

Introduction:
Recurrent corneal erosion syndrome (RCES) is a chronic, relapsing condition first described by Hansen1, who termed it as ‘‘intermittent neuralgic vesicular keratitis.’’ Stood in 1901 suggested that trauma to the corneal epithelium and anterior stroma resulted in an inability of the new epithelium to form normal attachments to the injured anterior Bowman’s layer2.
Despite more than a century of advances in corneal science, RCES remains one of the most challenging conditions to manage3. Most patients have a history of epithelial trauma or associated corneal dystrophy and respond initially to a conservative regimen of lubrication. However, they often experience frequent and debilitating recurrences. In this review, we will investigate the etiology and pathogenesis of this challenging disorder, discuss the histopathological changes with a highlight on ASOCT findings, current therapies, and present future directions for research.
Etiology and epidemiology:
Recurrent corneal erosion (RCE) is a clinical syndrome characterized by inadequate epithelial basement membrane adhesions, resulting in repeated episodes of corneal epithelial defects4. The average age of onset is the fourth or fifth decade, with a slight female preponderance4,5. The interval between the first recurrence and initial abrasion varies from 2days to 16 years9. Pain is the most common symptom followed by the watering of the eye and blurred vision6. The most common site of erosion is usually inferior paracentral cornea6,7,11.
RCES may be either primary or secondary, depending on whether the defect in the epithelial basement membrane is intrinsic or acquired. In the majority of patients with RCES, trauma is the initiating factor, especially trauma from a scratch that damages or destroys the corneal basement membrane6. Epithelial basement membrane dystrophy (EBMD), also called Anterior basement membrane dystrophy (ABMD) or Cogan's Map Dot Fingerprint Dystrophy, and Lattice Stromal Corneal Dystrophy are other non-traumatic causes of RCES.
In women, recurrent corneal erosions often occurred secondary to injury from a baby’s finger10 while in men, occupational hazards were noted to cause injury9. Other reported aetiologies included refractive surgery11, bullous keratopathy, nocturnal lagophthalmos12, meibomian gland dysfunction13 and chemical or thermal injuries14. Further, there are high rates of meibomian gland dysfunction (MGD) and ocular rosacea in eyes with non-traumatic corneal erosion.5 Recurrences commonly occur at the time of awakening10,11,13,15 as poorly adherent epithelium is further loosened or sheared off the cornea by opening of the eyelid. RCES is thought to be precipitated by rapid eye movements during the REM sleep phase16.
Erosions are of two types23- the microform and macroform. Microform lesions, recognized as small intraepithelial breaks, usually resolved within 1–4 hours, and the epithelium was often intact at the time of examination10. Macroform lesions, recognized as large areas of the absent or loose epithelium, resolved on a variable time scale between 1 and 21 days10. Typically, microform erosions occur with spontaneous attacks associated with EBMD whereas macroform erosions are associated with traumatic etiology.
Pathogenesis:
The histopathology of RCES has been studied with light and electron microscopy, and anomalous structural findings have been described in three regions: the epithelium, basement membrane and Bowman’s layer3. The ultrastructural changes which reduce adhesion of the corneal epithelium include a deficient epithelial basement membrane, the absence and abnormality of hemidesmosome, and the loss of anchoring fibrils6. Abnormalities in hemidesmosome formation and function, along with a focal absence of the basement membrane, have been reported in patients with RCES 8,14,20.
Increased levels/activity of several members of the matrix metalloproteinase(MMP) enzyme family, including MMP-2 and MMP-9 have been reported in patients with recurrent erosion17,18. In the post-traumatic setting, upregulation of these components is thought to lead to basement membrane degeneration, aberrant epithelial basement production and poor epithelial adhesion3.
