
1 How to choose the right cases to start
Idiopathic macular hole in non-myopic eye is a good case. ILM comes off as a single sheet and underlying retina is healthy. Same applies to traumatic macular holes. Beginners can also start peeling ILM in eyes with epiretinal membrane. Unsuccessful peeling may not jeopardize the long-term outcome significantly here. Peeling ILM for Myopic macular holes or in eyes with Diabetic Retinopathy needs more experience but can be achieved easily if one understands the basics of peeling.
2 Arrange your Inventory – Forceps is the key
Lander's ring with Macular contact lens, Disposable ILM forceps and BBG dye serve as a formidable low-cost inventory for ILM peeling. A good ILM forceps should match your technique of ILM peeling. Because most of us initiate peel by "Pinch Technique", forcep is desired to have a structure that can "pinch". It needs to have fine teeth on opposing surfaces and good range of movement for its prongs. It should also be light weight and easy to rotate to allow you to initiate peel in any direction and at any clock hour.
3 Illumination and Viewing system
Illumination and viewing systems play extremely important role in peeling ILM successfully and safely. Illumination can be adjusted by altering the distance of light pipe from retina. Aim is to use minimum illumination that allows adequate visualization. It's advisable not to direct light towards fovea or stay closer to fovea for prolonged duration, especially after staining. Choice of Viewing system for ILM peeling depends on Surgeon's preferences, media clarity and axial length of eyes. Non-contact Green lens from Re-Sight system is very handy for macular peeling in emmetropic eyes if media clarity is good, it's quick and assistant independent. Sutured or self-stabilizing Contact lenses provide an excellent view of macula with better depth perception. They have other advantages too - like obviating the need for an image inverter (lesser optics means better view), no obstruction to ILM forceps (advantage for long eyes) and also are not affected by fogging. Because they are in close proximity to cornea, they offer a stable field of view with little adjustments in microscope.
4 Working with Dyes
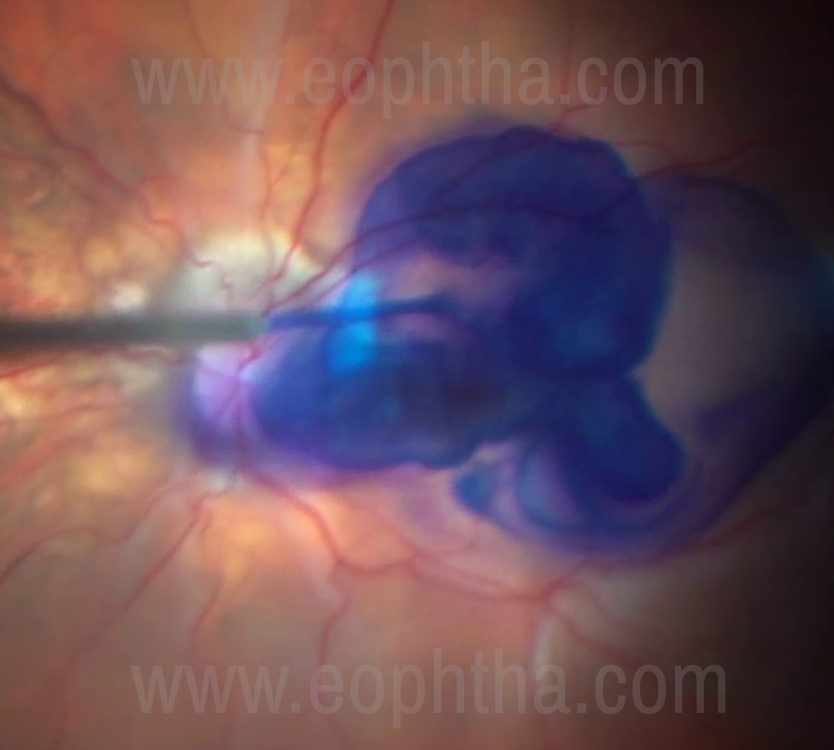
Figure-1 Intraoperative picture showing a striking contrast of BBG dye against orange fundus in a myopic eye.
Our search for a good dye for ILM ended in 2011, when we found Brilliant Blue G. 05% BBG selectively stains ILM providing nice blue contrast against orange background of fundus (Figure-1), doesn’t stain ERMs (property that was exploited for negative staining) and has not been associated with any clinically significant toxicity to photoreceptors or RPE cells. It also doesn't stain posterior capsule significantly and gives an equally great contrast in phakic and pseudophakic eyes. Unlike ICG, it is low cost and not photosensitizing in low concentrations and with shorter exposure duration, so can be used multiple times for re-staining if required. It works very well under PFO and air.
