomaterial (Gore-Tex) is being increasingly used for scleral fixation of IOLs. It has the advantage of potentially lasting very long and thus reducing the late dislocation seen very commonly with a 10-0 polypropylene suture 10-15 years later. But long term data about its viability is still not available. It is also easy to handle, easy to insert and knot. The suture lies flat on the sclera and over time gets integrated into it reducing chances of any erosion or exposure. Figure 3 shows the main steps which are as follows-
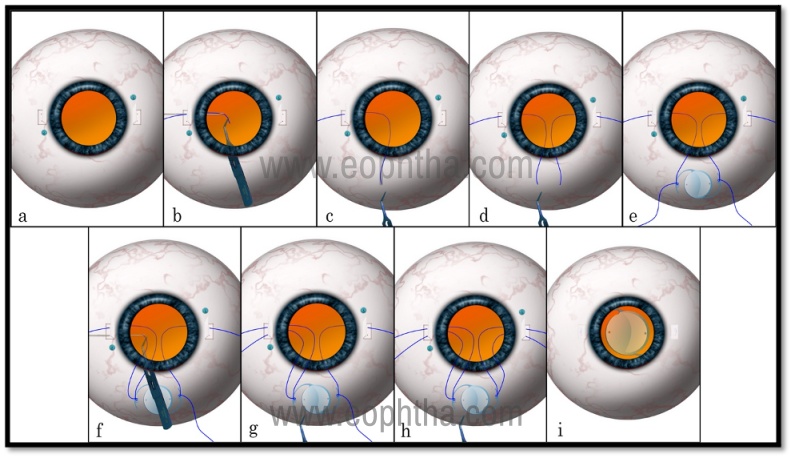
Figure 3: Four point fixation with Gore-tex suture.Partial-thickness scleral flaps are made at 3 and 9 o’clock and 2 each sclerotomies are made under the flaps with 23 G trocar (a). A piece of the Gore-tex suture is cut, held with intraocular forceps, and is passed into the eye under the flap from one of the sclerotomies. It is taken out through the superior section with the help of a McPherson’s forceps (b & c) Similar procedure is done on the other side (d). The suture ends are threaded through the eyelets on both sides (e). The suture end is then passed back into the anterior chamber and taken out under the flap through the second sclerotomy (f). The maneuver is repeated on the other side too (g). The IOL is inserted and the sutures are tied (h & i).
- Partial-thickness scleral flaps or pockets are made 180 degrees apart as usual.
- A 23g trocar assisted scleral entry is made under the scleral flap on both sides of the radial mark keeping the same distance of 1 mm from limbus and the radial mark. Four such entrees are made, 2 on each side.
- A free piece of the Gore-tex suture is cut approximately 10 cm in length. One end of the suture is held with a 25G intraocular end-gripping forceps (used during vitrectomy surgeries) and inserted into the eye from one of the 23G entry points under the flap. (It is easier to insert a thinner 25G forceps through the 23G entry)
- This suture end is grasped with a non-toothed suture holding forceps inserted through the superior corneo-scleral tunnel and brought out of the eye.
- The IOL is threaded through the eyelet and the suture is passed back into the eye through the corneo-scleral tunnel and taken out under the flap with the help of a 25G intraocular forceps.
- The same maneuver is repeated on the other side.
- The IOL is inserted in the eye, positioned in the sulcus while the sutures and tightened. The sutures are tied in a 3-2-1 loop sequence and the ends are trimmed. The flaps can be sutured or glued.
A rigid one-piece IOL from Aurolab which has eyelets on the haptics and has a larger optic with increased overall length suits well for such fixation. It centers well without causing any tilt. But recently IOL materials and designs have been modified to improve success rates and reduce the risk of complications in scleral fixation. For example, newer IOLs such as the CZ70BD (Alcon, Fort Worth, TX) and the Akreos AO60 (Bausch and Lomb, Rochester, NY) which can be inserted through smaller incisions also incorporate suture eyelets, which help to prevent suture slippage and subsequent IOL dislocation.
