
History :
While writing about the instrumentation of retinal surgery, the first name came in my mind was the none other than the Jules Gonin, who not only identified the Retinal tear as a prerequisite for the retinal detachment in the way back in 1904 in his first paper with series of 3 cases but also described the management of the same later on after constant hard work over the next two decade. He made major contribution and impact in the field of retinal surgery, immediately after his major presentation at the International Congress of Ophthalmology in 1929, and hence it is worth starting the topic recalling him.
From the Gonin era to date, there were three major events in terms of development. 1st – improvement in instrumentation used to evaluate vitreoretinal pathology. 2nd – Evolution of the methods to create a chorioretinal adhesion around retinal breaks. 3rd – the development of a variety of techniques to tackle the vitreoretinal adhesion and hence to close the break permanently. In this write-up, our discussion is mainly focused on instrumentation used in vitreoretinal surgeries.
Begining of vitreous surgery
The real beginning of the vitrectomy started with an open sky approach with the cellulose sponge, developed by Kasner, and was primarily used for vitreous complications of cataract surgery and occasionally for the removal of opaque vitreous through a keratoplasty wound.
Banko (one of the partners of Kelmen during their work on developing the phacoemulsification machine) patented a vitreous cutter, including aspiration and infusion, but this was never commercialized.
It was an era of basic invention, fewer resources, and limited technology hence took almost a half-decade in the development of instrumentation and closed vitrectomy after Gonin provided the basis for the successful management of retinal detachment. Pioneering work by Robert Machemer made it possible to address the surgical treatment directly via the transvitreal route. For the transvitreal approach, there were basically three requirements. 1. Visualization of the vitreous – illumination system. 2. Removal of vitreous – cutting with aspiration function 3. Replacement of excised and removed vitreous with a clear physiologic solution - Infusion. Considering the basic three need, 1st vitreous full functioning probe came into reality with efforts of none other than Robert Machemer. The Vitreous infusion suction cutter (VISC) developed by Robert Machemer & Parel and the Roto extractor - developed by Douvas, were single port, large incision, so-called full function, slow speed, rotary, electric cutters with aspiration provided by a syringe operated by the assistant. The tip of such a vitrectomy probe was around 2.2 – 2.5 mm in diameter and was in need of pars plana incision of a size larger than 3 mm. Later on, these four instrumental functions are divided among different probes and cannulas of the same diameter. The cutting and aspiration in one probe, illumination with fiberoptic source in other probes, and infusion are provided with a separate cannula. This divided system was advantageous not only because of reduced tip diameter of each instrument to 0.9 mm but also in man other ways like - improved visualization from the different angle in the quadrant of the interest, different angle accessible for difficult intraoperative manipulation and continuous infusion even during temporary withdrawal of the cutter or instruments.
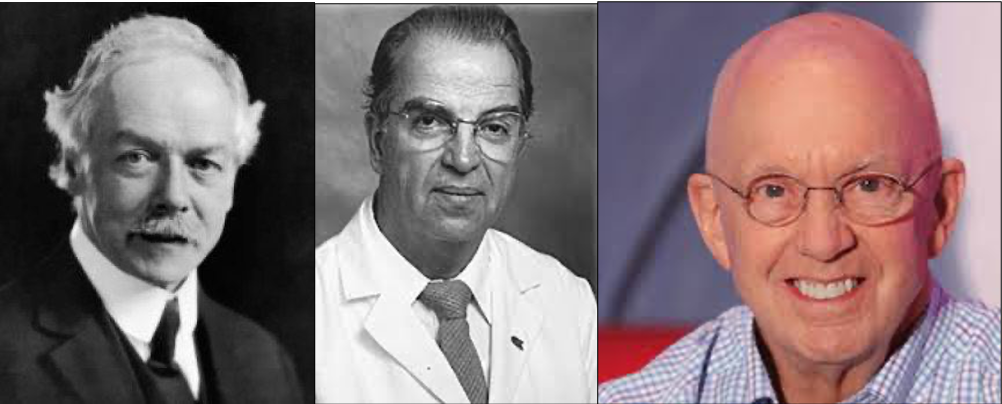
Figure 1:Jules Gonin, Robert Machamer, Steve Charles
In 1974, Ocutome 800, developed by Berkley bioengineering with Conor O’Malley and Ralph Heinz, which became the basis of the modern vitrectomy with its three-port, 20 gauge (0.89 mm) system with the first lightweight, pneumatic probe with axial cutting and surgeon foot pedal controlled on-off aspiration.
Peyman developed the electric solenoid driven axial (guillotine) cutter at about the same time. Steve Charles described internal drainage of fluid in 1973 and McEwen developed the air pump which replaced using a syringe for fluid-air exchange. The air pump produced a controllable intraocular pressure.
Carl Wang and Steve Charles developed the first power gas injector and first power silicone injector.
The Coopervision, which had acquired the original Berkley Bioengineering subsequently developed Ocutome 8000, with the efforts of Carl Wang, Steve Charles, and their engineering team. They also developed the first linear proportional aspiration system, an integrated light source, and a connected fragmented. The MidLabs MVS system, developed by Carl Wang and Steve Charles had the first disposable pneumatic cutter.
Foundation stone of MIVS :
In the 1980s, Visitec introduced the first 23 gauge cutter for vitreous biopsy. In the year 1990, Eugene DeJuan & Hickingbotham developed 25 gauge vitreoretinal instruments like vitreous cutter, vitreous membrane dissector, and microforceps. In 1995, Stanley Chang and the group introduced the 23 gauge system. However, these 25 and 23 gauge systems were not adopted by the industry at that time for various reasons.
Further progress in MIVS :
In 2002, the 25 gauge sutureless entry-site alignment system was modified and reintroduced by Fujii and co-workers followed by a modified 23 gauge system in 2005 by Stanley Chang and Claus Eckhardt with which era of MIVS started.
Current State of MIVS :
After the introduction of the Ocular Connection machine(OCM) in the vitrectomy machine by Steve Charles, the machine became more user friendly with almost all answers in one. The central design concept behind the OCM was ‘systems integration’. One large display with reconfigurable smart keys surrounding it with different functionality depending on the selected mode and one power supply, one housing, and one reconfigurable foot pedal instead of multiple small single-function boxes each with a power supply, foot pedal, and a tiny display gave it popularity. Innovision lead by Steve Charles introduced it 1st, which never commercialized, but latter Alcon acquired innovision and launched 1st OCM based Vitrectomy machine – Accurus and latter on more fine-tuned Constellation came in the market.
Recent advances in MIVS :
Initially, MIVS became popular only in simple vitrectomy cases and bending of the instruments during manipulation due to thinner and thinner instrument was a major challenge, recent development in technology make it possible to have a stiffer instrument of same size and diameter and hence the same 25guage is now a day preferred even for the difficult surgeries including ROP surgeries. Recently 27 gauge (0.40 mm) system has evolved with further improvements in instrument design and function. Even 29 gauge vitrectomy system is also there in the pipeline.