5 Choosing your initial site and creating the edge
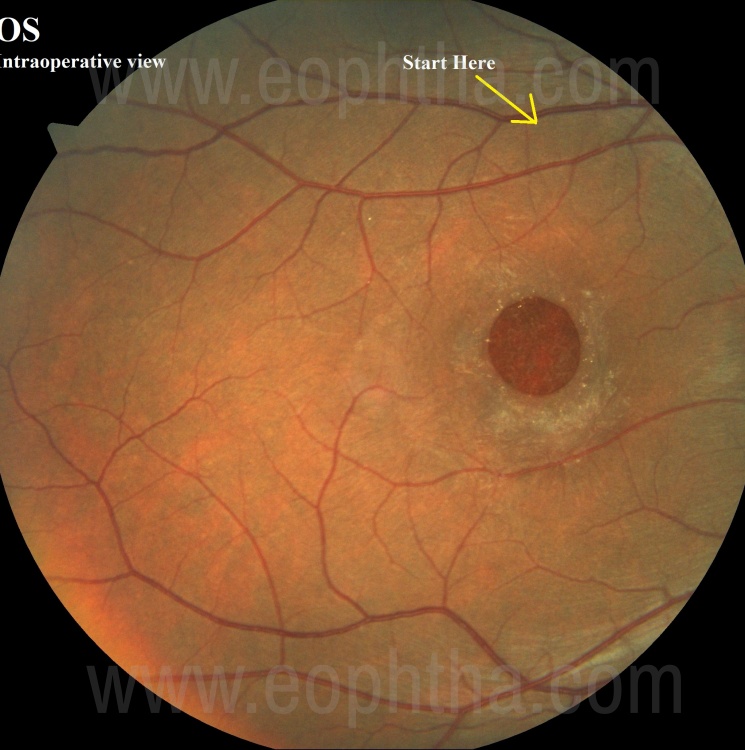
Figure-2 Inverted fundus picture of Left eye showing the inferior site (Yellow arrow) where ILM peeling can be initiated.
Peeling ILM can be a mini-project. Plan it well preoperatively to get best results (Figure-2). Your goals of peeling will vary depending upon the indication, while for macular holes you are looking to relieve tangential traction and place an ILM flap to cover it, sub-ILM hemorrhage just needs deroofing, peeling in retinal detachment can address a star fold in vicinity and so on. Planning your peeling should also include the site where you will initiate (Figure-2). Most would recommend starting at inferior macula close to a retinal vein, acknowledging that the trauma to NFL from “PINCH” would produce a superior scotoma for patient and also the ILM is easier to pinch and peel near blood vessel (Figure-3). Surgeon should also consider the comfortable hand position while choosing the starting point.
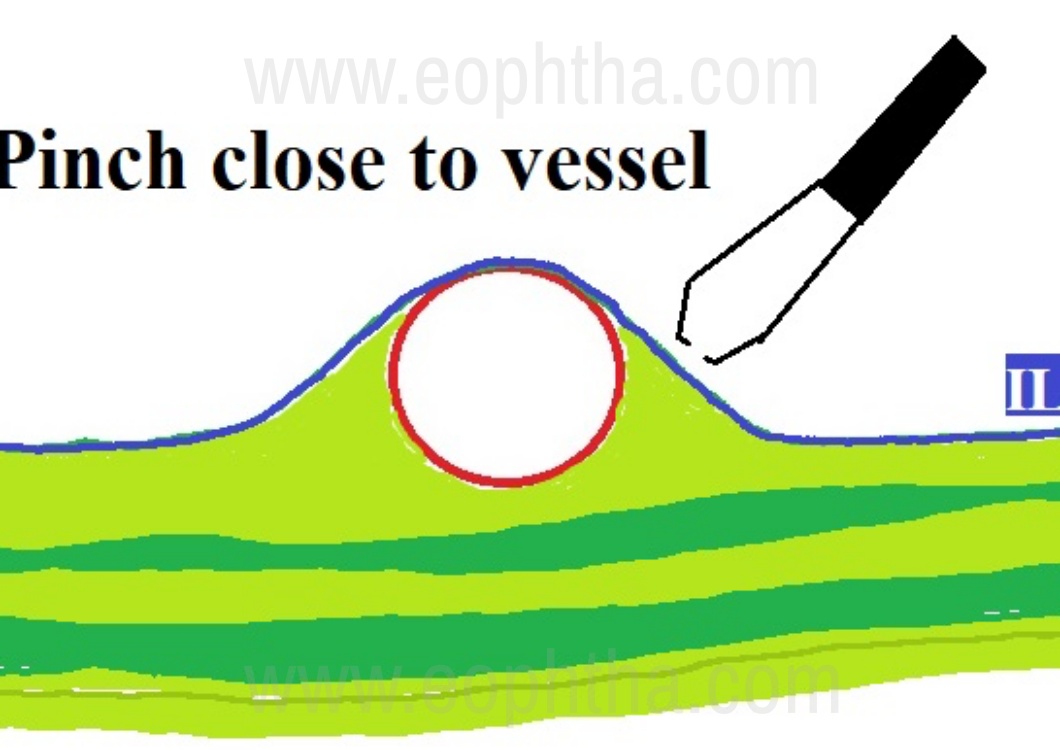
Figure-3 Schematic Diagram showing why “pinching ILM” is easier close to blood vessel.
Successful peeling needs creation of an “edge”. Earlier days, 20G MVR blade was used to create the edge. The process was traumatic and demanded improvisation. This was followed by maneuvers like fluidic separation, diamond dusted membrane scrappers, bent needles to lift the edge of ILM. Introduction of 25G and 27G vitrectomy ensured that surgeons would do maximum from cutter and forceps. Most surgeons use ILM forceps to create the edge with “PINCH” technique. This technique requires you to touch ILM with open blades of ILM forceps, followed by a gentle indentation and pinch ILM to lift it and then “release” it. This pinch and release technique loosens the ILM. Surgeon can now pinch again to pick ILM and peel off a thin strip to get a long edge (Figure-5). The long edge facilitates creation of a larger flap.
