
Question
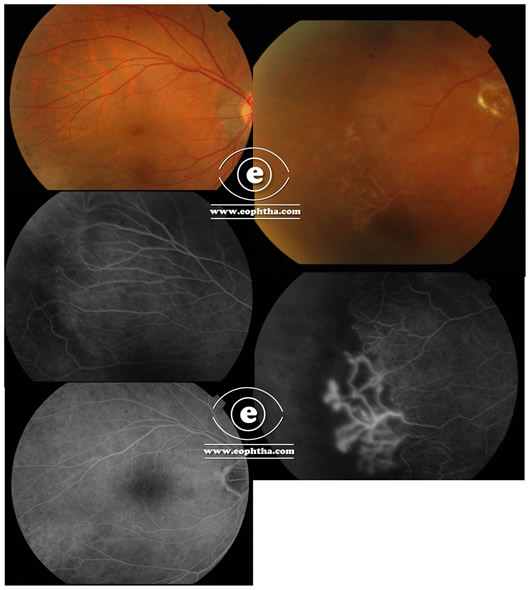
A healthy 26-year-male presented with sudden onset diminution of vision in OS of 1-week duration. The loss of vision was not associated with any trauma, pain, redness. No history of flashes. No previous history of a similar episode. On examination BCVA OD: 6/9 N6; OS: HM. Anterior segment unremarkable OU. Fundus: OD: as depicted in the fundus and FFA, OS: had a dense vitreous hemorrhage
- What are the differentials for the case based on the fundus picture/ Fundus Fluorescein Angiogram?
- How do you manage it?
Answer:
Let’s go in a stepwise fashion to decipher this question. The relevant points from history and FFA are
- The patient is young with no previous such episodes
- The loss of visual acuity is 1 week
- Although not mentioned, we presume the patient to be non-diabetic, and is not hypertensive; however, the same needs to be investigated
- The better eye has a large frond of NVE( neovascularization elsewhere) in the temporal quadrant
So differentials in a young with dense vitreous hemorrhage in one eye and a large frond of NVE in another are
Vasculitis related hemorrhage:
Vasculitis is a broad terminology used in ophthalmology under which are multiple disease conditions. In India, the foremost differential of vasculitis in a young male with the bilateral disease is Eales’s disease. The pathology involves retinal venous obliteration secondary to inflammation followed by retinal hypoxia and neovascularization which presents with recurrent hemorrhage. The pathology involves hypersensitivity to probable tubercular protein.
Another etiology seen commonly in young is SLE-related retinal arteriolar obstruction and neovascularization. Behcet disease is another important cause of retinal neovascularization and recurrent vitreous hemorrhage. It’s always preferable to look for clues in the better eye with better fundus visualization. Following are few important tips to note when ruling out causes of vasculitis
Note the presence or absence of KP, cells in the anterior chamber in both eyes. Remember vasculitis can also be infective in nature. Toxoplasmosis, Tuberculosis are few causes of infective vasculitis
In the better eye look for signs of vasculitis. The signs include perivascular sheathing with or without hemorrhage. In some cases, the vessels may be sclerosed with no ACTIVE signs which are suggestive of previous episodes of the disease entity
The presence of vitreous cells with signs of vasculitis( especially if bilateral) denotes active infection with secondary vasculitis. In young it’s imperative to rule out HIV and syphilis
Note if the vasculitis is predominantly PERIVENULAR or PERIARTERIOLAR. Causes for perivenular vasculitis include Eales disease, Behçet’s disease, Pars planitis, sarcoidosis. HIV related or also due to Multiple sclerosis. PERIARTERIOLAR causes include SLE, PAN, Varicella-Zoster infection
The second important differential in such a case is the sequelae of aborted ROP and FEVR. Both these diagnoses are often overlooked although is an important differential in young with the bilateral vascular anomaly. In aborted ROP the child will have persistent peripheral avascular retina which secondarily leads to neovascularization and vitreous hemorrhage. So in history always ask of a history of prematurity. Patients of FEVR on another hand will not have any typical history of prematurity although they will have a positive family history. Patients of FEVR generally present young with recurrent vitreous hemorrhage and is bilateral. The better eye will have multiple fronds of NVE or NVD
Blood Dyscrasias are another important differential in such a presentation especially Sickle Cell disease. Hence always ask for easy bruising, history of typical sickle cell crisis, gum bleeds, etc. Certain belts in India have predominant sickle cell disease like those in the tribal belts of Maharashtra( Vidharbha), Tamil Nadu. A simple blood test will easily rule out the same
Diabetes Mellitus: Even though this patient is young, those with type 1 disease often have their disease process begin early. The most important risk factor for developing retinal neovascularization in diabetes is the duration( apart from control and other factors). Those with type 1 disease generally begin their disease early and that is an important risk factor.