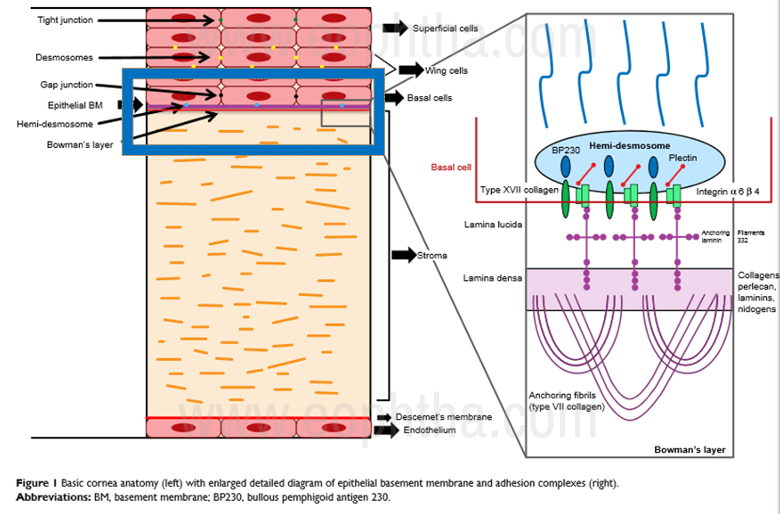
The figure above (Fig.1) explains the different layers of the cornea and highlights the ultrastructure of the adhesion complex. Histologically, the epithelium was extremely thickened and pale, secondary to intercellular and intracellular edema22. Hemidesmosomes were reduced or absent in the area of pale epithelial cells. Intraepithelial extension of redundant basement membrane wear seen. Basement membrane complexes were frequently discontinuous, and a decreased number of anchoring fibrils was noted21.
Diagnosis:
RCE is diagnosed based on clinical signs and patient history. A history of recent and remote trauma to the involved eye, recurrent episodes of pain on awakening, and a loose, ragged, greyish-staining area of the epithelium with greyish deposits +/- epithelial defect (Figure 2) constitute major diagnostic criteria6. A detailed slit lamp examination should be performed with fluorescein staining and retro-illumination, and the fellow eye should be examined for signs of basement membrane dystrophy4.
If the examination does not reveal obvious epithelial defects, an adhesion test can be done to assess for inadequate epithelial-stromal adhesion. A dry cellulose surgical sponge is gently passed over the area of the suspected epithelium. If the intact epithelium is movable, the adhesion test is positive24.
Other investigations that can help in the diagnosis of RCES include video-keratography, confocal microscopy and ASOCT. The surface asymmetry index (SAI: the measure of the difference in corneal power at every ring 180_ apart, over an entire corneal surface covered with rings) and the surface regularity index (SRI: the measure of local fluctuations in central corneal power, a circle of 4.5-mm diameter around the center of the entrance pupil) may be considerably increased in those eyes with RCES25.


Figure 2: Clinical presentation of Recurrent Corneal Erosion
In this modern era of non-contact investigative modalities, ASOCT holds significant value in the diagnosis of RCE (Fig 3). Characteristic changes are seen in the anterior layers of cornea mainly the epithelium, basement membrane, Bowman’s membrane, and anterior stroma. The basement membrane- Bowman’s membrane junction (BM-BM junction) which is the main site of the anchoring complex, where the pathology lies, shows characteristic features like hyperreflectivity, surface irregularity, thickening, and slit-like spaces. Undetected basement membrane, anterior stromal hyperreflectivity, and epithelial changes like hyperreflectivity, edema, irregular breaks, and intraepithelial inclusion cyst are also seen in most patients with RCE.