6 Peeling techniques including Flaps
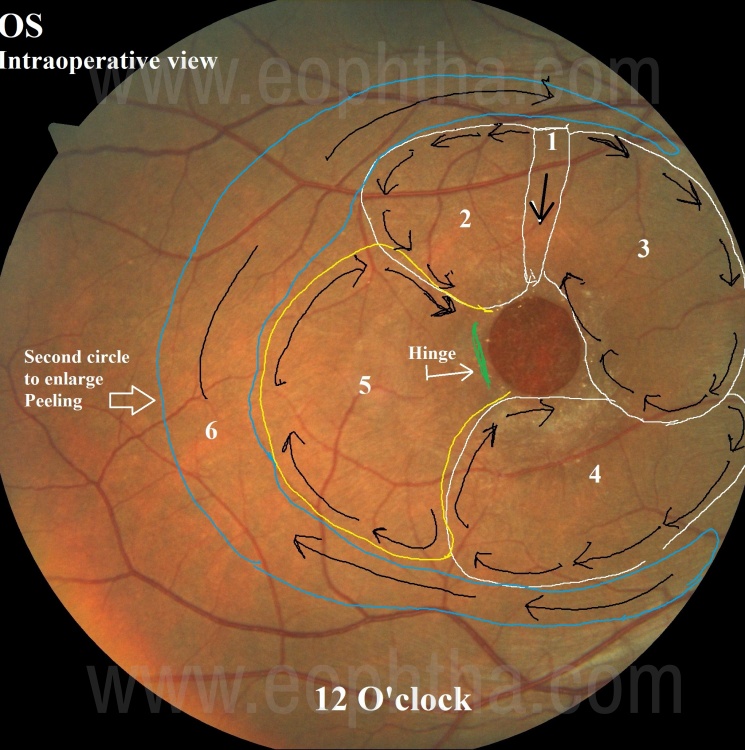
Figure-4 Overlay on inverted Fundus picture of Left eye showing a sample of ILM peeling plan. Numbers indicate the sequence in which ILM can be peeled in 6 circles. Every circle is started at the most peripheral part of the edge. 6th circle is peeled in way to create a temporal flap (Yellow circle) with the hinge (green line) at the temporal edge of the macular hole. 7th strip (blue line) is peeled in the last to enlarge the size of peel.
Once the “Edge” has been created, the peeling can be progressed by holding the edge of ILM at the point that is farthest from Fovea and ILM is peeled circumferentially in a circular pattern. It’s always good to plan your peeling technique before-hand to guide you in controlling these circles to achieve your goals. Because repeated pinching to lift ILM is believed to be traumatic, one should try to get bigger flaps. While you are planning for a large flap, the process itself should be done in small steps (note more than 2 DD in each step). This will not only help you control the size and direction of peeling but also prevent inadvertent hitting of retina especially in myopic eyes with staphyloma. Figure – 4 shows one sample plan for creating a temporal ILM flap with hinge at the temporal edge of macular hole. While surgeons need to improvise and upgrade skills regularly, it always helps to have a fixed plan (Figure-4) for consecutive cases to “hard-wire” your reflexes and overcome the challenges related to learning curves.

Figure-5 Intraoperative picture showing a thin strip of ILM that provides 2 long edges for peeling
ILM peeling technique would depend upon goal of surgery and surgeon’s preference. Earlier days of macular hole surgery, opinion was divided whether to peel across the hole or circumferentially until we realized the benefits of sparing fovea or edge of macular hole during peeling. Most surgeons now avoid to peel across fovea for almost all indications although there are reports that have shown very little harm in peeling over the fovea in lamellar macular holes. Some would refrain to peel over fovea in cases with LMH and epiretinal proliferation to reduce the conversion of LMH to full thickness macular hole. Detailed discussion of this aspect is beyond the scope of this write up but sparing fovea has not been shown to reduce the success rate of most macular surgeries and so can be considered for all cases.

Figure-6 Intraoperative picture showing ILM flap with temporal hinge and positioned over macular hole
After Michalowski and colleagues described ILM flaps, same was quickly adapted by retinal surgeons all over the world with lot of modifications. Lot of Surgeons have observed and reported better outcomes of Macular Hole Surgery with ILM flaps as compared to surgery with conventional ILM peeling without flaps. Creating ILM Flaps involves even more careful planning and extra caution while handling the ILM flap especially during the final phase of fluid-air exchange. Because ILM flap has a tendency to migrate towards disc, it was not long before surgeons realized the advantage of leaving the hinge temporal to macular hole (Figure-4 & 6). Other modifications include creating multiple small flaps and placing it on macular hole. In this technique, peeling is done towards center and you aim to leave multiple hinges near the edge of macular holes. Advantage of this technique is that you get multiple flaps and an “assurance” that at least one of them would cover the hole. Disadvantage is the challenge you face while manipulating multiple small flaps during last phase of FAE.
7 Size of ILM peeling
The optimal size of ILM peeling has been discussed and evaluated by multiple researchers and general consensus is to peel at least 2 DD of ILM for all macular holes and larger area for large macular holes (≥1000 µ). For large macular holes, most surgeons would peel off ILM over posterior pole area with in arcade. ILM peeling outside vascular arcade is generally not recommended and can invite complications like bleeds and tears. However, in presence of any ERM, it is advisable to peel ERM as far as possible. Cases where we have created flaps need ILM peeling in 2 circles; inner circle is for flaps and outer one is to obtain the appropriate size of peeling as planned by surgeon. Some surgeons would peel large flaps and trim it with cutter before positioning it over macular hole. This is lesser controlled maneuver than creating smaller flaps and peeling ILM in 2 circles.
