

SICS is the most commonly performed cataract surgery by young budding surgeons. Young postgraduates are introduced to the world of ophthalmological surgery via SICS. Initially, every new surgeon struggles to make good scleral tunnel and capsulorhexis. These TOP TEN pearls will make young surgeons confident to achieve textbook tunnel.
1. Good Visualization:
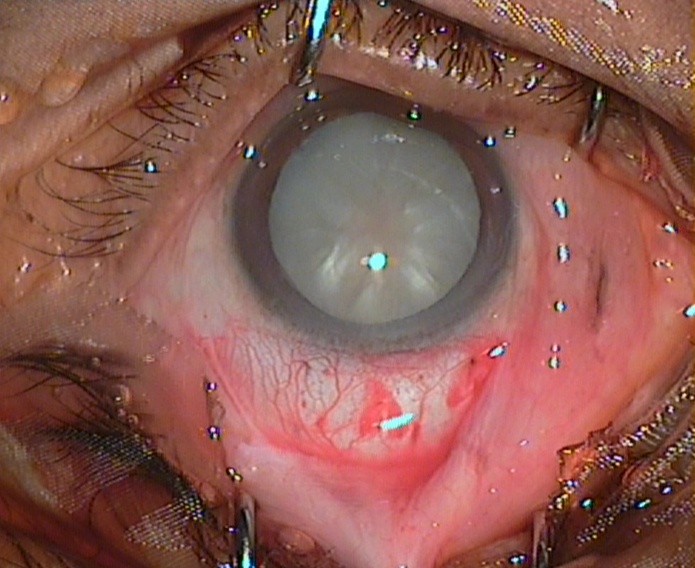
If you can see well, you can do well. Proper exposure of working field is a must. So, focus on to make adequate Conjunctiva and tenon’s dissection, avoid pooling of blood with judicious cautery and don’t let saline or visco to pool.
2. Superior rectus bridle suture: Mind the rectus
It is probably one of the most important step in SICS. It is the first step any beginner surgeon learns, but it has not been given the due credit. It is a hidden player in tunnel construction. Furthermore, it provides the globe with sufficient traction and support to construct the tunnel seamlessly.
3. Tight globe : Tight, the base
