
Introduction
Intraocular lymphoma, a great non-infective masquerader occurs intraocularly in either the vitreoretinal( primary vitreoretinal lymphoma PVRL)) or in the uveal space( primary choroidal, iris lymphoma). By definition, PVRL denotes the presence of pathology limited to vitreoretinal space without its occurrence in the central nervous system. The term ‘primary’ is however controversial as almost 56-90% of PVRL patients will ultimately go on to involve the CNS over few months to years( 8-29 months) and is considered a subset of primary CNS lymphoma( PCNSL) [1]. Incidentally, 25% of patients with PCNSL will have concurrent ocular involvement at presentation [2]. Primary choroidal and iridial lymphomas are rarer, less aggressive as compared to their vitreoretinal counterpart and due to their rarity, the following section will deal primarily with PVRL.

Pathophysiology of Primary Vitreoretinal Lymphoma
The origin of lymphoma cells in the retina is a point of debate. Two etiologies have been proposed: infectious and hematogenous. Infectious etiology proposes an agent which triggers B cell migration to CNS which subsequently undergoes clonal expansion [3]. This theory is particularly true in immunocompromised individuals who have an increased incidence of lymphoma. The role of viral agents like EBV(Epstein-Barr virus) seen commonly in immunocompromised patients and its association with CNS lymphoma has already been documented [4]. Hematogenous theory suggests spread of lymphoma cells from extraocular foci to eye via the central retinal artery [5]. Preferential entry to retina rather than choroid has been attributed to selective receptive retinal endothelial receptors [6].
Once in the retina space; cells then move anteriorly towards the vitreal space and also posteriorly where Bruch membrane acts as a natural barrier preventing it from reaching the choroid. Lymphoma cells then get accumulated in the subRPE space( retinal pigment epithelium)

Clinical Features
Although PVRL is aggressive in nature, the presentation is insidious. It generally presents between the fifth and eight decade without racial predilection with slightly more occurrence in females ( female to male ratio of 2:1) [7]. It is mostly bilateral although asymmetrical. The insidious nature of the condition can be summed up as the average time to diagnose a case of PVRL from its onset of symptoms is approximately 1 year. This contradicts to a case of CNS lymphoma where the average time to diagnosis is approximately 3 months [8]. Since PVRL is closely related to CNS lymphoma its imperative to elicit any recent CNS signs in a patient suspected to have PVRL.
CNS lymphoma most commonly affects the frontal lobe, so enquiring for recent behavioral changes , or history of recent hemiparesis or ataxia is a good way to begin examination of any suspected case of PVRL [8]
PVRL is painless clinical condition with generally no signs/ symptoms of inflammation like pain and redness. The most common symptom is blurring of vision present in 90% of cases.[9]. Patient also complain of floaters which are intermittent . Patients may have already visited few ophthalmologists with multiple courses of systemic and topical steroids. Typically patients will report decrease in floaters and blurring with steroids which again reappears. This is a important clinical clue which is because steroids are lympholytic in nature [9].
Clinical signs typically will show a quiet eye with no scleral/ ocular tenderness. Anterior chamber may be absolutely quiet or present with cells/ flare and keratic precipitates(KP). Rarely PVRL can present with pseudohypopyon. Although presence of cells and KP mimics other uveitic entity, a close examination of these KP and cells yield important clinical clues. Cells in PVRL will be larger and so will be the KP which are typically found throughout the corneal endothelial surface. With time these KP will not show changes of pigmentation or change its shape. These features are because cells are not true inflammatory cells but individual lymphoma cells which then conglomerate to form the KP. Posterior synechiae is typically absent.
Posterior examination reveals presence of vitreous haze secondary to vitreous cells. Depending on the state of vitreous syneresis, vitreous haze can be divided into 3 types [10]. Aurora Borealis variety of vitreous haze was reported to be the most common where the individual lymphoma cells align themselves along the vitreous fibrils. The other 2 types are string of pearls where lymphoma cells align akin to a string of pearls and non specific variety.