The Bausch and Lomb Akreos AO60 lens has four haptics, each with its own eyelet for suture passage. The four-point stabilization of Akreos lens theoretically decreases the risk of lens tilt and decentration. However, the Akreos is a hydrophilic IOL and is susceptible to optic opacification due to calcium salt deposition especially following intraocular gas or air fill.6
Recently, a 4-point flanged fixation using 5-0 polypropylene monofilament, has been described by Canabrava et al wherein the ends of the sutures are cauterized and fixed as a 4 point fixation after passing through the IOL haptics.15
Surgical Techniques of Suture-less SFIOLS
In order to reduce the suture-related complications, various techniques of fixating the IOL without sutures have been described. One of the earliest descriptions was by Maggi and Maggi.16 Gabor and Pavlidis described the exteriorization of the haptics of a three‑piece IOL for a sutureless SFIOL fixation.17 Herein, the 23‑gauge trocar or needle can be used to create partial-thickness scleral tunnels parallel to the limbus. These scleral tunnels or pockets are used to house the exteriorized haptics. This technique provided for shorter surgical times and good IOL centration.6 This technique popularly known as the glued IOL has been further modified and perfected by Agarwal et al.18
The glued IOL technique:
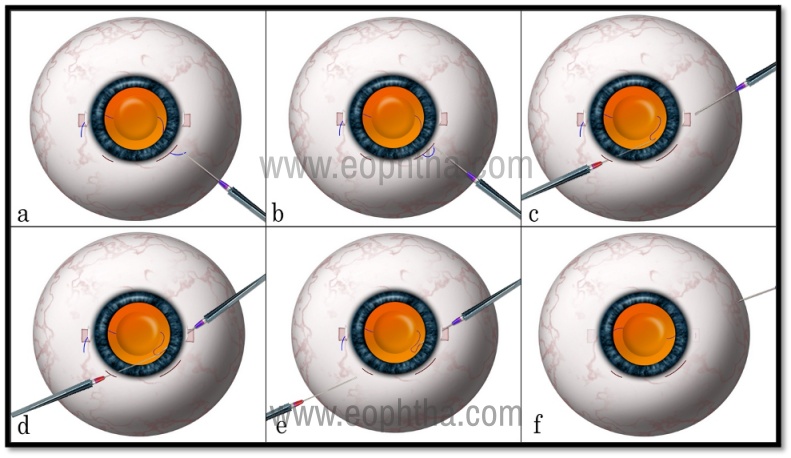
Figure 4: GLUED IOL- Sutureless fixation. Partial-thickness scleral flaps, scleral tunnels, and sclerotomies are made on both sides. A 3 piece IOL is inserted and the leading haptic is exteriorized through the sclerotomy under the flap (a). The second haptic is held with intraocular forceps and passed into the anterior chamber (b). With the help of 2 intraocular forceps, the haptic is maneuvered and taken out through the sclerotomy from the other side (c,d,e). 2-3 mm length of the haptics is tucked into the tunnels on each side and the flaps are glued over it (f).
This technique is shown in figure 4. The main steps are as follows:
- In this technique, partial-thickness scleral flaps are created 180 degrees apart centered on the visual axis.
- 25 G sclerotomies are created under the flaps 1 mm posterior to the limbus corresponding to the horizontal axis marks.
- A 26G needle is used to create intrascleral tunnels of 2-3 mm on either side, parallel to the limbus but facing in opposite directions.
- A 3 piece foldable IOL is inserted through the corneoscleral section with the help of an injector.
- An intraocular end gripping forceps is introduced through the sclerotomy on one side and the leading haptic is exteriorized.
- The intraocular forceps are introduced through the second sclerotomy on the opposite side. The trailing haptic is inserted in the anterior chamber and pulled out through the sclerotomy.
- About 2-3 mm length of the haptics on each side are then inserted into the scleral tunnels and are tucked intrasclerally.
- Fibrin glue is applied to seal the scleral flaps and the conjunctiva.