Extraocular procedure
Instruments for peritomy and conjunctival closure
Speculum: In the present era, the extraocular procedure includes mainly encirclage with or without scleral buckle, and hence exposure of muscle insertion site is crucial. Hence, stout, Open bladed, Self-retaining speculum are preferred one. Most commonly used once are Clark’s/William’s universal speculum.
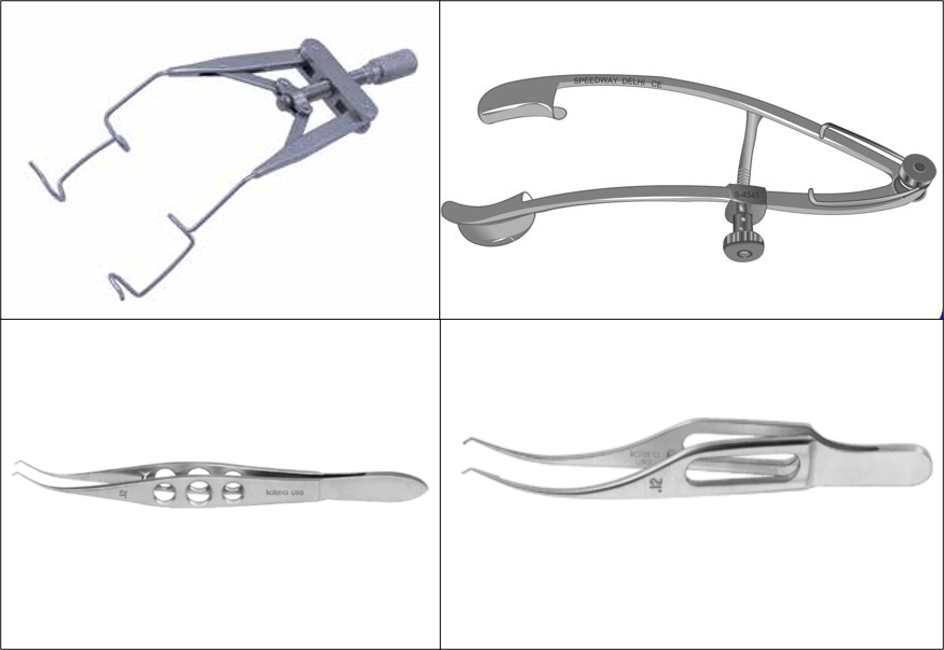
Figure 2: Self-retainingspeculum, Colibri/Lim’s forceps
Pierse - Hoskin/Barraquer - Colibri forceps: These are the most commonly used atraumatic tooth forceps used to hold conjunctiva and/or tenon’s capsule.
Westcott Scissor: It has a standard blade with a blunt tip. It is used during 360 peritomy.
Stevens tenotomy scissor: It is used mainly for posterior tenon’s dissection, especially during scleral buckling surgery. It is available with a curved blade also to follow the curve of the globe easily.
Alabama utility forceps: Tying platform of the long tip of this forceps makes it easy for firm grasping of the suture material and hence secures the tight knot.
Barraquer/Castraviejo microneedle holder: Simple microneedle holder used in suturing during any ophthalmic surgery.
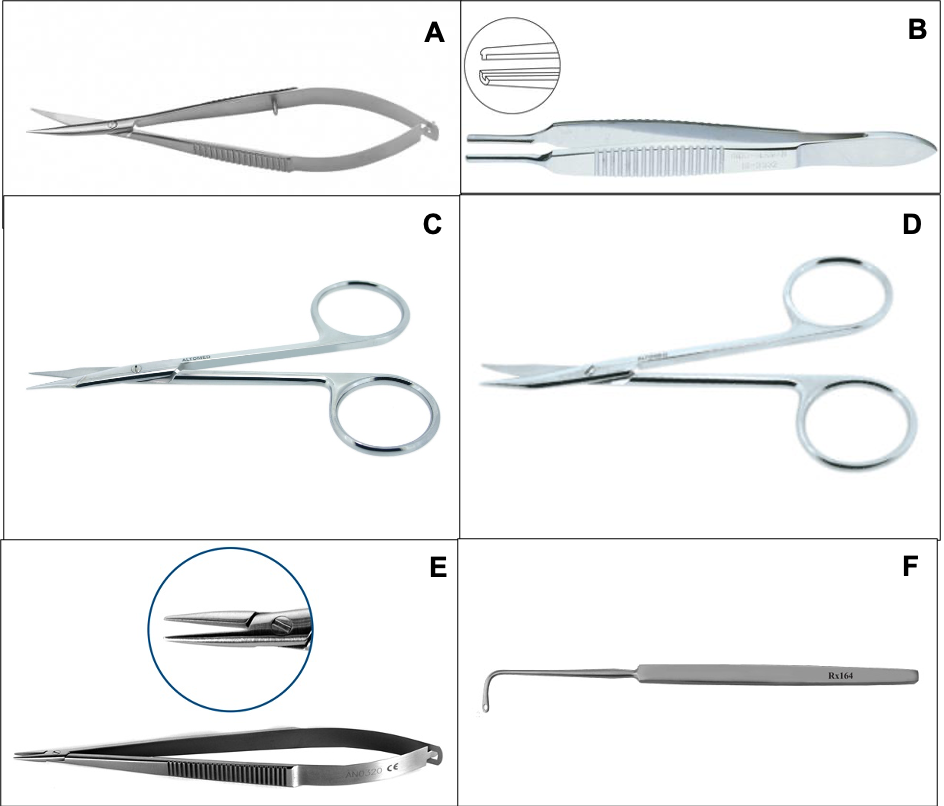
Figure 3:A. Westcott, B. Alabama C, D. Stevens tenotomy - Straight, Curved, E. Barraquer microneedle holder F. Gass muscle hook
Scleral buckle/Encicrclage
Gass retinal detachment hook: Isolation and tagging of the muscle during encirclage or scleral buckle is a primary step. The Gass retinal detachment hook is preferred one due to the presence of eyelet at the tip of the hook through which a bridle suture may be passed conveniently and withdrawn under the muscle with ease. Graefe muscle hooks lack an eyelet and a needle with the bridle suture may need to be passed separately under the hooked muscle.
Schephen’s forked retractor: To retract periocular tissue from the sclera during scleral buckling surgery. Forked tip gives way for the muscle at the same time achieving tissue retraction.

Figure 4: Castraviejo’s calipre
Castroviejo’s caliper: It is the most commonly used caliper to measure the incision site or suture site or pars plana sclerotomy site on the sclera. However, it actually gives chord length and hence can be erroneous at long measurement. Amsler caliper is the preferred one which actually measures the circumference.
Arruga’s/carl’s/Silcock’s needle holder: Basically all of them have a catch(Lock) and hence having the self-retaining capacity and used for heavier gauge needles (Thicker than 6-0).