The most typical sign are multiple foci or a single foci of yellowish subRPE deposits( figure 1). An earliest retinal sign is perivascular infiltration which mimics vascular sheathing (figure 2). These deposits are individual clusters of lymphoma cells. Since Bruch’s membrane acts as a natural barrier to spread of cells towards choroid, these cells then gradually rests under the RPE. Gradually over time with varying degrees of RPE atrophy, a typical ‘leopard spot’ appearance is seen.
An important clinical sign is the absence of cystoid macular edema in spite of long standing cells.
PVRL comprised mainly of B cell has increased interleukin 10 levels( IL10) in aqueous and vitreous. IL10 in turn helps in B cell proliferation and decreases host immunity. This explains the absence of typical inflammatory signs like redness, pain, and cystoid edema [11].
Suspect PVRL when
|

Figure1: Typical appearance of sub RPE lymphoma
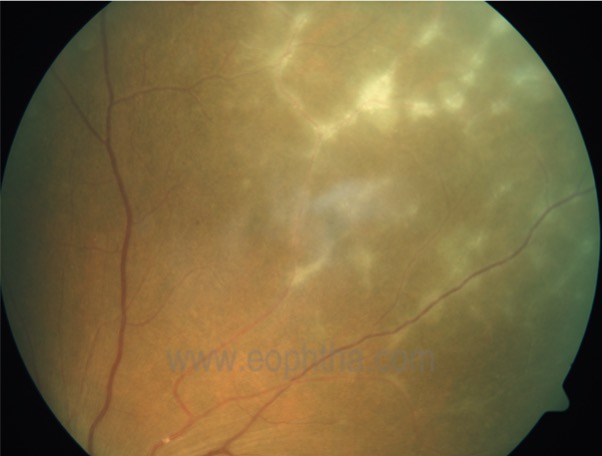
Figure 2: Early PVRL mimicking vasculitis
Differential diagnosis
Being a great masquerader, following ocular conditions need to be kept in mind when examining a case of PVRL
|
Inflammatory conditions:
Infectious entities
Neoplastic conditions
|
Imaging in PVRL
Although a typical clinical appearance of yellowish subretinal / subRPE deposits is very much suggestive of PVRL, early retinal lesions are very much confusing even to the best of the clinician.
Fundus Autofluorescence ( FAF): Since the lymphoma cells rest in the subRPE space, FAF plays an important role. Typically on FAF, early lesions appear hyper-autofluorescent, and as the overlying RPE undergoes atrophy FAF lesions become to hypo autofluorescent. FAF findings are not pathognomic although it's useful for the follow-up to detect new lesions and should be corroborated with other imaging modalities [12].
Optical Coherence tomography( OCT): No other retinal imaging modality provides so many novel markers for early detection of PVRL as does OCT. Since the pathology in PVRL is mainly concentrated in the subRPE space, OCT scans specifically documenting the same is useful. Lesions may not be in the macula; hence it's important to convey to the OCT technician the area in the retina to scan through. Multiple nodular saw tooth-like elevations of RPE with hyper-reflective areas beneath RPE is typical which denotes infiltration of lymphoma cells. As the disease progresses, there occurs disruption of the interdigitation and ellipsoid zone with multiple hyperreflective and confluent bands in the subretinal space [13]. The presence of these hyperreflective bands along with nodular RPE elevations have reported to be typical of PVRL [13](figure 3). Vertical hyper-reflective lesions( VHRL) is a recent OCT biomarker described in PVRL [14]. These are hyperreflective columnar lesions extending from inner retina( ganglion cell/ nerve fibre layer) to RPE. Pathophysiology of VHRL is not known although they have been postulated to be early lymphocytic infiltrations of sensory retina
Fundus Fluorescein angiography( FFA): FFA features of PVRL are not diagnostic. Window defects, staining and blocked fluorescence are some of the features seen in PVRL. Features of leakage are typically not observed. Capillary dropout a feature seen in FFA has been described by Ramesh et al secondary to tumor infiltration of sensory retina leading to ischemia [15]. Although an interesting find it may not be pathognomic.