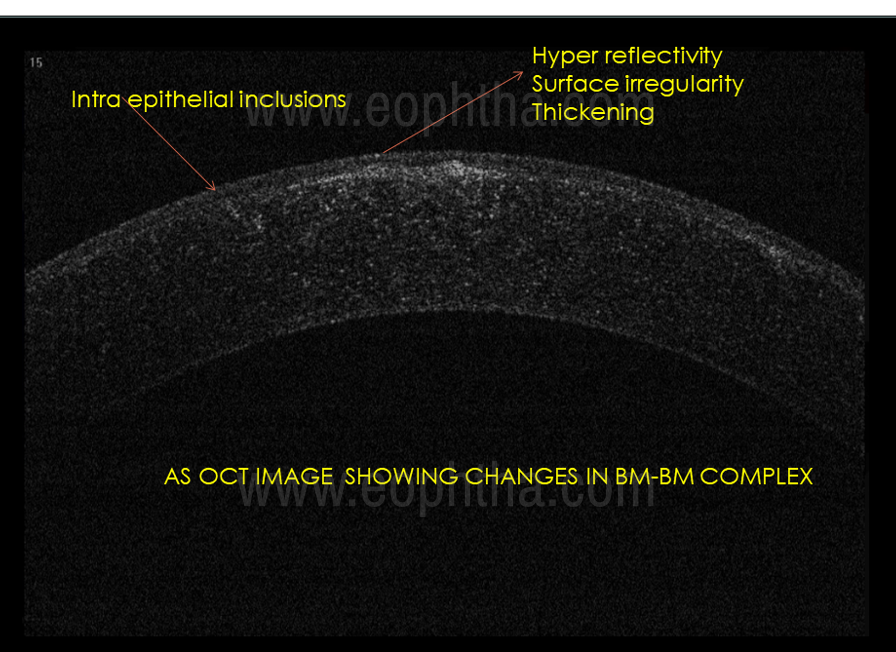

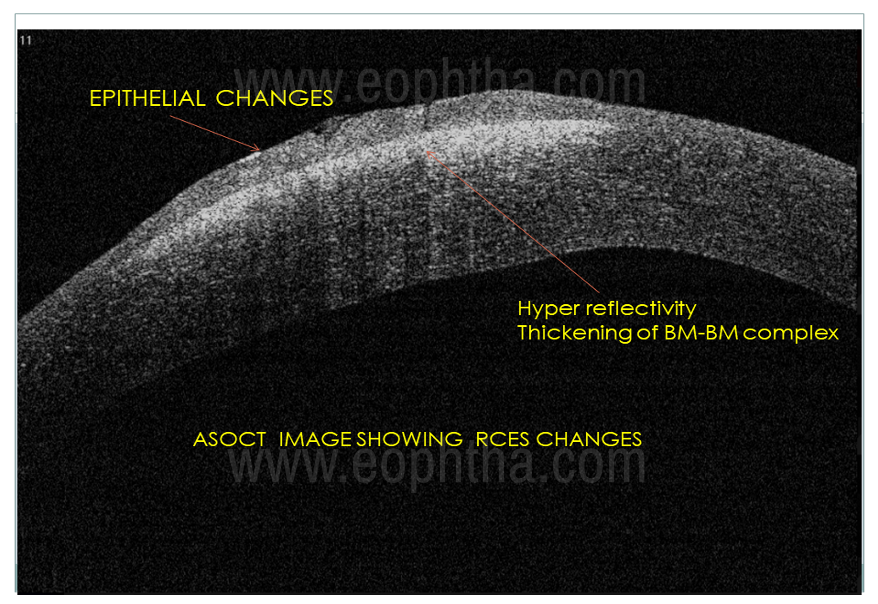
Figure 3: ASOCT images showing different features of RCES in different layers.
Treatment:
The two primary therapeutic goals for RCE are to facilitate rapid re-epithelialization and relieve pain. A secondary goal is to prevent future occurrences of erosion. The basic principle of treatment of RCES is to increase the adhesion of the epithelium to the underlying stroma. This may be due to the increase of hemidesmosomes and anchoring fibrils or due to the promotion of fibrosis6.
Historically, a plethora of therapeutic options have been tried to alleviate the symptoms and prevent the recurrences like antiseptic ointment26, fresh chlorine water27, hypertonic ointment with pressure patching28, iodine cautery29, hypertonic dextran polysaccharide solution30, etc. Current management of RCE can be broadly divided into medical management which is used as first-line for acute presentations and surgical management which aims to treat the pathology and treats recurrences permanently.
Medical management:
1) Lubrication with drops, gels, and ointment with or without patching and cycloplegia. This was was shown by Reidy et al to be effective in the short run in about 50% of patients,5 the other 50% required surgical intervention long term for recurrent erosion7.
2) Bandage contact lens (BCL) The bandage lens is thought to allow time for normal epithelial anchoring to take place, protected against the frequent microtrauma of rapid eye movement and blinking. A period of six weeks is considered to be the minimum period for lens wear on the basis of time taken for epithelial basement membrane remodeling. Studies show the advantages of BCL like recurrence-free patients at 1 year31 and an increase in the speed of symptom resolution32. Extended wear contact lenses carry a risk of infection33-35 and a topical antibiotic is recommended during the duration of therapy. It should be tried after the primary modalities of treatment have failed6. It has been found that recurrences are fairly common in dystrophic cases after the removal of the lenses.
3) MMPase inhibitors as MMP2 and MMP9 have been found to be upregulated in the tears of patients with traumatic corneal abrasions and recurrent corneal erosions. Hence, doxycycline which inhibits MMP936 has been reported to be effective. This produced rapid resolution and prevented further recurrences36. Hope-Ross et al reported that the combination of oral tetracycline and corticosteroid drops was helpful in the treatment of recalcitrant RCES37.