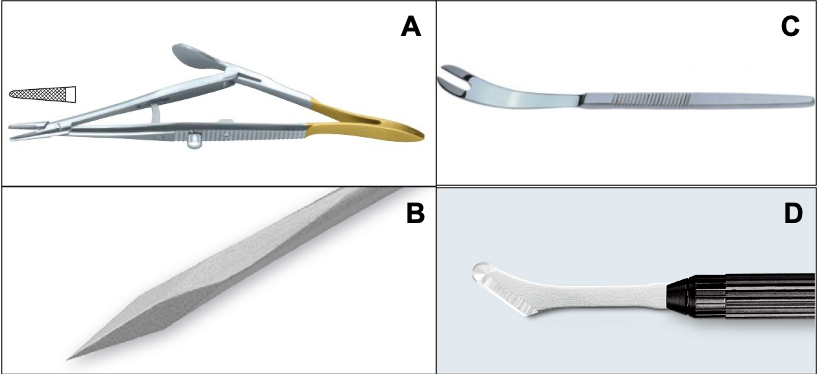
Figure 5: A. Arruga’s/carl’s/Silcock’s needle holderB.Schepens’ retractor, C.MVR blade D.Scleral knife/Dissector
Scleral knife/Dissector: Hockey stick shaped knife with a single outer edge having a width of 2.4 mm. Because of its shape, it is popularly known as ‘Hockey stick knife’. 2.6mm Cresent knife of cataract surgery set can be used as an alternative.
Trans sclera Cryoprobe: Cryotherapy results in aseptic inflammation from thermal injury, later resulting in the formation of chorioretinal scars. Cryotherapy is based on the Joule-Thompson effect: a change in temperature of the gas on sudden changes in volume and pressure. At room temperature, gases cool on expansion.***
Gases with a high positive Joule-Thompson coefficient have a greater temperature drop for a given pressure change. Nitrous oxide among all having the highest Joule Thompson coefficient and hence having the highest temperature drop makes it gas of choice for cryotherapy.
Intraocular procedure – Vitrectomy
Basic instruments in vitrectomy
Micro Vitreo Retinal (MVR) blade: Lancet shaped sharp instrument available in all gauges ranging from ancient most 19G to recent 27 gauge of MIVS. In pre-MIVS era, it was the first instrument used to create a pars plana entry and hence was an essential instrument in any vitrectomy surgery. After the introduction of the trochar-cannula set in MIVS, the role of this instrument is mainly limited. Presently its mainly used to elevate the edge of ERM or membrane or for puncturing and elevating edge of the ILM or fibrous capsule around RIOFB.
Infusion cannula: initially in 20G vitrectomy system, the infusion cannula was a slender metallic holo tube with a grooved collar. The grooved collar was used to put the suture to fix the cannula with the sclera. Originally, infusion cannula was available in 3 different lengths of 2mm, 4 mm, and 6 mm. Most commonly used infusion cannula were of 4 mm length, however, 6 mm long cannula were also designed to tackle special situations like vitrectomy in presence of thickened choroid or choroidal detachment. In MIVS, The infusion cannula fits through the microcannula array and hence there was the elimination of the collar from the design and there was the introduction of sliding lock design on the outer surface to ensure snug tight-fitting.

Figure 6: Infusion canula A. 20G B. MIVS – 23/25/27 G
Eckardt/Reichel-Chun pressure plate: it is a fixation plate with a 3.5 mm radius slotted circular plate with atraumatic teeth on the under surface. Depth of the slot will act as an incorporated caliper to measure the distance between the limbus and trocar entry site, while serrations on the under surfaces allow a good hold on the conjunctiva for misalignment over the proposed scleral entry. Dugel modification allows the pressure plate forceps to make a biplanar incision.
The Thornton or Shepard fixation ring has also been utilized for globe stabilization during trocar insertion.
Trochar-cannula :
The most important development of small-gauge vitrectomy was the introduction of a trocar-cannula system. Trochar-cannula rests inside the sclera and provides an easy introduction of instruments, it protects the sclera against direct injury through the instruments, and entry site with a trochar-cannula system is much easier to find than a usual sclerotomy. The disadvantage of the trochar-cannula system compared to the usual sclerotomy is the excessive leakage of fluid through the cannula during the exchange of instruments. To cop up with that, later on, the valved trochar-cannula system came into light. The valve maintains the globe as a close chamber and hence stable fluidics is achieved continuously with the low fluid infusion. Valves prevent the incarceration of vitreous into the trochar-cannula and hence in sclerotomy. Valves build up a higher intraocular pressure, which is useful during a fluid–air exchange or removal of a preretinal oil bubble; and reduce the need for plugs. The presence of the valve in the cannula makes the entry of the silicone soft tipped instrument difficult. Valved cannula should be avoided during the removal of silicone oil. It is important to check the tip of the trochar cannula under the microscope before using it for sharpness and to rule out the bent tips in view to achieve self-sealed sclerotomy.
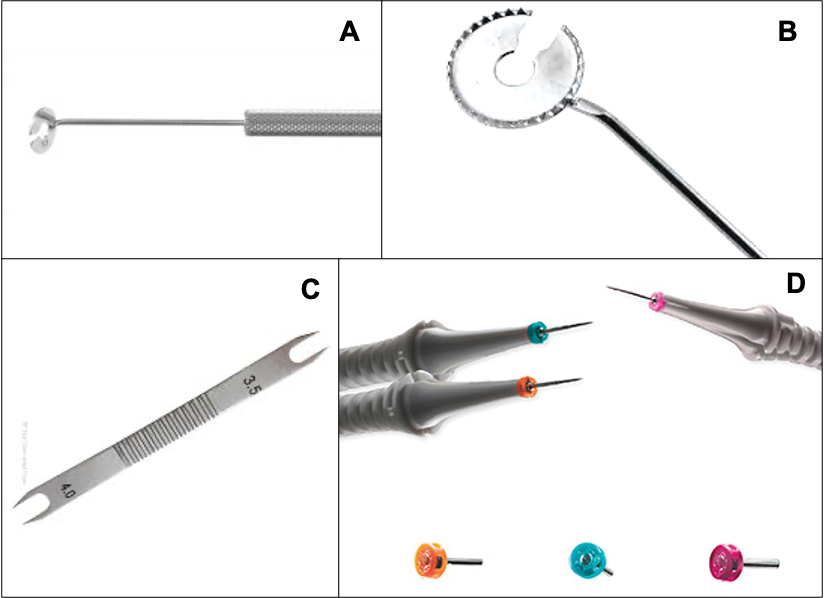
Figure 7 A, B: Eckardt/Reichel-Chun pressure plate C: Braunstein fixed caliper marker D: Trochar - Canula
Braunstein fixed caliper marker: Its a caliper made specifically for vitreous surgery having peaked both ends with 3.0 mm distance at side and 4.0 mm distance at other side.
Plugs: The cannula plug is used to seal the cannula after insertion into the eye wall. It is designed with a tapered shaft or a tight sliding fit to seal within the cannula port. The plug should be inserted only as far as necessary to seal the cannula. Forcing the plug too far within the cannula may cause problems during removal. Even with proper plug insertion, counter-force should be applied to the cannula hub when removing a plug. With the invention of the valved cannula, there is a significant reduction in the use of the plug during surgery.
Plug removal forceps: Specialised forceps having cross action with the groove at the tip to hold the plugin the proper position for insertion as well as removal.