Ultrasound(USG): B scan usg yields no additional result in cases of PVR although it may be an useful adjunct in cases of optic nerve infiltration .
Neuroimaging: 16-34% of PVRL patients will have concurrent CNS disease. When suspecting any case of PVRL, its important to order a MRI of the brain with orbit with contrast. Lesions are typically hypodense on T1 and hyperdense on T2 weighted scales. Since absence of CNS lesions does not rule out the pathology in CNS, an MRI should be ordered every 3 months for the first 2 years followed by at every 6 months thereafter [9].
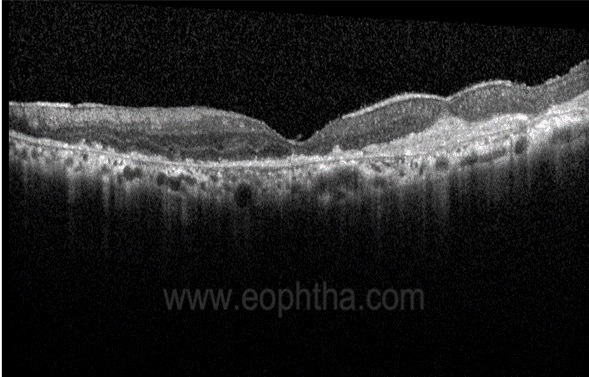
Figure 3: Typical OCT in PVRL showing sub-RPE hyperreflectivity and nodular RPE elevations
Diagnostic tests in PVRL
Like any other cancer in the body a definitive diagnosis is important to start treatment; and herein lies the most difficult aspect when dealing with patients of PVRL. Vitreous being the most accessible and common site for PVRL, vitreous biopsy is the most preferred method to diagnose or refute a case.
Method of biopsy: Before performing biopsy, its absolutely necessary to stop any form of steroids be it oral or topical. Although no fixed schedule is prescribed, a general consensus is to withdraw steroids for a minimal of 3 weeks. Biopsy can be performed either with 23 or 25 gauge vitrectomy system. Whatever the gauge, while performing the same a low cut-rate( approximately 600 cpm) is essential to prevent mutilation of lymphoma cells. Initially undiluted sample is taken. To maximize undiluted vitreous yield once the globe starts collapsing, air can be introduced through the infusion cannula and vitrectomy can proceed under air. Once sufficient material is obtained, fluid can then be turned on. Its important to send both undiluted and diluted fluid for further test, including the fluid in the cassette. Sample should ideally be processed with an hour( preferably < 30 min) to get the best possible outcome. In case no inhouse pathologist is available, sample can then be send via RPMI( Rosewell Park Memorial institute) solution or HOPE solution( Hepes Glutamic acid buffer mediated organic solvent effect) in a ratio of 2:1. If none exists, commercially available Ctyolyt solution can be used [16,17]. Its best not to to transfer sample in alcohol solution. Its important to remember that lymphoma cells are fragile and gets destroyed easily, hence prior intimation to pathologist is crucial. If vitreous yield is less a retinal biopsy with aspiration of subretinal material is warranted.
Sample obtained ideally needs to undergo five assessments. They are a) cytological b) immunohistochemical analysis c) Flow cytometry d) Molecular analysis e) assessing cytokine levels.
Cytological exam is the most commonly performed test whereby a morphological assessment of the vitreous sample is performed. Typically pathological lymphoma cells appear large with a scanty cytoplasm and prominent nucleus and nucleoli. If seen diagnosis of PVRL is certain , but alone confirms < 50% cases [11]. Poor tissue handling, improper trained personnel, lack of sample are some of the causes for a negative result.
Cytokine analysis is another test commonly performed. That lymphoma cells generate more of IL10 than IL6 forms the basis of this test. IL6 levels are seen more in uveitic pathologies and comparing the two helps not only to differentiate between the two but also support a diagnosis of PVRL. A ratio of IL10: IL6 >1 supports a diagnosis of PVRL although IL10 levels have also been higher in uveitic entities [18]. That IL10 levels are variable also puts this test in the spotlight. Immunohistochemical analysis and flow cytometry are useful tools to study cell surface markers mainly CD20 positivity. CD20 positivity not only confirms presence of B type lymphoma cells but also is useful in therapeutic intervention as we will see later.