Transconjunctival, flapless, glueless, and sutureless technique for SFIOL
Recently, Yamane et al described a modification of the glued IOL technique which has become very popular.19 This does not require any flaps or tunnels, is very quick and easy to perform. (see Figure 5)
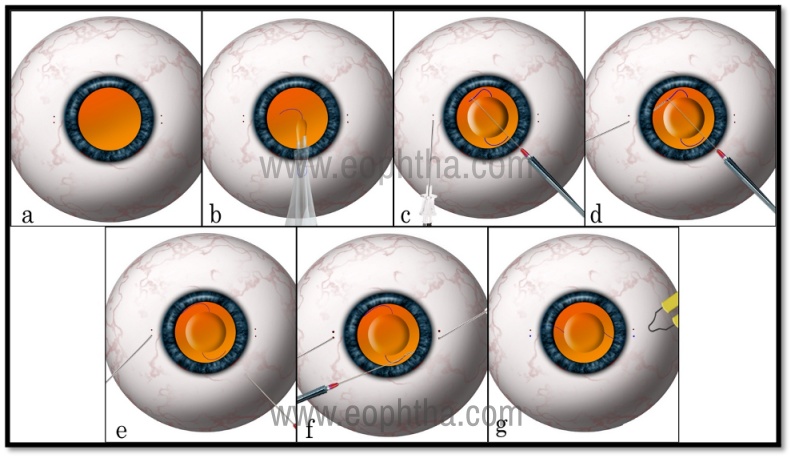
Figure 5: Yamane Technique of transconjunctival, sutureless, flapless, and glueless scleral fixation of IOL Two points are marked 2 mm from the limbus on each side (a). A 3 piece foldable IOL in injected into the anterior chamber (b). A 30 G needle is passed transconjunctivally into the eye from one of the marked points on one side making sure to have a long passage in the sclera and the haptic is docked into the needle (c,d). While leaving the first needle inside the eye, a second needle is introduced from the other side and the trailing haptic is docked into it (e, f ). Both the needles are simultaneously pulled out and removed, leaving the haptic ends out of the conjunctiva. The exposed ends are cauterized to cause a bulbous shape and allowed to retract inside the short scleral tunnel and slide beneath the conjunctiva (g).
- In this technique, a toric marker is used to mark the 3 and 9 o’clock positions.
- The calipers are used to mark the conjunctiva 2 mm from the limbus, with another mark placed 2 mm superior (at 3 o’clock) and 2 mm inferior (at 9 o’clock).
- A standard pars plana vitrectomy and/or lensectomy is performed with cannulas placed away from the above-marked locations
- A keratome fashions a triplanar 3.2-mm clear corneal incision at the superior limbus to inject the IOL in anterior chamber (a scleral tunnel can also be used).
- Two 30‑gauge needles, one on each side, are passed 2 mm from the limbus through the conjunctiva, with an intrascleral length of 2 mm on either side.
- The leading haptic is grasped with micro forceps and inserted into the shaft of the 30G needle on one side.
- The trailing haptic is similarly inserted into the 30G needle on the opposite side.
- Both the 30G needles are then withdrawn and the haptics are exteriorized.
- The tips of the externalized haptics are cauterized. The heat shortens the length of the haptic outside the eye and also creates a bulbous flange whose diameter is larger than the thickness of the haptic.
- This flange is then pushed back so that it lodges within the substance of the sclera and is completely covered by the conjunctiva, thus fixating the IOL to sclera without any sutures, flaps or glue.
Both sutured and sutureless techniques of IOL fixation are being practiced widely. Some authors have compared these two techniques and concluded that both techniques are good, but with a set of complications unique to them and it is difficult to ascertain the superiority of one over the other without large clinical trials.20
Complications:
Intraocular pressure fluctuations have been noted commonly in the immediate post-operative period. Similarly dispersed intraocular bleeding might be seen immediately after the surgery due to the passage of needles through the vascular uveal tissue. These conditions usually settle with conservative treatment and observation.
Cystoid macular edema: The incidence of CME is noted to be around 5-6% after SFIOL and can be seen after 1-3 months after the surgery. In rare instances, it can be seen even after 9 months following the surgery. The incidence is higher in cases where the anterior vitrectomy has been done inadequately. Vitreous prolapse in the anterior chamber or incarceration lead to the development of a CME. The treatment involves nonsteroidal anti-inflammatory drugs and oral acetazolamide. Refractory cases can be treated with intraocular steroid injection.