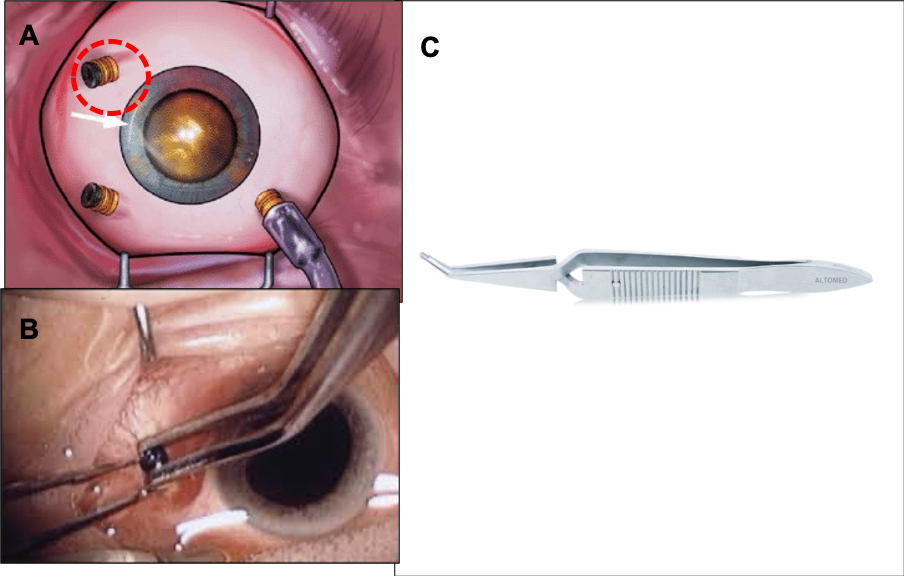
Figure 8: Plugging accessory: A, B -Plugs, C -Plug forceps
Vitrectomy cutter: it is the single most important essential during even the smallest vitreous procedure like Vitreous biopsy and hence it is the instrument that had undergone several modifications from its introduction as a VISC in the 1970s to till the date. This modification were numerous in several ways, such as the cutter size, cutting speed, port geometry, blade design, duty cycle, a propulsive mechanism for the diaphragm/piston, etc. The main objective and goal were to convert high-performance skills demanding surgery into safe and more successful vision rewarding surgery.
Electric cutter: The initial vitreous cutters utilized brush-type direct current (DC) motors for the movement of the diaphragm/piston. Being an electrical motorized, they were too costly to be disposable. The electric motor was also contributing rotary movement known to cause some amount of traction and the weight and size of the motor were making the instrument somewhat bulkier.
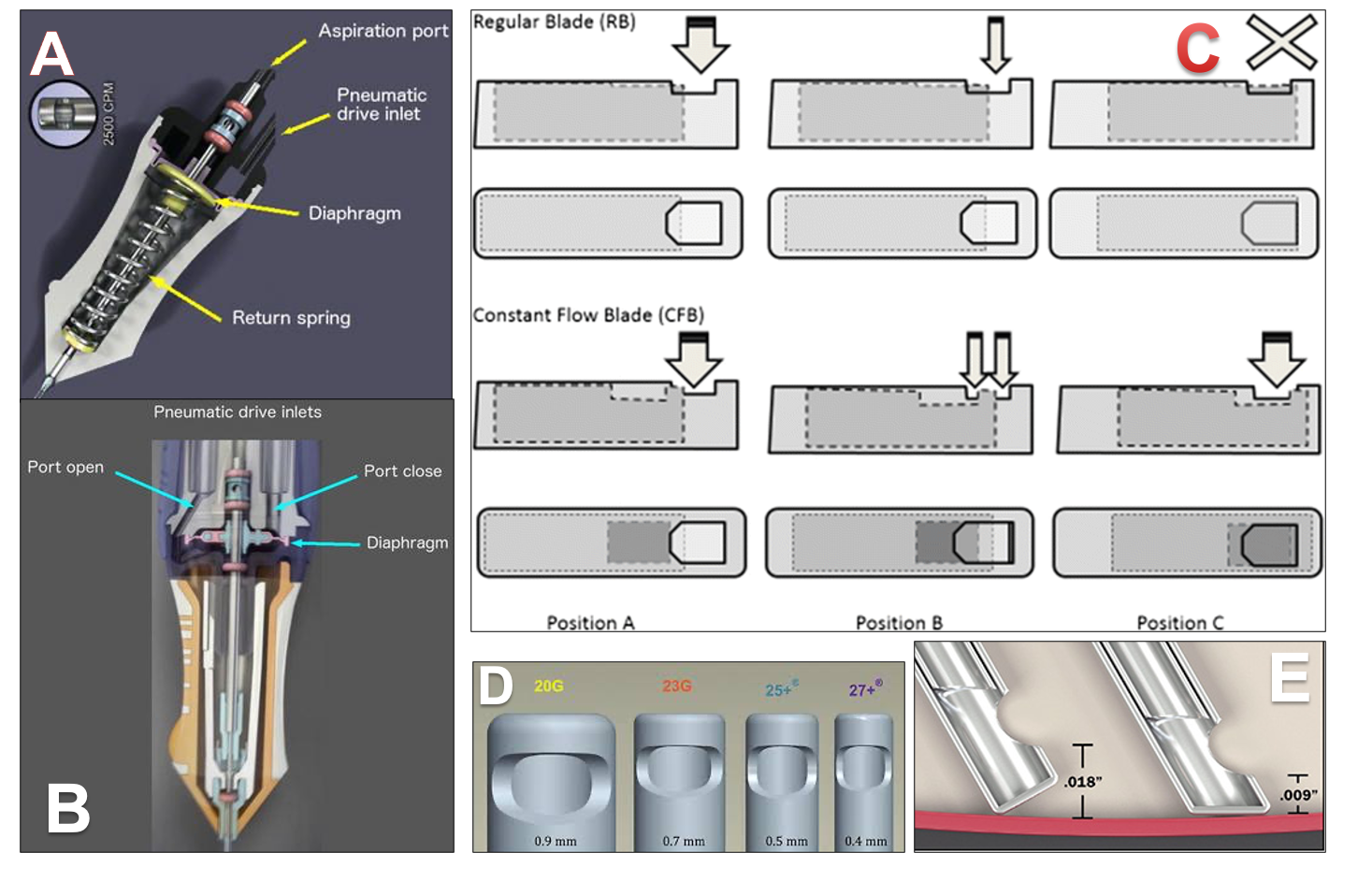
Figure 9: Image about Vitrectomy cutter: A. Mechanism of Pneumatic spring cutter B. Mechanism of Doble Pneumatic cutter C. Mechanism of TDC/CF cutter D. Tip port relationship of cutter E. reduced tip port relationship in the bevelled tip of the cutter
The pneumatic spring return is driven vitrectomy cutter: An air pulse pushes down the diaphragm located inside the vitrectomy probe, leading the port to a closed position (the guillotine movement); at the same time, a spring is compressed and forces the diaphragm back to the open port position. The biggest advancement was that pneumatic cutter were significantly lighter in weight and having a significant reduction in rotary gullitone movement to avoid traction. Limitation of this was, as cut-rate increases the duty cycle decreases to some degree over all the gauges, and hence individualization of cut-rate and duty cycle was not possible. InnoVit was the 1st version of this.