Management
Management includes not only treating the patient but also decipher the cause for the disease entity.
Ocular Investigations
Fundus Photography is an important investigation that not helps in documenting the disease but also serves as a nice educative tool for the patient and their attenders. Although a wide field photograph is ideal, it may be accessible to all. In such scenarios have a routine 7 field photograph
Fundus Fluorescein Angiogram: In all cases of unilateral vitreous hemorrhage with the other eye having suspicious areas should undergo an FFA. This case wonderfully depicts the usefulness of the same where it shows a large frond of NVE. FFA will also show areas of capillary non-perfusion which may serve as a guide for treatment by laser
Ultrasonography: Its importance cannot be overemphasized. In this case with left eye dense hemorrhage, USG will help not only to document the status of the retina but also provide clues to the status of posterior hyaloid which helps the operating surgeon plan his surgery. In the presenting case if the USG shows retinal detachment, then surgery needs to be planned at the earliest.
NonOcular investigations
Routine TC, DC, ESR, Platelet count, peripheral smear, ESR
Mantoux and Quantiferon TB gold test
HIV, VDRL, and RPR
FBS, PPBS, Blood pressure measurement
ANA, Serum homocysteine
IgG, IgM Toxoplasmosis if suspecting the same
X-Ray Chest PA or preferably an HRCT chest( rules out not only TB but also Sarcoidosis)
Treatment
Right eye
In this case, the right eye needs laser photocoagulation to treat the active frond of NVE. The laser needs to be applied not only in the vicinity of NVE but also in the Capillary non-perfusion areas as shown by FFA.
Tips for laser: Never apply laser directly to NVE or close to it. There should be a minimal of 2 disc diameter of the safe zone near the NVE. Direct laser and the close laser will increase chances of bleed and increase in retinal traction
Apply laser also to the area of capillary non-perfusion
If FFA has not been done, then let the area of sclerosed vessels serve as a guide. Generally, the area in the vicinity of sclerosed vessels is ischemic. Apply laser to the same or sectoral laser to the sector desired
If there is NVD; it denotes global ischemia needing laser to the entire retina
If the diagnosis is inflammatory in nature, then plan laser under cover of steroids to minimize secondary inflammation
In follow up pay close attention to the macula, excessive laser or the disease process itself can later on lead to macular edema
Left Eye
Let USG be a guide for treating the left eye
If USG shows an attached retina: no active intervention is needed as the duration of hemorrhage is only 1 week. Ask the patient to avoid any kind of Valsalva-related activities and to sleep with a head elevated position. Follow up every week. As and when the hemorrhage reduces apply the laser to the available retina. Keep repeating the laser as and when the view clears
THERE IS NO ROLE OF ANTIVGEF only if surgery is not planned. INJECTING ANTI VEGF only in such cases with no prior treatment history is NOT ETHICAL.
Most of these cases show a wonderful resolution of hemorrhage with a conservative approach
If USG shows retinal detachment or shows traction involving the macula, then surgery needs to be planned which will be done by the retinal surgeon. Surgery involves removing the vitreous, removing any form of traction, and applying a laser.
Surgery can also be planned if the hemorrhage shows no signs of clearing even after 3 weeks. The earlier teaching of waiting for 3 months for intervention for non-clearing vitreous hemorrhage doesn’t stand in the era of small gauge vitrectomy. However a minimum of 3-4 weeks should be given before embarking on surgery