Molecular analysis by PCR to confirm clonal expansion of B cells are newer tests being employed to confirm diagnosis of PVRL.
A recent marker known as myeloid differentiation primary response 88 protein( MYD88) and its mutation detected by PCR analysis is emerging to be an important diagnostic tool to confirm cases of PVRL [19]. Detecting MYD88 mutation is specially important when routine cytological and immunohistochemical tests yield negative results.
|
Checklist before Vitreous Biopsy
|
Treatment
Unlike other ocular tumors, treatment in the case of PVRL needs a thorough systemic evaluation to rule out CNS involvement. To begin with laterality of the condition along with whether CNS is involved or not is of paramount necessity. Broadly treatment can be divided into local and systemic therapy.
Local therapy includes intravitreal agents and ocular radiation. Systemic therapy involves the use of chemotherapeutic agents, whole-brain radiotherapy( WBRT), and stem cell therapy. Treatment strategies are not universal and the following description provides an approximate guide.
Uniocular disease without CNS involvement:
The choice is local intravitreal agents. The most common drugs are Methotrexate( MTX) and Rituximab although Melphalan use has also been reported [20]. Intravitreal agents are given under aseptic and sterile environment preferably in a OR setting like any other retinal intravitreal injections. The role of anterior chamber paracentesis prior to injection is not a must.
IVM( Intravitreal MTX): MTX is generally used as 400mg/0.1m dose. The ideal regimen involves: INDUCTION phase comprising of biweekly injection for 1 month, CONSOLIDATION phase of weekly injection of 2 months and MAINTAINANCE phase of monthly injection for 9 months. Due to its large number of injections, many patients opt out. Most common side effects of IVM is corneal epithelial toxicity which is reversible once injections are withdrawn.
A mean of 6.4 injections are needed to induce remission [21]
IVR: Intravitreal Rituximab. As discussed prior CD20 positivity plays an important role in therapeutics. Luckily and thankfully 95% of PVRL are large B cell with CD20 positivity. Rituximab a monoclonal antibody against CD20 has been in use and slowly gaining popularity due to its less toxic effects and less number of injections. Mechanism of action is disputed although its is believed to act by inducing apoptosis and complement mediated cell death [22]. Regimen involves weekly injections for 4 weeks. Most common side effect is increase in intraocular pressure. With either of agent, recurrences have been reported and once the same happens, its then time to switch treatment regimen.
Ocular radiation Once the most common modality of treatment, ocular radiation is now reserved in uniocular condition when intravitreal agents fail or PVRL recurs after completion of intravitreal regimen. Current regimen uses 30-36 Gy [23]. Complication of radiation includes cataract, radiation retinopathy and neuropathy. These complications have been seen even with dose as low as 20Gy.
Local ocular treatment does not alter survival time neither does it prevent CNS or other eye diseases.
If during the course of treatment, CNS disease occurs or the other eye gets affected, immediate systemic treatment in consultation with a systemic oncologist is warranted. Systemic therapy with chemotherapy in uniocular disease without CNS involvement is now being thought of as its just time before a CNS disease is detected.
Bilateral ocular disease without CNS involvement
With bilateral disease, its just time before the CNS gets involved, hence need for systemic therapy. Systemic chemotherapeutic agents include MTX, Rituximab, Ibrutinib, or Pomalidomide. Lenalidomide a newer drug with immunostimulant property holds promising results for systemic therapy [24]. Local therapy with intravitreal agents is also used along with systemic therapy in bilateral disease.
Ocular disease with concurrent CNS involvement
With primary CNS involvement, multiple therapeutic strategies get involved. Systemic chemotherapy, WBRT is initially used. Stem cell therapy is currently employed when the initial treatment fails with or without the use of high dose MTX.