Double pneumatic cutter: Instead of using a spring to return the guillotine to the original position, the dual pneumatic probes use separate airlines to both open and close the vitrectomy port. Advantage of this modification is, this allows the duty cycle to be controlled independently of the cut-rate with customized modes, for e.g. “port biased open” or core mode (the port remains open for the majority of the time), 50/50 mode (the port is open***
Twin duty cycle (TDC) cutter: Claus Eckardt and Mitrofani Pavlidis, in conjunction with DORC, have developed a double-port two-dimensional cutter, formerly known as twin duty cycle (TDC) available in 23, 25 and 27-gauge, which features a larger rectangular aperture in the piston/inner lumen, with two sharp cutting edges. Aperture in the piston allows continuous and even flow due to the two open cutting ports. Two sharp edges over piston allow cutting vitreous in a forward and backward movement during each cycle, effectively doubling the cutting speed. The vitreous cutter has a cutting rate of 8000 cuts/min. But the actual cutting rate with two cutting blades is 8000 × 2 = 16,000 cuts/min, which itself is a new dimension. This novel technology reduces vitreous traction, decreases surgical time, and increases the safety of surgery. TDC cutter has 1.5× to 1.75× higher performance than a regular cutter, resulting in a faster core vitrectomy.
Endoilluminator: It is again the second important instrument as an internal reflection of light within the vitreous cavity won’t allow the microscope light to enlighten the retina. Constant use of adequate illumination via light source throughout the surgery also induces localized thermal changes and hence Spectrum of light used in light source, efficacy, safety, life of light source were few among the many important driving force for constant advancement in this instrument.
A halogen lamp: It has a long lifetime without darkening due to the halogen cycle. The spectral irradiance of halogen lamps has a peak of 650 nm. The retinal hazard with halogen light is less than any high-intensity discharge lamp (The hazard efficacy: 1,920 lumens /hazard watt).
Metal halide lamps: These are high-intensity discharge lamps. The compact arc tube contains a high-pressure mixture of argon, mercury, and a variety of metal halides. The argon gas in the lamp is easily ionized and facilitates striking the arc across the two electrodes when voltage is applied to the lamp. The heat generated by the arc then vaporizes the mercury and metal halides, which produce light as the temperature and pressure increase. The mixture of halides affects the nature of light produced, influencing the color, temperature, and intensity (making the light more blue or red). The spectral output has two peaks at 550 nm and 580 nm. The hazard efficacy is 1,343 lumens/hazard watt.
Xenon lamps: They are high-intensity discharge lamps. Pure xenon short-arc lamps have a “near daylight” spectrum, i.e. the light output of the lamp is relatively flat over the entire color spectrum. To reduce phototoxicity due to ultraviolet and blue light, short-wavelength 420 nm/435 nm filters and for infrared light, 650 nm/700 nm filters are used. The luminous efficacy ranges from 277–355 lumens/watt. The hazard efficacy is 1,913 lumens/hazard watt.
Light-emitting diode lamps: This relatively new light source offers several advantages. The LED produces “near daylight” like light, produces less heat, is more compact, and has a very long life(Available in DORC EVA). It is so much compact that, it can be directly fixed in the probe and obviating the need for a separate lightbox and fiberoptic cable. It has two spectral peaks: 455 nm and 565 nm. The proportion of harmful blue light is low as compared to xenon light source, with or without 435 nm filter.
It is not only the source of light that had undergone advancement but also the type of fiber optic used and light probe too are important aspects. There are various types of light sources available nowadays.
Straight: projects a narrowly focused beam, yielding an enhanced Tyndall effect. It is useful for vitreous identification.
Bullet type: projects a wide field of highly scattered light that is ideal for diffuse surface illumination and panoramic fundus view.
Shielded light pipe: A small hood is designed to be placed over the bullet tip, so that glare toward the surgeon can be reduced.
Wedge type: provides a hybrid illumination with both focal and wide-field illumination characteristics due to an asymmetric light cone. On the other hand, it compromises on the transmitted light, providing only 40–55% of the illumination seen with the bullet or straight probe. These probes are available in different tip angles (30, 45, 60° wedge).
The bullet and 30° wedge probes provide the largest illuminated surface area, while the straight project the narrowest beam. Backscatter or surgeon glare is maximum with the bullet probe, followed by straight and significantly lower with wedge-type aperture. Therefore, wedge-shaped light pipes are advantageous in vitreous base shaving, membrane peeling, laser and for maneuvers performed superiorly and underneath surgeon’s nondominant hand.
Chandeliar illumination system: A chandelier light provides a panoramic light source and illuminates the entire fundus. It is fixed as a fourth port. A chandelier light is either fixated directly in the sclera or in a trochar-cannula. In general, scleral-based fixation is used for eyes that are not vitrectomized and the trochar-cannula - based chandelier light for eyes that are vitrectomized and have a soft globe. This enables bimanual surgery and allows the surgeon to use a second active instrument in addition to the vitreous cutter. In 27G an Eckhardt twin light chandelier is available. For optimal illumination of a chandelier light, an external light source (Photon, Xenon) or a modern vitrectomy machine (Stellaris PC, Constellation, Eva) is required.