8 ILM peel on fragile Retina
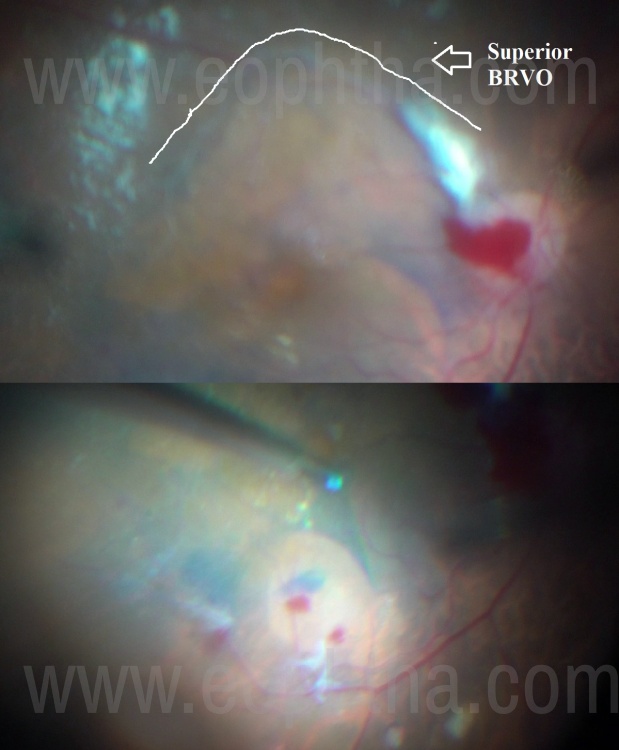
Figure-7 Intraoperative picture showing ILM peeling in case with superior BRVO. Peeling was initiated in inferior perfused area.
Peeling ILM in cases with Vasoproliferative retinal diseases can be more challenging because of multiple reasons; retina is often avascular and easy to tear, ILM is firmly adherent and media clarity can get compromised by bleeding from neovascular complexes. Few modifications that can help are; start in a relatively less affected area that is better perfused (Figure-7), proceed in smaller steps (Figure-8), change the site of peel if you encounter strong adhesions, do not hesitate to leave few islands of ILM over extremely friable retina (Figure-9). Peeling can be extended to the base of NVCs to prevent future traction when NVCs regress (Figure-10). Re-staining often helps in better visualization. Avoid using any scrappers or loops over the ischemic retina. Learn to identify the “Retinal Drag” where retina tends to drag with the ILM when we are attempting to peel it (Figure-11). That’s the first sign that retina is going to tear if proceed further. At this point, just leave the ILM and come to that area from other direction and leave ILM attached at the site of strongest adhesion.
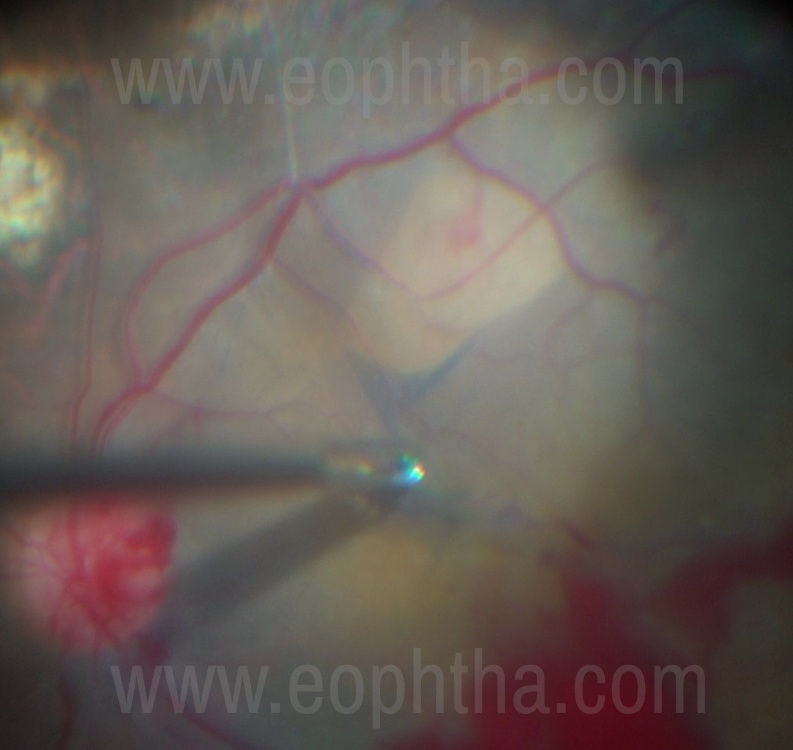
Figure-8 Intraoperative picture showing a small area peeled in patient with Diabetic retinopathy.
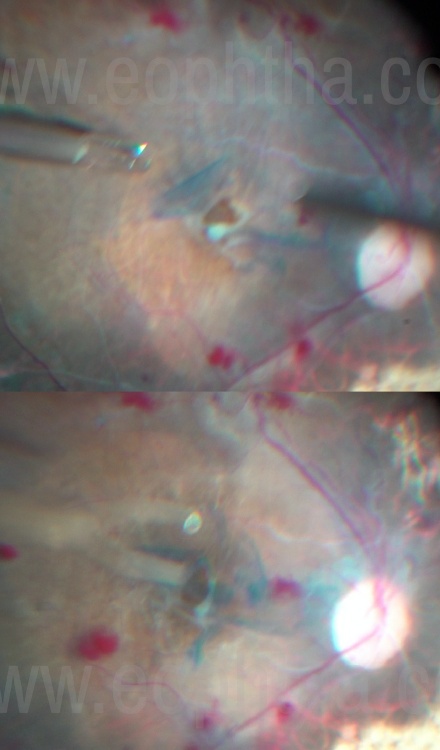
Figure-9 Intraoperative picture showing extremely friable and ischemic retina with macular hole managed by multiple small flaps of ILM.