Lens tilt or decentration: The incidence of a tilt is higher with a 2 point fixation and reduces with 4 point fixation. Even a small tilt of 5 degrees can induce significant astigmatism leading to patient discomfort. Careful marking of the anchoring points placed precisely 180 degrees away would reduce the risk of tilt or decentration.
IOL dislocation: IOL dislocation can occur in either of the techniques. In sutured SFIOLs, a late dislocation has been noted nearly 10-15 years after the initial surgery due to biodegradation of the polypropylene suture and subsequent breakage. It is more common with 10-0 polypropylene than with 9-0 suture. However, the Gore-tex suture is supposedly more resistant to biodegradation and breakage. The risk of IOL dislocation is greatly reduced with the Gore-tex suture. In the case on suture-less SFIOL too, dislocation of IOL can occur. In fact, dislocations have been noted to occur earlier than in the sutured variety. The IOL haptics can slip out from the tunnel and get retracted into the intraocular cavity. None of the currently available IOLs are designed for such kind of scleral fixation. Their overall size is small and the haptics is unnaturally stretched between the two fixation points. Also, the movements of the ocular coats can theoretically dislodge the haptics leading to IOL dislocation.
Retinal detachment: Retinal detachment can occur in about 3-4% of patients. Pre-existing retinal tears in a case of traumatic cataracts can predispose the patient for retinal detachment. But often the cause could be trauma to the vitreous base during suturing. Meticulous removal of the vitreous, especially at the sites of fixation can reduce the risks of retinal detachment.
Other rare complications are endophthalmitis and suprachoroidal hemorrhage.
Complications of SFIOL
- Early postoperative complications: include hypotony, increased intraocular pressure, intraocular bleeding, and cystoid macular edema.
- Late complications are suture erosion, suture knot exposure, suture breakage, haptic exposure, IOL tilt or decentration, IOL dislocation, glaucoma, and retinal detachment.
Pediatric Considerations
Children who need early correction of aphakia and amblyopia, but who do not have capsular support represent a unique population for SFIOL. Although aphakic spectacles or contact lenses are considered as a safe first-line treatment option in children, the unmistakable advantages of an SFIOL over the traditional alternatives make it more preferable.21,22 Similarly children with congenital subluxation of lenses with associated systemic anomalies such as in Marfan’s syndrome show better outcomes with an SFIOL. Various retrospective and longitudinal case series of children implanted with mainly sutured SFIOLs have yielded promising results at follow-ups ranging up to six years.21-23 Special attention has to be paid to the age at which an SFIOL can be performed. It is advisable to wait till at least 6 years of age for the eyeball to attain its final size and reach adult measurements. However, it must be borne in mind that the pediatric population is more prone to complications such as glaucoma, endophthalmitis, IOL decentration/dislocation, suture degradation, myopic shift, and retinal detachment. Therefore the need for a long-term follow-up and a possible need for additional surgery should be well explained to the guardians.22
Conclusions:
SFIOL is a safe and effective treatment option for situations where there is inadequate capsular support for the placement of an IOL. They offer stable, long-term visual rehabilitation. Sutured SFIOLs have been the mainstay until the last decade but with recent innovations, sutureless SFIOLs have come to the forefront offering a faster and easy learning curve for surgeons. Although we await the long‑term results of these new techniques, it is clear that the intraoperative difficulties are lesser with sutureless methods. The choice of IOL and technique will depend on the ocular anatomy and integrity of tissues. Both the sutured and sutureless have a subset of early and late complications that need long-term data comparing the various techniques to identify optimal strategies for SFIOL implantation.
References:
- Por YM, Lavin MJ. Techniques of intraocular lens suspension in the absence of capsular/zonular support.Surv Ophthalmol.2005;50(5):429–462.
- Vajpayee RB, Sharma N, Dada T, et al. Management of posterior capsule tears. Surv Ophthalmol 2001; 45:473–488.