4) Autologous serum treatment (AST) Autologous serum is largely similar in composition to that of tears and provides the ocular surface with basic nutrients for epithelial renewal50. AST as second-line therapy for RCES in eyes failing conservative measures has been evaluated in various studies38,39. It was administered 6times a day for 6weeks. AST is mostly safe, with a mild risk of infection, and should be used in conjunction with topical antibiotics.
Surgical management:
1) Anterior stromal punctureit involves the utilization of a small gauge needle to create micro-punctures through the abnormal epithelium in RCES into the anterior half of the stroma40. It was believed that the breaching of Bowman’s layer stimulated a more secure bonding of the epithelium to the underlying basement membrane, Bowman’s layer, and stroma. Most of the patients had faint residual scars, which was visually insignificant.
The advantages6 of ASP over PTK include the following: (a) it can be easily performed in the office setting with simple equipment; (b) it has a low risk of inducing visually significant scarring and changes in refractive power; (c) it causes only minimal discomfort. However, if performed over the pupil, ASP may induce multifocal scars and irregular topographic changes.
2) YAG laser stromal micro-puncturefirst time used by Geggel41, this procedure allowed for more reproducible, translucent scars. Nd: YAG laser was focused at the basement-membrane zone after epithelial debridement.
3) Phototherapeutic keratectomy (PTK) as per a study42 subjects treated with PTK for RCES, 72% did not experience any recurrence for the 5–10 years of their follow-up. The success rate ranges from 74%-100%. The disadvantages of PTK include hyperopic shift, scarring, and pain. Treatment of recurrent erosions due to trauma has a higher success rate than treatment for corneal dystrophies51. Retreatment with PTK appears to be successful for patients with macro-erosions complicating RCES who failed conservative management with ocular lubricants and a primary PTK49. An alternative is transepithelial PTK, where the laser ablation starts at the superficial epithelial layer52. Potential of hyperopic shift following PTK53,54 has been associated with axial ablation to remove anterior stromal pathology and ablation depths many times greater than that used for the treatment of RCES. Subepithelial PTK should be tried in those cases who failed to respond to conservative modes of treatment and application of therapeutic contact lenses6.
4) Epithelial debridement/diamond burr polishingThe epithelium was removed with a Weck-Cel sponge and #57 blade, and a 3.3 mm diameter diamond burr was used to ‘polish’ the stromal surface for approximately 30s43. A significant improvement in symptoms, visual acuity, and topographical astigmatism was seen. Subepithelial haze remained a complication of this procedure, with a cumulative 26% incidence44,45.
5) Alcohol delaminationa circular well is placed on the cornea with the patient supine, and the cornea is exposed to ethyl alcohol for approximately 40–60 s. The alcohol-loosened epithelium is then removed with a cellulose sponge and Beaver blade, and the epithelium allowed to heal. This therapy is designed to separate the epithelium at the level of the superficial basement membrane without disrupting Bowman’s layer and leave a smooth surface for the epithelium to reattach. 75% of patients were symptom-free for a follow up of 2years46. A randomized control trial comparing PTK to alcohol delamination showed similar outcomes with both47. Pain is a primary drawback of any technique that removes the corneal epithelium.
6) Botox to orbicularis muscle/tarsorrhaphy In severe recalcitrant cases of RCES, Botox has been injected into the orbicularis muscle to induce ptosis to protect the ocular surface48.
Complications:
Complications of RCES are infrequent but may include non-infectious anterior uveitis and stromal scarring. It is important to note that RCES is a relative contraindication for LASIK because of the high risk of DLK post-LASIK due to spontaneous intraoperative erosion. Patients with EBMD are better dealt with PRK than LASIK because of the high risk of DLK.
Conclusion:
To conclude RCES is commonly encountered in ophthalmic practice, most commonly after a superficial corneal trauma, especially a scratch. Presents frequently with active and quiet phases causing a diagnostic dilemma to the ophthalmologist. Various treatment modalities have been tried to alleviate the symptoms as well as to prevent further recurrences. We recommend excimer laser PTK, Alcohol assisted delamination or anterior stromal puncture for eyes with four or more episodes of attack of traumatic or dystrophic origin after unsuccessful medical management for at least two weeks.