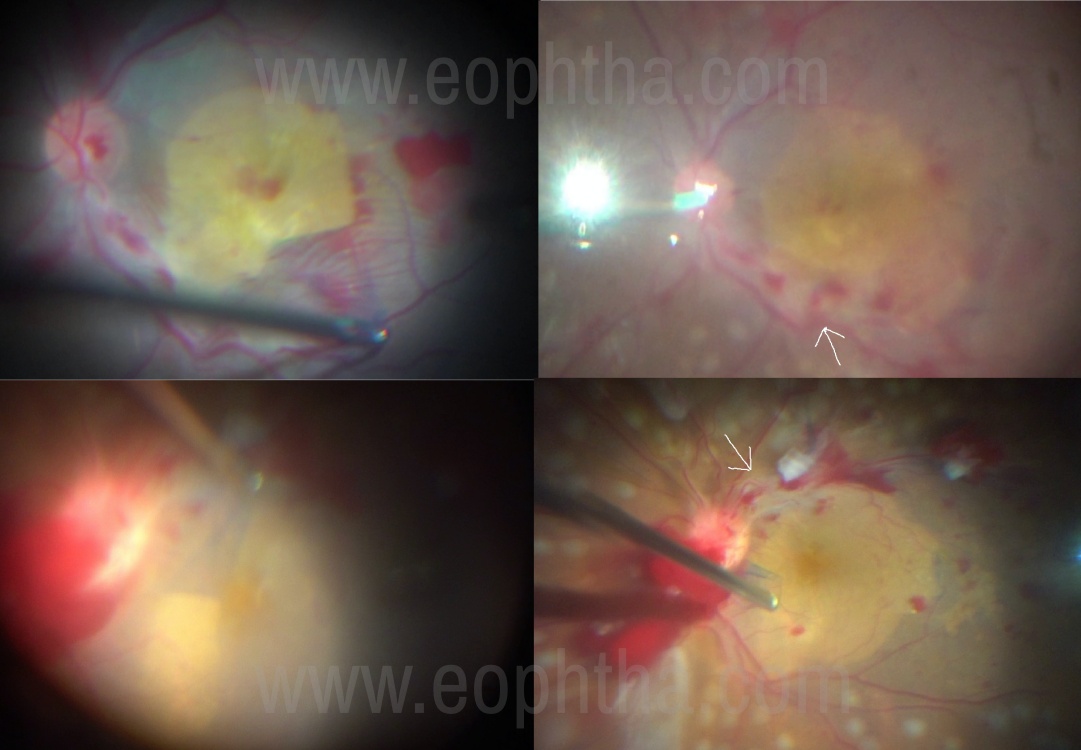
Figure-10 Intraoperative picture showing 2 eyes with PDR managed by ILM peeling. One can see Peeling extended to the base of NVC (White arrows)
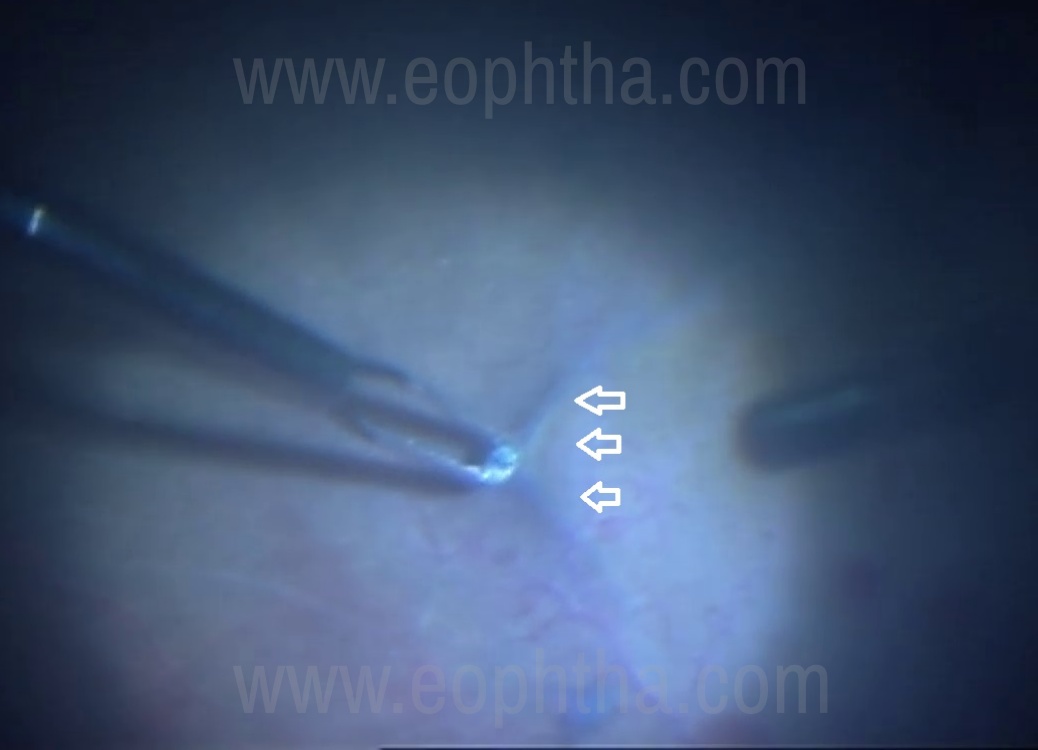
Figure-11 Intraoperative picture showing “Retinal drag” in ischemic retina during ILM peeling.