- Madanagopalan VG, Sen P, Baskaran P. Scleral-fixated intraocular lenses. TNOA Journal of Ophthalmic Science and Research. 2018 Oct 1;56(4):237.
- Jacob S, Kumar DA, Rao NK. Scleral fixation of intraocular lenses. Current Opinion in Ophthalmology. 2020 Jan 1;31(1):50-60.
- Sundmacher R, Althaus C. Surgical technical principles of trans‑scleral suture of posterior chamber lenses. Klin Monbl Augenheilkd 1993;202:320‑8.
- Stem MS, Todorich B, Woodward MA, Hsu J, Wolfe JD. Scleral-fixated intraocular lenses: past and present. Journal of vitreoretinal diseases. 2017 Mar;1(2):144-52.
- Yalniz-Akkaya Z, Burcu A, Uney GO, Abay I, Eksioglu U, Acar MA, Ornek F. Primary and secondary implantation of scleral-fixated posterior chamber intraocular lenses in adult patients. Middle East African Journal of Ophthalmology. 2014 Jan;21(1):44.
- Lee VY, Yuen HK, Kwok AK Comparison of outcomes of primary and secondary implantation of scleral fixated posterior chamber intraocular lens. Br J Ophthalmol. 2003 Dec; 87(12):1459-62.
- Price MO, Price FW Jr., Werner L, Berlie C, Mamalis N. Late dislocation of scleral‑sutured posterior chamber intraocular lenses. J Cataract Refract Surg 2005;31:1320‑6.
- Cho BJ, Yu HG. Surgical outcomes according to vitreous management after scleral fixation of posterior chamber intraocular lenses. Retina. 2014; 34(10):1977–1984.
- Malbran ES, Malbran E Jr, Negri I. Lens guide suture for transport and fixation in secondary IOL implantation after intracapsular extraction. Int Ophthalmol. 1986; 9(2–3):151–160
- Lewis JS. Ab externo sulcus fixation. Ophthalmic Surg. 1991; 22(11):692–695.
- Hoffman RS, Fine IH, Packer M. Scleral fixation without conjunctival dissection. Journal of Cataract & Refractive Surgery. 2006;32(11):1907-12.
- Szurman P, Petermeier K, Aisenbrey S, Spitzer MS, Jaissle GB. Z-suture: a new knotless technique for transscleral suture fixation of intraocular implants. British journal of ophthalmology. 2010 Feb 1;94(2):167-9.
- Canabrava S, Lima AC, Arancibia AE, Dornelas LF, Ribeiro G. Novel double-flanged technique for managing Marfan syndrome and microspherophakia. Journal of Cataract & Refractive Surgery. 2020 Mar 1;46(3):333-9.
- Maggi R, Maggi C. Sutureless scleral fixation of intraocular lenses.J Cataract Refract Surg 1997;23:1289‑94.
- Gabor SG, Pavlidis MM. Sutureless intrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg. 2007;33(11):1851-4.
- Kumar DA, Agarwal A, Packiyalakshmi S, Jacob S, Agarwal A. Complications and visual outcomes after glued foldable intraocular lens implantation in eyes with inadequate capsules. Journal of Cataract & Refractive Surgery. 2013;39(8):1211-8.
- Yamane S, Sato S, Maruyama‑Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double‑needle technique. Ophthalmology 2017;124:1136‑42.
- Sindal MD, Nakhwa CP, Sengupta S. Comparison of sutured versus sutureless scleral‑fixated intraocular lenses. J Cataract Refract Surg 2016;42:27‑34.
- Buckley EG. Safety of transscleral-sutured intraocular lenses in children. J AAPOS. 2008; 12(5): 431–439
- Sen P, Kumar V, Bhende P, Rishi P, Rishi E, Rao C, Ratra D, Susvar P, Kummamuri S, Shaikh S, Gopal L. Surgical outcomes and complications of sutured scleral fixated intraocular lenses in pediatric eyes. Canadian Journal of Ophthalmology. 2018;53(1):49-55.
- Caca I, Sahin A, Ari S, Alakus F. Posterior chamber lens implantation with scleral fixation in children with traumatic cataract. J Pediatr Ophthalmol Strabismus 2011;48:226‑31.