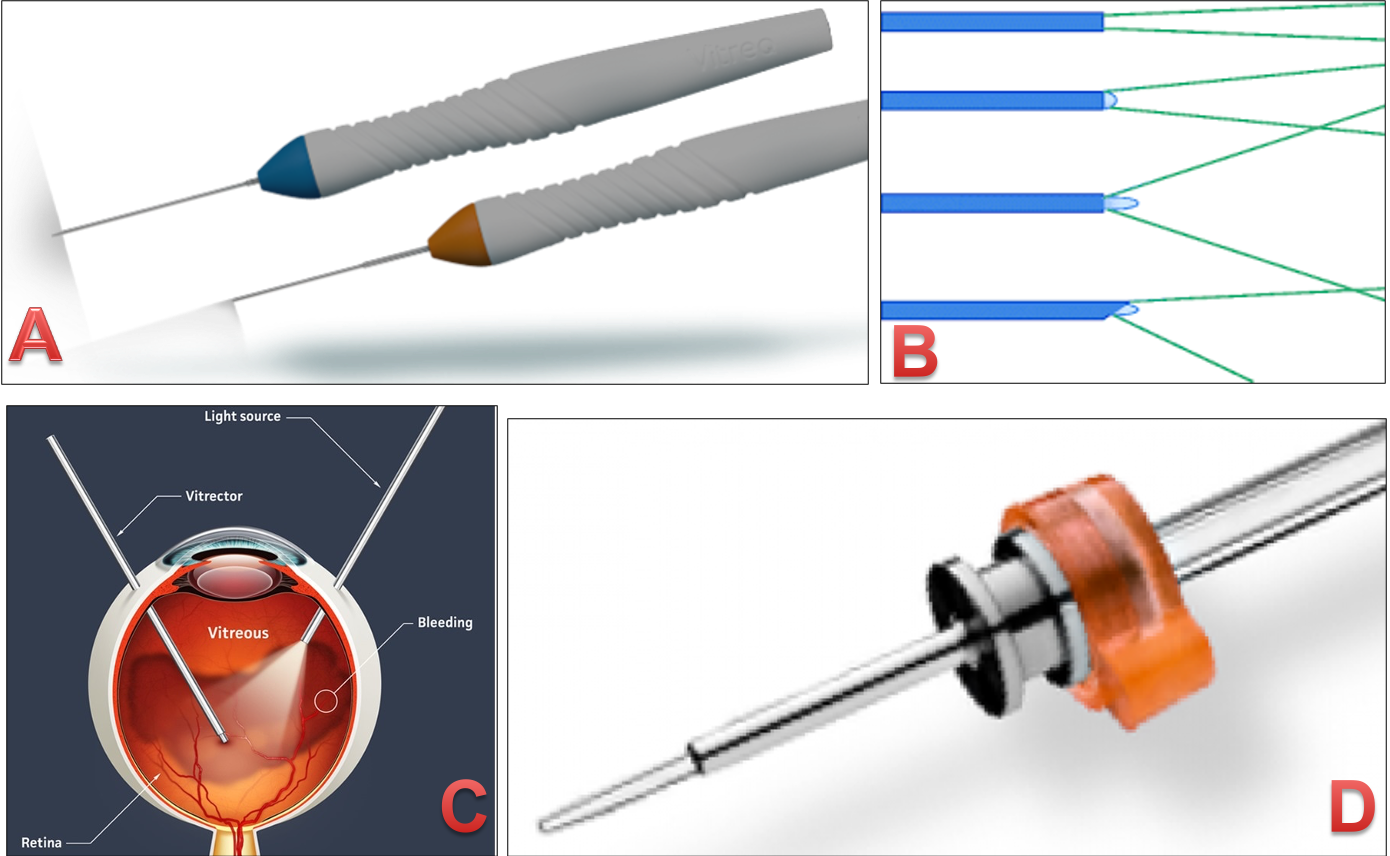
Figure 10: Light source used during vitrectomy. A. Comercial available light source B. Graphic suggestive of different design of light source and their role C. intraoperative role of light source D. Chandlier light source as an additional light source for complicated &/or bimanual surgery
Endolaser probe: The first endophotocoagulation probe was developed by Charles in 1979 and he only first reported endophotocoagulation using a fiberoptic probe attached to a portable xenon arc photocoagulator.
The most frequently used endolasers for vitreoretinal surgery today are the green and infrared diode laser. Laser tissue interaction principles even in surgical lasers are the same as photocoagulation and the effect depends upon the distance of the probe tip from the retina and angulation of the tip relative to the retina in addition to the standard parameter like laser power, duration, and pigmentation of retina. The xenon arc beam was divergent and hence the tip had to be positioned close to the retinal surface. The argon laser had a smaller angle of divergence enabling the probe tip to be positioned at a safer distance from the retina. Argon laser is also capable of rapid repetitive laser applications and could be used through air or fluid in contrary to xenon arc laser. The fiberoptic had an outer diameter of 0.89 mm (20 gauge) facilitating insertion through the same sized sclerotomy as other intraocular instruments. The diode laser is commonly used nowadays in vitreoretinal surgery. It is cheap, compact, portable and comes in infrared and green wavelengths. The clinical appearance of the burn while it is being made is similar to that with argon laser, but it is subtly lighter, especially in less pigmented eyes. Endolaser probes may be straight or curved and the recent one is having an adjustable, retractable tip. The straight probe provides direct access to the treatment site and facilitates easy access through the sclerotomy site. Angled probes (curved tip) are useful for applying endolaser anterior peripheral retina in addition to reduces the risk of lens touch in phakic eyes. Probes with adjustable tips have a fiberoptic which can be continuously adjusted over a wide range of angles for full coverage of peripheral retina and hence having the advantage of both straight and curved laser probe. Other uses of this laser with the probe are cyclophotocoagulation and correopexy.
Eckardt wound closure spatula: Proximal end of handpiece features a blunt insertor that facilitates re-insertion of 23 gauge cannulas. The tip has a V-shaped guided design with a knob-controlled pressure plate that promotes self-sealing of incision by applying exact pressure at the sclerotomy site.
Instruments used in RD surgery
Charles Backflush/Flute needle: It is basically a blunt needle with a handle containing channel and side port that is vented externally to evacuate nonclotted blood by permitting intraocular fluid to flow out of the eye through the needle and handle. Basically it works on the principle of the pressure gradient. The pressure difference between the intraocular pressure and the lower atmospheric pressure, when side port is not covered is a force for passive egress of fluid. In larger 19 – 20G surgery, this instrument can be of uniform diameter or tapered tip. The advantage of a tapered tip is limited fluid egress causes reduced outflow and hence more effective while working close to the detached mobile retina or at the posterior break. In MIVS, this needle is also available with a soft silicone rubber tip to minimize direct tissue trauma. A special handpiece has also been designed with a soft silicone catheter within the needle that can be advanced and used as an active suction.
Diathermy/Electrocautery: Its a device used frequently to control bleeding, to cause shrinkage of fibrovascular tissue, to mark the margin of retinal breaks, or to create a drainage retinotomy. It can be unipolar and bipolar, but bipolar is preferable to minimize stray current that might be conducted by the optic nerve. It can be co-axial or bimanual. Coaxial bipolar diathermy is preferred for marking retinal break and creating a drainage retinotomy, while bimanual bipolar diathermy is preferred to stop bleeding from elevated fibrovascular tissue. In case of bleeding from the inner retinal surface, diathermy of the choice is again coaxial one, which creates a small elliptical field of current around the tip, and hence bleeding site can be treated without tissue mass to hold in-between. It should be avoided on or close to ONH. Electrocautery presently used with a recent constellation machine is a high frequency (1.5MHz) sinusoidal diathermy producing 10watt maximum. Proportional control eliminates the need for an assistant to adjust the optimum power and intensity. Higher frequency produces a more focused lesion probably limiting the collateral damage.
de Juan micro-pic forceps: it is used to dissect tissue planes and separate epiretinal membranes from the inner retinal surface. There are series of instruments with different tip designs including the varying degree of angulation, contour, and sharpness to permit dissection from a different direction and to engage tissues of different consistencies. The most common variety of pic used is the one with tapered tip angulated 90 degrees.
Dual bore PFCL injector cannula: Injection of PFCL through one of the superior sclerotomy will result in a limited escape path for the BSS to come out. PFCL being a low viscosity liquid, can be injected through small microlumen easily hence dual lumen cannula came into to picture. In this cannula, the lowermost opening is for entry of PFCL into the vitreous cavity, all the middle opening are for BSS in the vitreous cavity to enter into canula to go out while uppermost opening opens into the exterior to drain out the BSS. They are really useful, especially with Valved trochar cannula.
Endocryo probe: Intraocular cryotherapy is applied with a straight cryoprobe with a 1.0 mm diameter (19G). Retina adjacent to break is touched with the end of cryoprobe and pushed against the RPE if there is substantial SRF. An iceball forms surrounding the tip and envelops the retina and underlying RPE and choroid. So here it can be useful in a case with albino fundus or wherever surgeon wants to create chorioretinal adhesion in presence of RPE atrophy. It is important to defrost the probe before moving it to avoid tearing of retina and the underlying choroid.
