

The management of microbial keratitis requires corneal scraping material for smear and culture. Scraping is a superficial keratectomy procedure to procure samples from central infiltrates or any infiltrate more than 2 mm in size. Stain/ wet mount gives a rapid clue to the diagnosis to initiate appropriate therapy. Inoculation of the sample on culture media help identify the offending organism and antibiogram help choose an appropriate therapeutic agent.
Erasmus Darwin the grandfather of Charles Darwin was the first to suggest corneal therapeutic debridement to try and make cornea transparent in 1795.
1. Proper documentation of corneal ulcer should be done before going ahead with corneal scraping
Before corneal scraping is planned it is important to document the corneal ulcer either diagrammatically or by photo documentation as this helps in showing progression or worsening of the therapeutic management. Areas of clinically active margins should be noted and always check the area of maximum thinning or impending perforation, to avoid excess manipulation leading to perforation.
2. Explain the patient about the procedure and use proper instruments for corneal scraping
The patient should be explained the steps of the procedure and the need for doing the scraping. Scraping material is obtained with aid of the following instruments
- 26 –g needle
- Kimura Platinum spatula
- Hyopdermic needle
- Calcium alginate swab
- 15-0 surgical blade on a Bard-Parkerhandle
- Bard-Parker Blade #57
In routine practice, a 15-0 surgical blade is preferred as it is disposable, sterile, and easy to use with a handle. Needles are not usually preferred due to the risk of perforation.
Spatulas have to be resterilized between specimen collection. Spatula is sterilized by flaming and cooling or wiping with 70% ethyl alcohol and drying. The advantage of kimura spatula is it has blunt edges and leaver smoother corneal surface.
3. Make the patient comfortable before starting the procedure
The patient is seated comfortably on the slit lamp. Apply anesthetic drops 0.5% proparacaine in the inferior fornix and wait for 1 minute. Anesthetic proparacaine is most preferred as it is least bactericidal and repeat the anesthetic drops if necessary and wipe off excess tears.
4. Reassurance is the key
Always reassure the patient to co-operate. This ensures the patient doesn’t blink often so that lashes and lids do not contaminate the specimen. Corneal scraping should be done under the slit lamp with light in dim to moderate illumination to avoid reflex tearing. Separate the lids with the non-dominant hand or use a wire speculum for better access.
5. Collection of the sample in the correct way
Purulent material and debris around the infiltrate is removed either by a sterile blade or sterile cotton bud and discarded. Scrape the edges and base of the infiltrate. Identify the active edge and scrape this region more. Exert mild to moderate pressure with the blade perpendicular to the surface of the cornea. Make multiple strokes in a single direction. Avoid areas of thinning and keep the tip of the blade away from these locations.
6.Transfer of collected sample to the glass slides
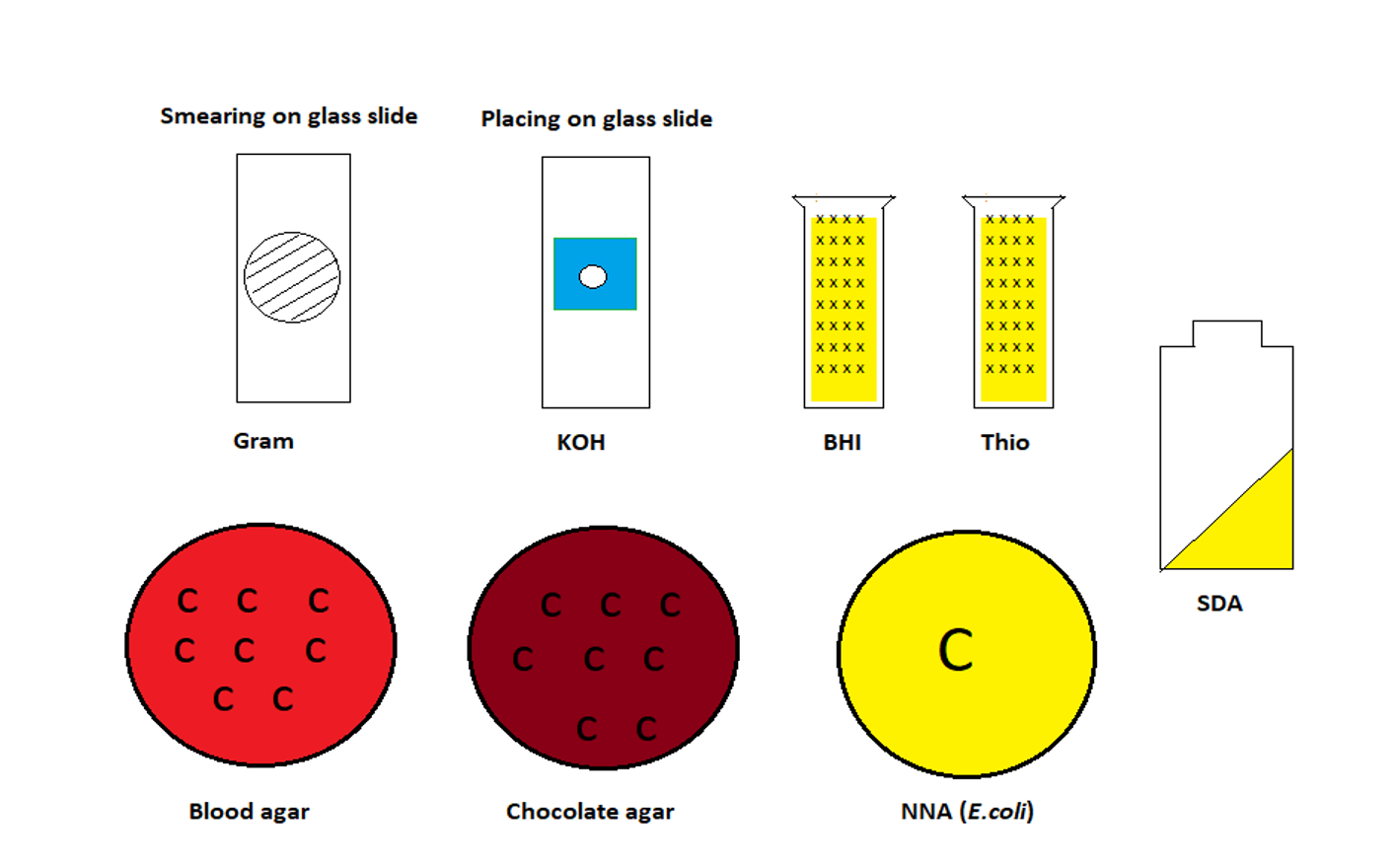
For direct smears, all-glass slides should be sterile and premarked with a wax pencil on the undersurface in the center of the slide. 3-4 smears are taken on clean glass slides within an area defined with a wax pencil on the reverse in the sequence as shown in Table 1. After direct smear, the blades are discarded. The smear should be placed in the center of the premarked zone. Ensure the marked slide has an identification name/number.