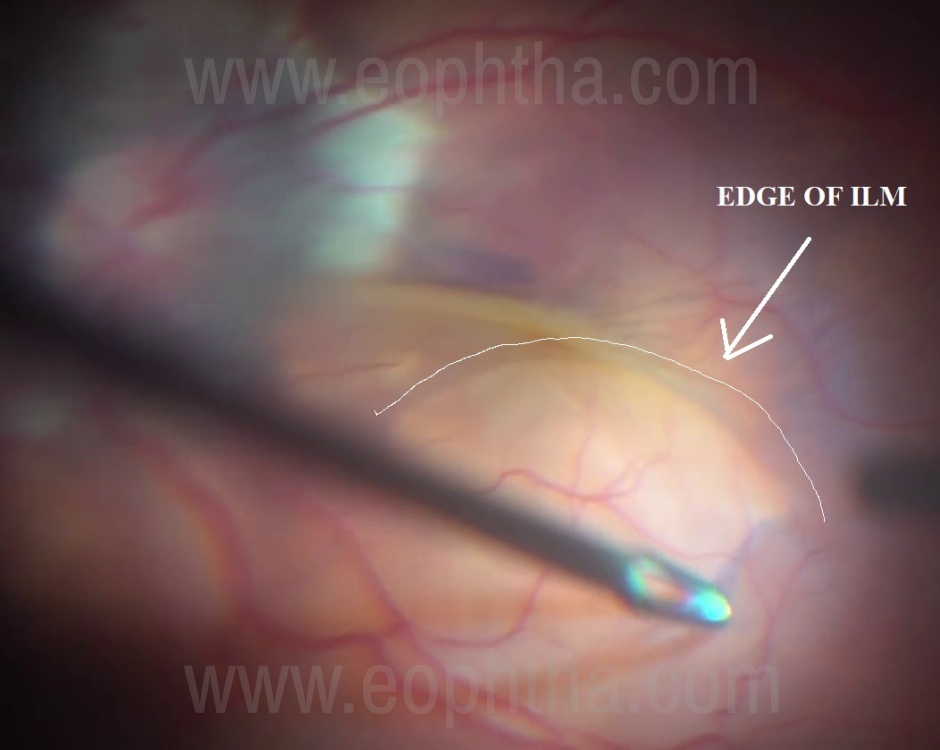
Figure-12 Intraoperative picture showing ILM peeling in a myopic eye with RRD. One can see the circular edge of the ILM in the area that has been peeled
9 Peeling in the detached retina
ILM peeling on macula off retinal detachments has been proposed to reduce the incidence of ERMs postoperatively. While there is no consensus on peeling ILM in all retinal detachments, eyes with RRD and coexisting PVR (posterior star folds) or macular holes will definitely benefit from ILM peeling. ILM peeling can be done without PFO in most eyes with RRD. Basic principles of peeling are the same here. One has to create an edge with the “PINCH” technique, peel off a thin strip, and then start peeling ILM in circles (Figure-12). Peeling in bullous retinal detachment can sometimes be challenging due to retinal mobility. Mobile retina would require repeated re-focusing of your viewing system and also does not offer any counterforce to the forceps (Figure-13). In this scenario, it often helps to drain subretinal fluid (SRF) before starting ILM peeling. Internal drainage can be repeated to flatten macula in case SRF reaccumulates. Alternatively, one can use perfluoro-octane to flatten retina before peeling.
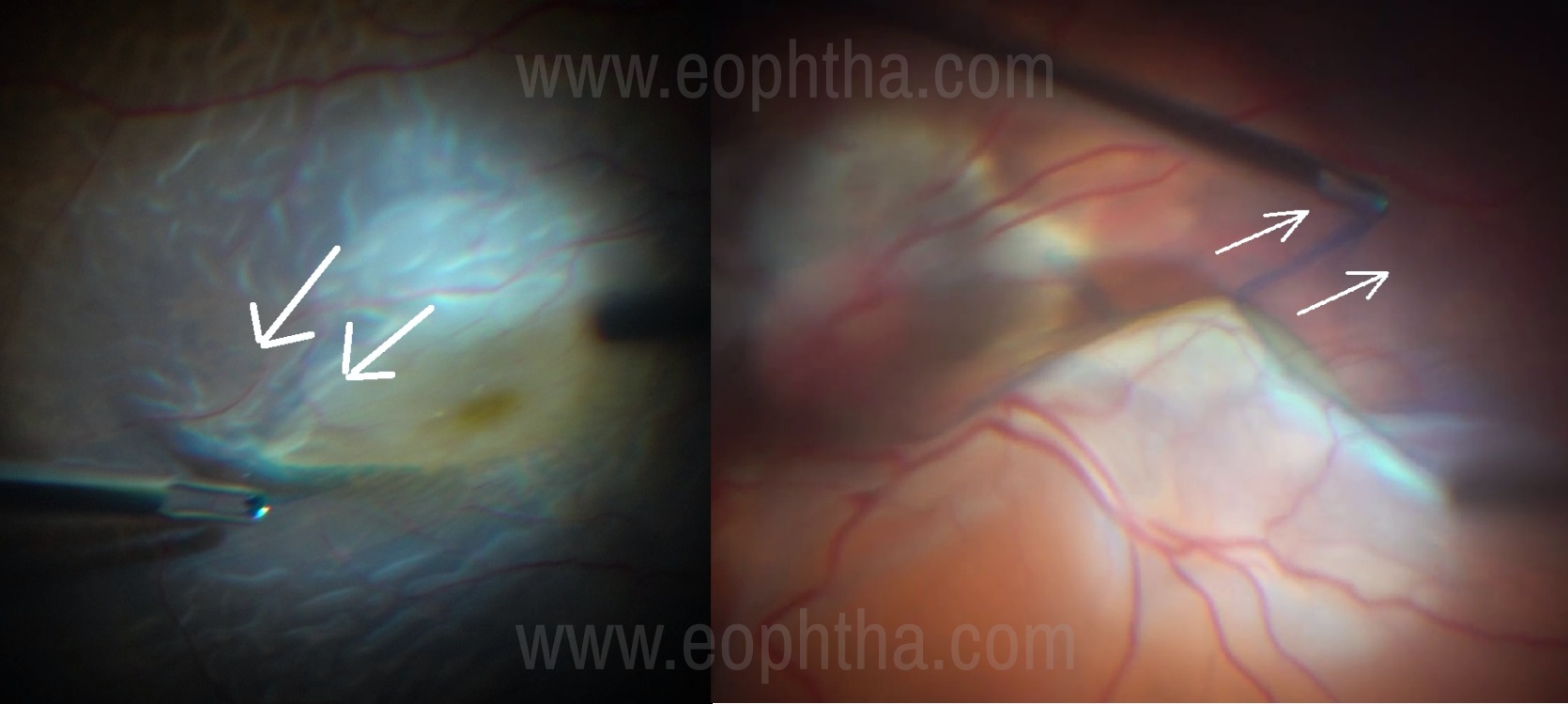
Figure-13 Intraoperative picture showing 2 cases where ILM peeling in bullous RRD is showing mobile retina being pulled towards forceps.