Role of therapeutic vitrectomy
Apart from a few incidental case reports [25], complete vitrectomy as a therapeutic modality has never been looked into. The author here and many other retinal surgeons will however concur regression of ocular disease when a complete vitrectomy is performed. It is postulated a complete vitrectomy not only reduces ocular load but also helps better penetration of systemic chemotherapeutic agents. It is preferable to do a complete vitrectomy when doing a vitreous biopsy although vitrectomy alone should never be used as a sole treatment method.
Emerging new treatment modalities
Stem cell therapy ( SCT)has been particularly useful in refractory and recurrent systemic CNS lymphoma. SCT has been shown not only to induce remission in refractory cases but also increases the overall survival rate [26,27].
Role of Ibrutinib: Ibrutinib a chemotherapeutic agent originally used for chronic myeloid leukemia, has shown promising results in systemic lymphoma. It's particularly invaluable as ibrutinib has been shown to cross both the blood-retinal and blood-brain barrier and is available as an oral agent [28,29]. Its role in PVRL will need further research.
PVRL is a unique ocular condition where the role of an ophthalmologist in its diagnosis cannot be over-emphasized. That an ophthalmologist can diagnose it before the CNS gets involved speaks volumes about our fraternity. Keeping it as a differential whenever examining any elderly patient with recurrent uveitis will surely help in detecting it early. Most importantly taking a second opinion from our colleagues whenever in doubt, rather than empirically starting steroids will also help to catch it early. Hopefully, this article will help our ophthalmologists friends to lift the veil off this great masquerader.
References
- Chan CC, Rubenstein JL, Coupland SE, et al. Primary vitreoretinal lymphoma: a report from an International Primary Central Nervous System Lymphoma Collaborative Group symposium. Oncologist 2011;16:1589–1599.
- Hochberg FH, Miller DC. Primary central nervous system lymphoma. J Neurosurg 1988;68:835–853.
- Chan CC. Molecular pathology of primary intraocular lymphoma. Trans Am Ophthalmol Soc. 2003;101:275e92
- Damato BE, Bever GJ, Afshar AR, Rubesnstein JL. Insights from a case of Vitreoretinal lymphoma. Ocul Oncol Pathol. 2019 Jan;5(1):13-19
- Zamora DO, Rivere M, Choi D, Pan Y, Planck SR, Rosenbaum JR et al. Proteomic profiling of human retinal and choroidal endothelial cells reveals molecular heterogeneity related to tissue of origin. Mol Vis 2007; 13: 2058–2065.
- SagooMS, Mehta H, Swampillai AJ, Cohen VM, Amin SZ et al.Primary intraocular Lymphoma. Surv Ophthalmol. 2014 Sep-Oct;59(5):503-16
- Grimm SA, McCannel CA, Omuro AM, Ferreri AJ, Blay JY, Neuwelt EA,et al. Primary CNS lymphoma with intraocular involvement: International PCNSL Collaborative Group Report. Neurology. 2008;71:1355–60
- Pulido JS, Johnston PB, Nowakowski GS, Castellino A et al. Thediagnosisandtreatmentofprimaryvitreoretinallymphoma:areview. Int J Retina Vitreous. 2018 May 7;4:18.
- Marchese A, Miserocchi E, Giuffrè C, Cicinelli MV, Querques G et al. Aurora Borealis and string of pearls in vitreoretinal lymphoma: pattern of vitreous haze. Br J Ophthalmol.2019 Feb [Epub ahead of print]
- JL Davis. Intraocular Lymphoma: a clinical perspective. Eye 2013 27: 153-62
- Casady M, Faia L, Nazemzadeh M, Nussenblatt R, Chan CC, Sen HN. Fundusautofluorescencepatterns inprimary intraocular lymphoma. Retina. 2014 Feb;34(2):366-72.