Tight globe provides support to the tunnel construction. It acts as a counter traction or a strong base to work on. At any given point if one feels the globe has become soft- identify the cause it could be a premature entry or even worse globe perforation. In any cases one need to stabilize the anterior chamber with visco via side-port and only after that can proceed further.
4. Incision Parameters : Parameters are very critical
Accuracy of scleral incision will govern the next steps; if it goes wrong then a cascade of events come uninvited like falling dominos, etc. So, be careful and strictly adhere to the following parameters
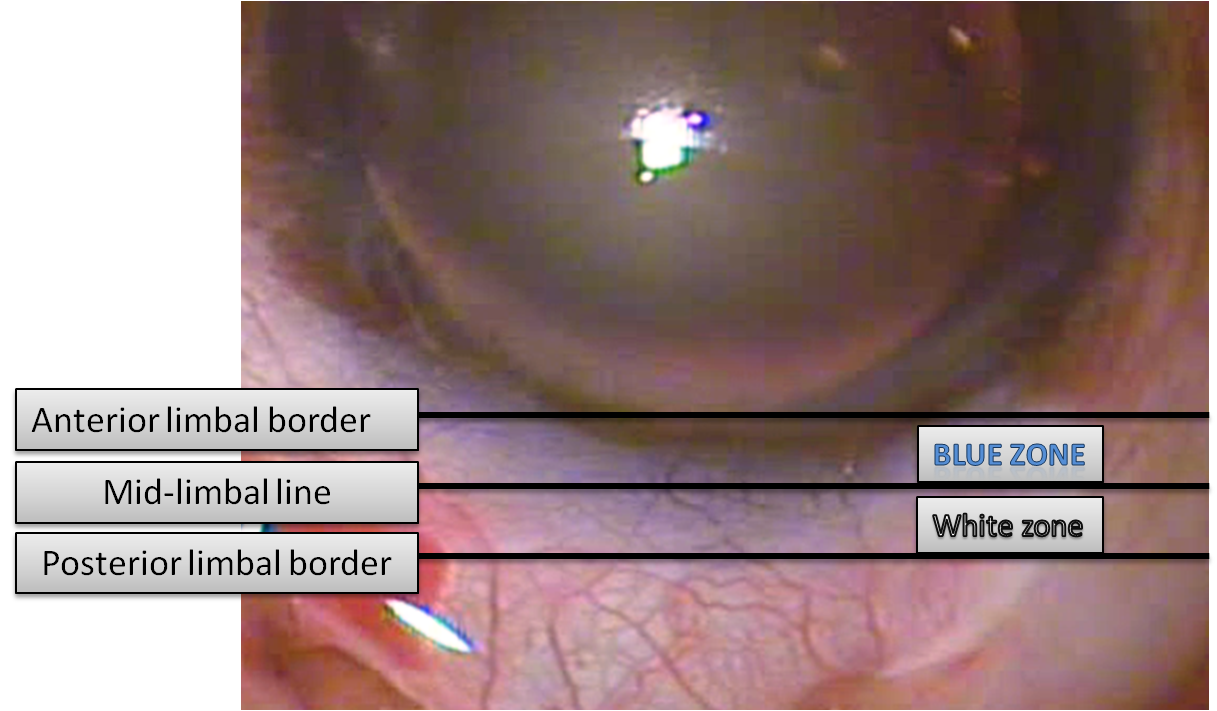
Location: Incision should be placed just adjacent to the Blue zone of limbus, but should never go over the blue zone
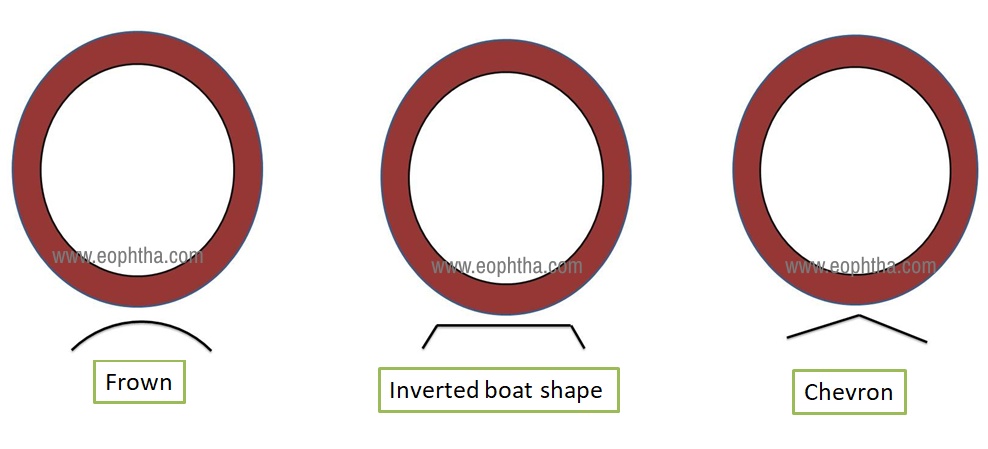
Shape: It's ideal and preferable to have frowned shape incision as it is astigmatically neutral

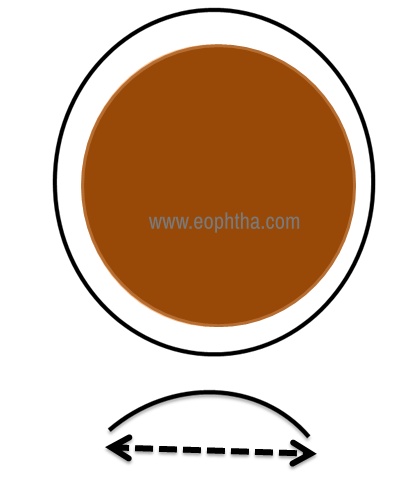
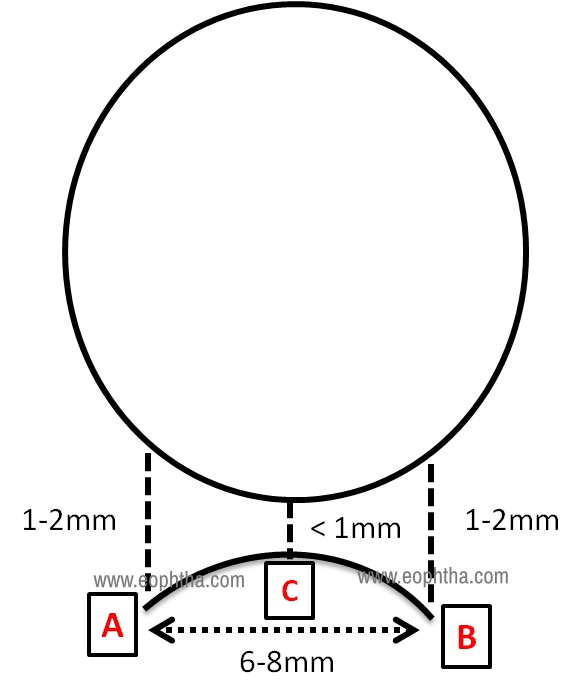
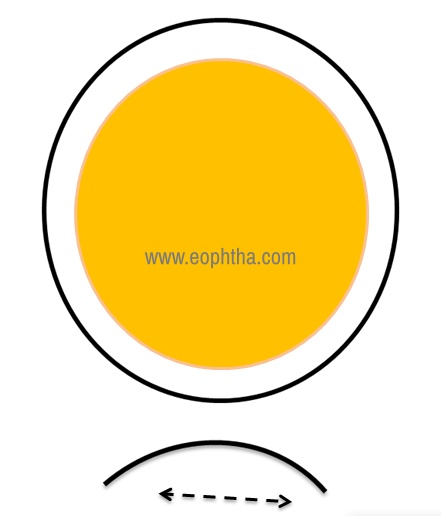
Size: It depends majorly on the nucleus size, ranging from 7-9 mm
Hard Brown Nucleus = Bigger Incision