10 Peeling under PFO
Using PFO in eyes with RRD for ILM peeling facilitates by offers lot of advantages like getting a counterforce that pushes the retina back, reduced retinal mobility and stable view and a clear media devoid of fluid turbulences. Staining with BBG dye can easily be done under PFO. This technique is very useful for highly myopic eyes with poor contrast and staphylomas. PFO also facilitates the mobilization of “Free Flap” the technique reserved for persistent macular holes. The technique involves injecting PFO as a single bubble in a conventional manner, starting at disc and ensuring that needle stays in bubble and also allowing egress of vitreous fluid to prevent intraocular pressure from shooting up. Technique of ILM Peeling under PFO is similar to one described without PFO. Pinch technique is used to create an edge followed by peeling in a circular pattern (Figure-14). It often helps to flip the peeled flap over the unpeeled ILM to get better contrast. PFO can also be utilized to retain ILM flap in eyes with RRD and full thickness macular hole (Figure-15).
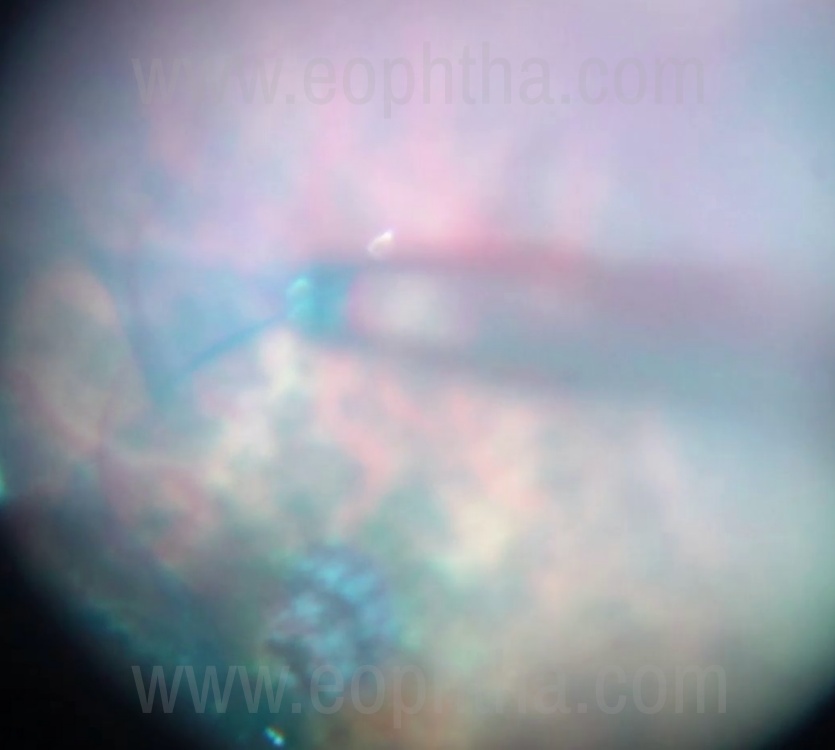