- BarryRJ,TasiopoulouA,MurrayPI,etal. Characteristic optical coherence tomography findings in patients with primary vitreoretinal lymphoma: a novel aid to early diagnosis. Br J Ophthalmol. 2018;102(10):1362-1366
- Deak GG, Goldstein DA, Zhou M,Fawzi AA,Jampol LM.VerticalHyperreflectiveLesionsonOpticalCoherenceTomographyinVitreoretinalLymphoma. JAMA Ophthalmol. 2018 Nov 29
- Venkatesh R,Gurav P,Abhishek Dave P,Gandhi A. CapillaryDropout:ANovelFluoresceinAngiographyFindinginPrimaryVitreoretinalLymphoma. Ocul Oncol Pathol.2017 Nov;3(4):324-327
- Coupland SE. Analysis of intraocular biopsies. Dev Ophthalmol. 2011;49: 96?116
- Coupland SE, Perez-Canto A, Hummel M, et al. Assessment of HOPE fixation in vitrectomy specimens in patients with chronic bilateral uveitis (masquerade syndrome). Graefes Arch Clin Exp Ophthalmol. 2005;243: 847?852.
- Sugita S, Takase H, Sugamoto Y, Arai A, Miura O, Mochizuki M. Diagnosis of intraocular lymphoma by polymerase chain reaction analysis and cytokine profiling of the vitreous fluid. Jpn J Ophthalmol 2009; 53: 209–214
- Raja H, Saloma?o DR, Viswanatha DS, Pulido JS. Preva- lence of MYD88 L265P mutation in histologically proven, diffuse large B-cell vitreoretinal lymphoma. Retina 2016; 36:624–628.
- Shields CL, Sioufi K, Mashayekhi A, Shields JA. IntravitrealMelphalanforTreatmentofPrimaryVitreoretinalLymphoma: ANewIndicationfor anOldDrug. JAMA Ophthalmol.2017 Jul 1;135(7):815-818
- Frenkel S, Hendler K, Siegal T, Shalom E, Pe’er J. Intravitreal methotrexate for treating vitreoretinal lymphoma: 10 years of experience.Br J Ophthalmol2008;92: 383–388
- Hashida N, Ohguro N, Nishida K. EfficacyandComplicationsofIntravitrealRituximabInjectionforTreatingPrimaryVitreoretinal Lymphoma. Transl Vis Sci Technol.2012 Oct 22;1(3): 1. eCollection 2012
- Kaushik M, Pulido JS, Schild SE, Stafford S. Risk of radiation retinopathy in patients with orbital and ocular lymphoma. Int J Radiat Oncol Biol Phys. 2012;84:1145–50
- Rubenstein JL, Treseler PA, Stewart PJ: Re- gression of intraocular large B-cell lymphoma with lenalidomide monotherapy. J Clin Oncol 2011;29:e595–e597.
- Venkatesh P, Gogia V, Khanduja S, Gupta S, Kumar L. Therapeuticvitrectomyforvitrealrecurrenceofintraocularlymphomaresistanttointravit real methotrexatepostsystemicchemotherapy. J Cancer Res Ther.2015 Jul-Sep;11(3):668
- Soussain C, Hoang-Xuan K, Taillandier L, Fourme E, Choquet S, Witz F, et al. Intensive chemotherapy followed by hematopoietic stem-cell rescue for refractory and recurrent primary CNS and intraocular lymphoma: Societe Francaise de Greffe de Moelle Osseuse-Therapie Cellulaire. J Clin Oncol. 2008;26:2512–8.
- Soussain C, Choquet S, Fourme E, Delgadillo D, Bouabdallah K, Ghesquieres H, et al. Intensive chemotherapy with thiotepa, busulfan and cyclophosphamide and hematopoietic stem cell rescue in relapsed or refractory primary central nervous system lymphoma and intraocular lymphoma: a retrospective study of 79 cases. Haematologica. 2012;97:1751–6
- Wilson WH, Young RM, Schmitz R, Yang Y, Pittaluga S, Wright G, et al. Targeting B cell receptor signaling with ibrutinib in diffuse large B cell lymphoma. Nat Med. 2015;21:922–6.
- Bernard S, Goldwirt L, Amorim S, Brice P, Briere J, de Kerviler E, et al. Activity of ibrutinib in mantle cell lymphoma patients with central nervous system relapse. Blood. 2015;126:1695–8.