Retinal tacks: One of the obsolete instruments, mainly was used in pre-PFCL era. They have been developed to a temporary secure portion of the retina to choroid and sclera in GRT, the eye with extensive retinotomies. It is 0.2 mm in diameter and 2.7mm long and can be introduced with a transvitreal device. It is not optional to permanent retinopexy (Laser/Cryo).
Nob Spatula: One of the ancient instruments available in only 20G, used for massaging the edge of the retina in an attempt to unroll or flatten the edge of GRT or relaxing retinotomy.
Instruments used in Diabetic vitrectomy :
Membrane peeling forceps: They are of several types with varying sizes, shapes, and compositions. Some have both peeling and grasping, some are diamond dusted to prevent membrane slippage from the forceps. The common characteristic among all of them is, having the ability to grasp a membrane only with the tip of forceps and hence also called ‘End gripping/grabbing forceps’ or ‘epiretinal forceps’. It can be power-driven with linear(Proportional) control.
Microscissors: They are useful to cut/dissect tissue near the inner retinal surface while causing only minimal traction on adjacent vitreoretinal attachment. It can be horizontal, useful in delamination, or vertical useful in desegmentation. It can be power-driven and finger driven. Power scissors can be with a single cut and multi-cut with horizontal curved tipped or vertical. Finger driven are most commonly used.
Instruments used in macular hole surgery :
Vitreoretinal INternal limiting membrane Colour Enhancer (VINCE): Its an ILM painting brush constructed of a silicone tube connected to a 20G metal cannula, a diluted dye in a silicone cartridge. The unique characteristic of the instrument is that, like a painting brush, you can selectively brush the limited area of the ILM over the desired area and hence reduce the overall amount of the dye used and exposed to the retina and thus reduce the risk of toxicity. It also prevent the dye migration and staining of posterior capsule even in fluid filled cavity and hence remove the need of using dye under air.
ILM peeling forceps: This forceps is used to pinch the ILM and hold the elevated edge to complete the maculorrhexis.(Available in all gauge). Newer ILM peeling forceps are also available in power driven with linear proportional control.
Finnis loop: This is recently introduced retractable wired loop with serration on the inferior edge. Make of wire gives it unique characteristic like retractibility for easy entry through smaller gauge ports and malleability to prevent direct pressure-induced trauma to retina. It is used to create and elevate the ILM flap as well as to complete the maculorrhexis.
Tano’s diamond dusted scraper: Diamond dusted end gives rough surface which helps in creating the flap with avulsion mechanism. Mainly used for ILM peeling but can be used for ERM removal or sometimes for peeling of flat fibrovascular proliferation too.
Instruments used in IOFB removal surgery
Machemar FB forceps: It is mainly a bulky forceps, available mainly in 17G, 19G, and 20G. Generally, this instrument has a roughened/serrated tip to provide a good grasp over the IOFB. Newer modification has a diamond-dusted tip for good hold on IOFB.
Magnet : They are different types and needed to remove the iron foreign body. It can be applied external to the sclera or introduced into the vitreous cavity. External magnets range from small pencil-like models to the electromagnet of varying sizes. A handheld magnet is usually preferred and has interchangeable tips. Short blunt tip enhances the strength of the magnetic field: thin, elongated tips permit application in areas where exposure is difficult. Electromagnet that used intravitreally has a slender elongated tip. The reduction in the magnetic field is offset by the reduced distance between the tip and the intraocular foreign body. The electromagnet has its magnetic pole external to the eye, even when an intraocular tip is used. Therefore, a foreign body may be pulled towards the magnetic pole rather than the tip if not held and aligned properly. Permanent earth magnet is available in 20G with a magnetic pole at the center of the tip, but are relatively weaker than electromagnet, still the problem of alignment can be avoided.
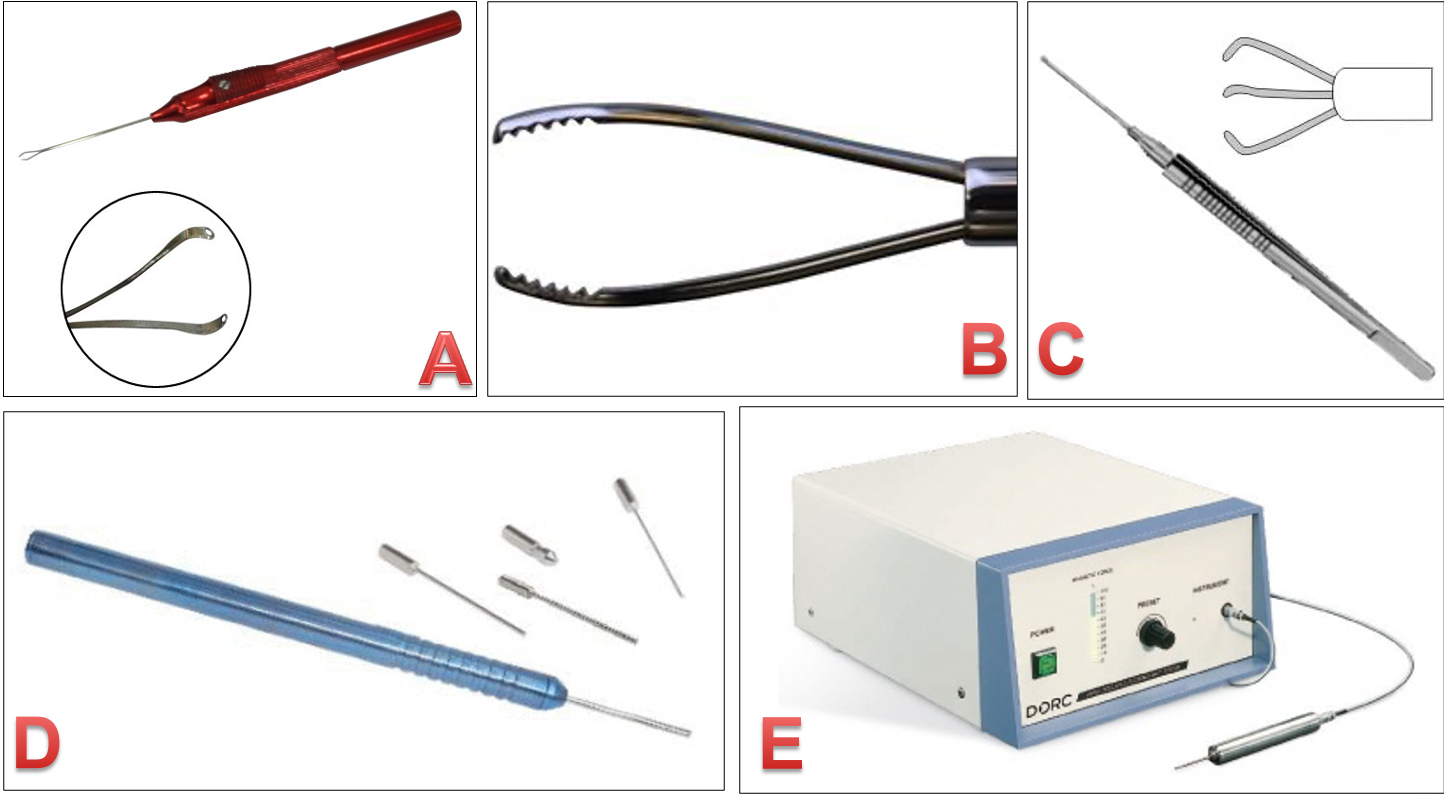
Figure 11: A. Foreign body holding forceps – biblade B. Foreign body forceps with serrated tip C. Foreign body forceps Triblade D. Foreign body magnet – Earth 5. Electromagnet
Instruments used in lens-related vitreous surgery
Ultrasonic phacofragmentor: It is a needle used to remove the cataractous lens of firm consistency. Having a separate infusion line during vitrectomy, the need for infusion line with fragmentor is eliminated which gave the breakthrough in availing this instrument in MIVS too. Proper complete removal of vitreous all around the nucleus and complete vitrectomy is a prerequisite before entering with this instrument in order to have the least possible undesirable effect. Clear Understanding of the word, ‘phaco power’ which reflects stroke length is important here. Phaco power should be generally kept not more than 5- 10 % to reduce the stroke length. More important here is positioning of the tip of fragmentotome, which should be always in the mid vitreous cavity and nevertheless close to or on to retina to avoid unplanned contact with the retina or pushing the nuclear pieces close to/on to the macular region. In case of a softer nucleus, it can be dealt with microvit itself. In absence of the fragmentome, the limbal/Scleral section can be used to deliver the nucleus in toto, if IOL is not placed in primary cataract surgery.