Figure-14 Intraoperative picture showing ILM peeling under PFO in a high myopic eye with RRD and Macular Hole
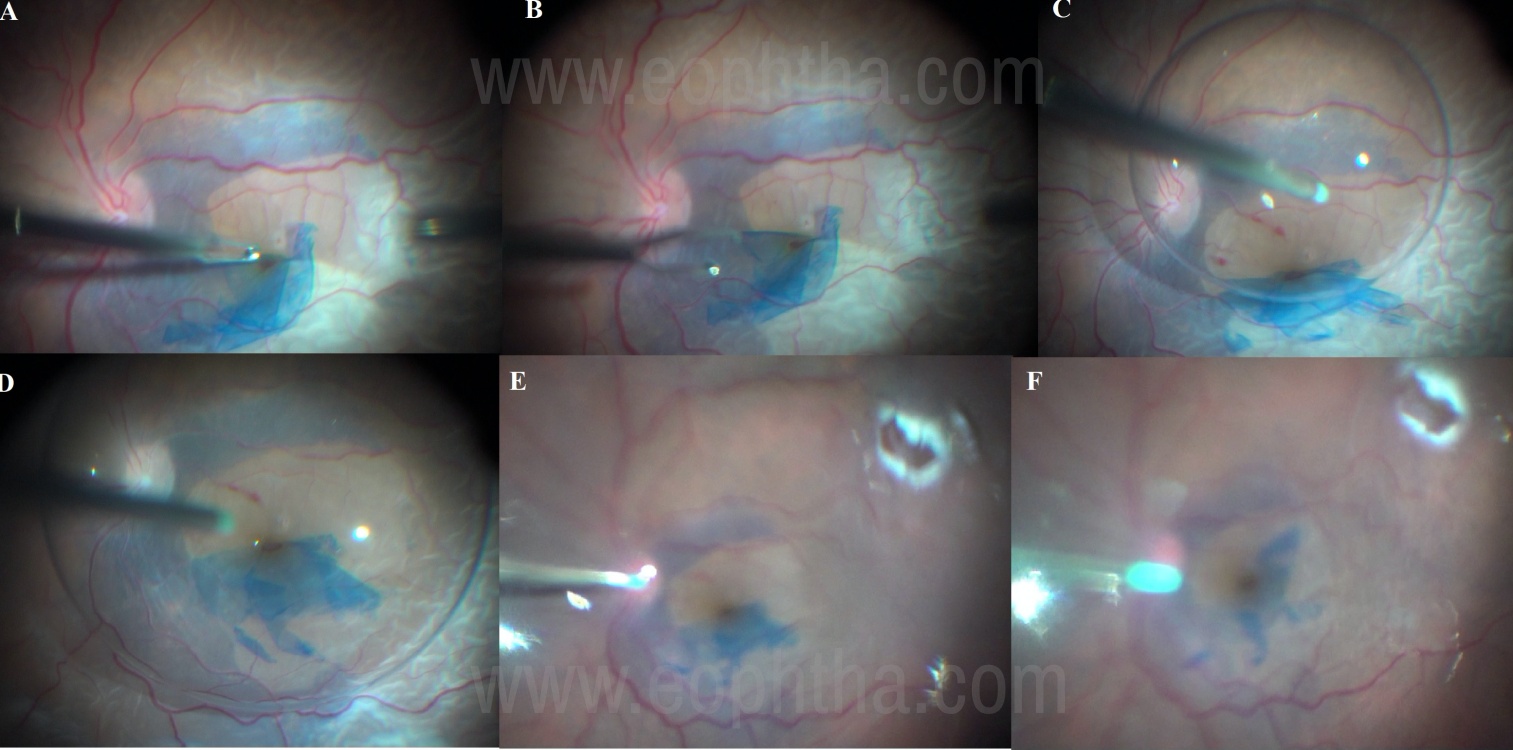
Figure-15 Intraoperative picture showing PFO being utilized to retain the ILM flap in an eye with RRD and macular hole. ILM peeling was done without PFO (Fig-15 A and B)
Difficult cases where peeling is unsuccessful or ILM is too brittle can be completed by a finesse loop or scrapper or a 27G cutter. Persistent macular hole even after successful ILM peeling can be managed by autologous free flap, where ILM flap is lifted from extramacular area and repositioned over macular hole during FAE. (Figure-16). This step can also be done under PFO.
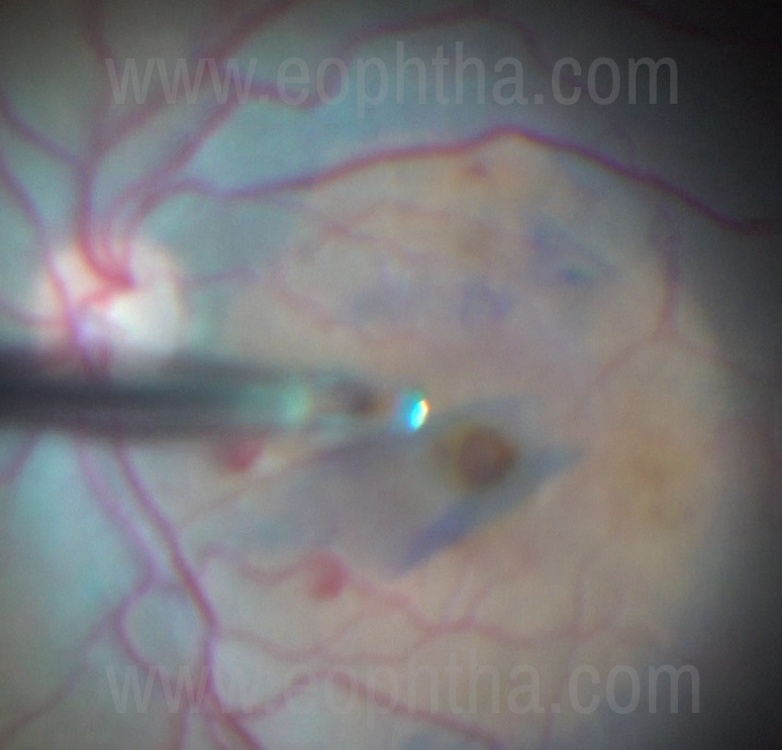
Figure-16 Intraoperative picture showing Free Flap of ILM positioned over a persistent Macular Hole.
ILM peeling is one of the most discussed and evolving retinal surgical maneuvers and has many more indications like sub-ILM hemorrhage and Optic pit maculopathy. The peeling technique is the same in these cases and needs to be repeated. 3D heads up Surgery with colored filters and image enhancement are few other exciting developments that we can look forward to.