7. Always try to make an ideal smear
For Grams staining spread the smear as thin as possible on the premarked zone. For KOH wet mount, place the smear sample at the center of the marked area and place 1 drop of freshly prepared 10% KOH and immediately cover with a coverslip. In certain laboratories along with 10%KOH Calcofluor white is added to aid the identification of fungi under fluorescence microscope. Additional smears like Giemsa and Acid-fast smears are taken when necessary.
|
1 |
Potassium hydroxide (KOH) ± Calcoflour White |
|
2 |
Gram Stain |
|
3 |
Geimsa Stain |
|
4 |
Special stains - Ziehl Neelsen Acid Fast Stain or Immunoflorescent staining for chlamydiae and viruses (the smears taken for immunoflorescent staining are immediately fixed either in cold acetone or in 95%alcohol). |
|
5 |
Optional Special stains like Periodic Acid Schiff (PAS) stain or Gomori Methenamine silver (GMS) stain. |
Table 1: Sequence of direct smears for processing of clinical samples of suspected infectious keratitis samples
8. Inoculation of culture media
Scraping for smears is followed by direct inoculation of culture media with a fresh blade. Several scrapings are collected and used in a sequence to innoculate culture media as given in Table 2. Inoculate the culture media with `C` streaks without cutting the media and move the flat end of the blade along the surface of the culture plate. Always apply fresh specimens on the agar for each `C` streak. For Non-nutrient agar (NNA), place the sample in the center of the agar plate and add a few drops of Escherichia coli. For inoculating liquid medium, the scraping material is swirled or gently agitated to dislodge the specimen into the media. For viral and chlamydial cultures, corneal scrapings are collected in Hanks Balanced Salt Solution (HBSS) and sent to the laboratory immediately. In case of delay, the specimens are stored at -20°C for viral and chlamydial isolations.
|
Culture media used |
Incubation period and conditions of growth for culture media |
Isolated organism |
|||
|
Temperature (°C) |
Atmosphere |
Period (Days) |
|||
|
1 |
Blood agar |
35 |
Aerobic |
10 |
Aerobic bacteria at 35 °C and Saprophytic fungi at room temperature |
|
2 |
Brucella Blood agar |
35 |
Aerobic |
10 |
Obligate anearobes |
|
3 |
Chocolate agar |
35 |
5-10% CO2 |
10 |
Hemophilus, moraxella and Neisseria |
|
4 |
Sabouraud’s Dextrose agar |
25 |
Aerobic |
15 |
Fungi |
|
5 |
MacConkey agar |
35 |
Aerobic |
10 |
Identifies lactose fermentors |
|
6 |
Brain Heart Infusion broth |
25 |
Aerobic |
10 |
Fastidious organisms/ fungi |
|
7 |
Thioglycolate broth/ Roberson cooked meat medium |
35 |
Aerobic |
10 |
Aerobic + Anaerobic bacteria Saprophytic fungi |
|
Optional Culture Media: |
|||||
|
8 |
Lowenstein Jensen medium/ Kirchmer’s liquid medium |
35 |
Aerobic |
21 |
Mycobacteria tubeculosis |
|
9 |
Non-nutrient agar with E. coli overlay |
30 |
Aerobic |
10 |
Acanthamoeba |
Table 2: Sequence of culture media for processing of clinical samples of suspected infectious keratitis samples
9. Other samples to be sent for microbiology along with corneal scraping
Culture positive rates may differ due to prior use of antibiotics/ antifungals, deep-seated lesions, inadequate samples, and improper inoculation techniques. In addition to corneal scraping foreign body embedded in the infiltrate, loose sutures and contact lenses/solutions are also sent for microbiological investigation.
10. Dealing with special situations
- Uncooperative patients: Procedure planned under local anesthesia
- Paediatric/highly uncooperative patients: Prefer to proceed under general anesthesia
- Associated descemetoceole: Plan under local/ general anesthesia and perform tissue glue and place a bandage contact lens
- Deep-seated infiltrate: Use a disposable skin biopsy punch and trephine the specimen. Cut the specimen in two 2 equal halves. Send one to microbiology and other to histopathology. Alternatively, a flap is raised over the infiltrate with a hinge and the base of the infiltrate is scraped. The flap is reposited and either a suture is placed or glue is applied to the edges.