Instruments used in SFIOL
Axis marker: Conventional radial keratotomy marker is the most common instrument used to mark horizontal axis. There are few dedicated axis marker with simultaneous marking of the flaps are also available.
Haptic holding micro forceps(DORC): Specific non-traumatic micro forceps with relatively shorter shaft length are available to enter through the sclerotomy for easy exteriorization of haptic. It can be curved or straight.
High myopic instrument: These are the instrument having 5.0-millimeter extra shaft length to deal with these eyes with high axial length. Mainly instruments used over posterior pole like end gripping forceps, ILM peeling forceps and backflush needs are
Instruments used in Subretinal Surgery :
All the subretinal surgery required an additional set of instrumentation in addition to the standard instrumentation for the vitrectomy. The most important among this additional set is
130⁰ angled 36G subretinal pick
130⁰ angled 33G subretinal infusion cannula
130⁰ angled horizontal subretinal forceps
130⁰ angled horizontal subretinal scissors
Each of these four instruments has few common characteristics like a long tapering tip to permit the retinotomy to be made as far from fovea as possible. 130⁰ angulation from the shaft allows manipulation at the tip of the instrument without striking the heel against the RPE or choroid.
Recent advances: 41gauge Injection – Aspiration dual-bore cannula and 42Gauge injection cannula.
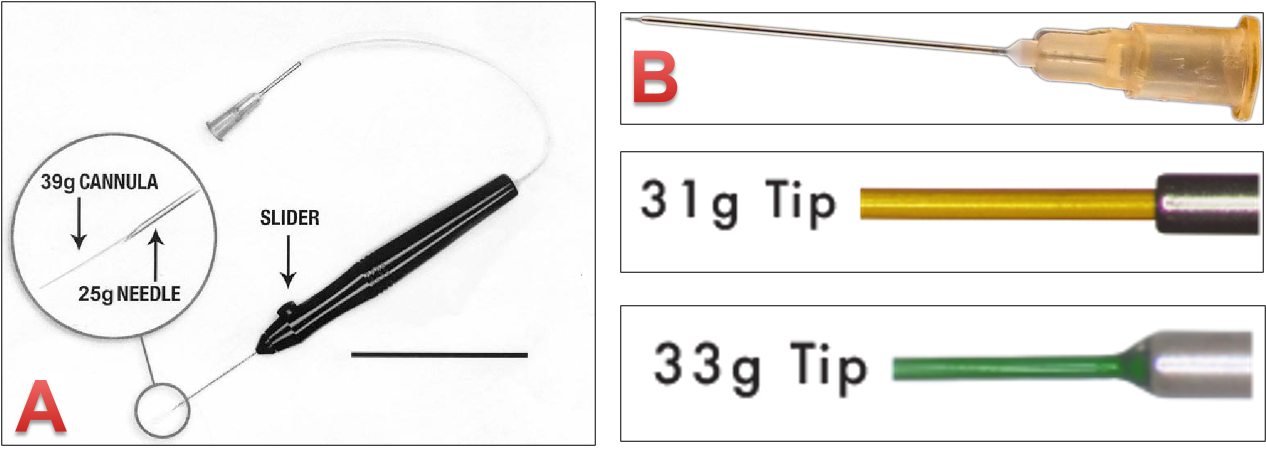
Figure 12. Subretinal surgery instruments A. 25g subretinal injection cannula with 39G extendible tip B. 25G injection cannula with 48G fixed-length tip. Tip of 31G aspiration cannula and the tip of 33G aspiration cannula
Instruments with combined function: for bimanual surgery
Irrigating chandlier: Infusion along with light source can be useful not only during bimanual surgery but also provide a better view during routine 3 port pars plana vitrectomy without extra 4th sclerotomy.
Illuminated pick: Better visualization of the semitransparent and transparent membrane will help in easy identification of a site for membrane peeling in addition to better visualization of the widespread membrane and their removal with bimanual technique.
Aspirating pic forceps: Specifically used during membrane peeling. Aspiration function will provide the uninterrupted clear field during peeling.
Illuminated endolaser probe: The illuminating laser probe described by Awh et al. provides the functions of endolaser and fiberoptic illumination in a single instrument. It frees the surgeon’s non-dominant hand which can be used for bimanual techniques or scleral depression. The laser and illumination rays differ in the angle in which they enter the optical fibers, resulting in significantly different emission angles. This permits the probe tip to be positioned sufficiently away from the retina to provide good illumination while maintaining effective laser spot size. Uram has described an ophthalmic laser microendoscope which is a triple function endoscope combining illumination, endolaser, and video endoscopy capabilities. Such probes reduce intraoperative complications related to frequent instrument insertion and extraction through the sclerotomy and can be employed where a clear view of the posterior segment cannot be obtained.
Basic facts of understanding the MIVS :
The gauge which we address is an internal diameter of trochar-cannula and not the sclerotomy size. A 27G trocar creates a 25G sclerotomy. A 25G trocar has a 23G sclerotomy. And a 23G trocar has a 22G sclerotomy.
Hagen–Poiseuille equation (Flow ≈ diameter4 ) and its relevance for vitrectomy
|
Gauge |
Internal diameter (mm) |
Flow(Diameter4) |
|
|
20G |
0.52 |
0.073 |
|
|
23G |
0.39 |
0.02 |
3.65 times less flow than 20G |
|
25G |
0.29 |
0.007 |
2.8 times less than 23G |
|
27G |
0.2 |
0.0016 |
12.5 times less than 23G |