Soft Nucleus = Smaller Incision
Depth: Similarly depth of incision plays a very important role
Very Deep Incision = Premature Entry
Superficial Incision = Buttonhole
5. Plane of tunnel construction:Sweep it before you start it:
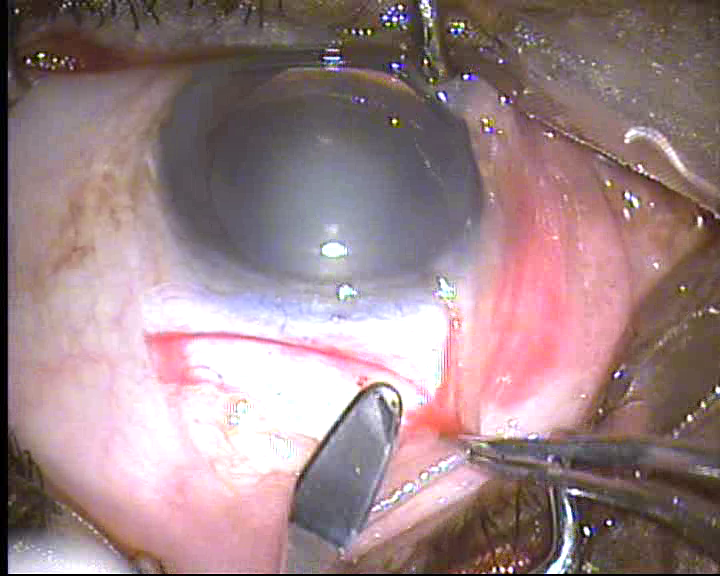
It is very important to sweep the tunnel and find dissection plane with crescent knife, before starting the tunnel construction. This is a very important step that is unknowingly neglected
6. Starting site preference: Say no to start at the centre:
While making a tunnel, the most common site to start is at the centre of incision and after that surgeon sweeps towards right and left side. Everyone has a weak side, i.e. tends to make complications on one side while extending. So, to avoid this one can start on the weaker side, for example if you start on centre and tends to make premature or buttonhole on Right end of the tunnel then it would be great idea to start on right extreme end. This way, only side pockets needs to be made and rest of the tunnel can be constructed by hand movements on your strong side.
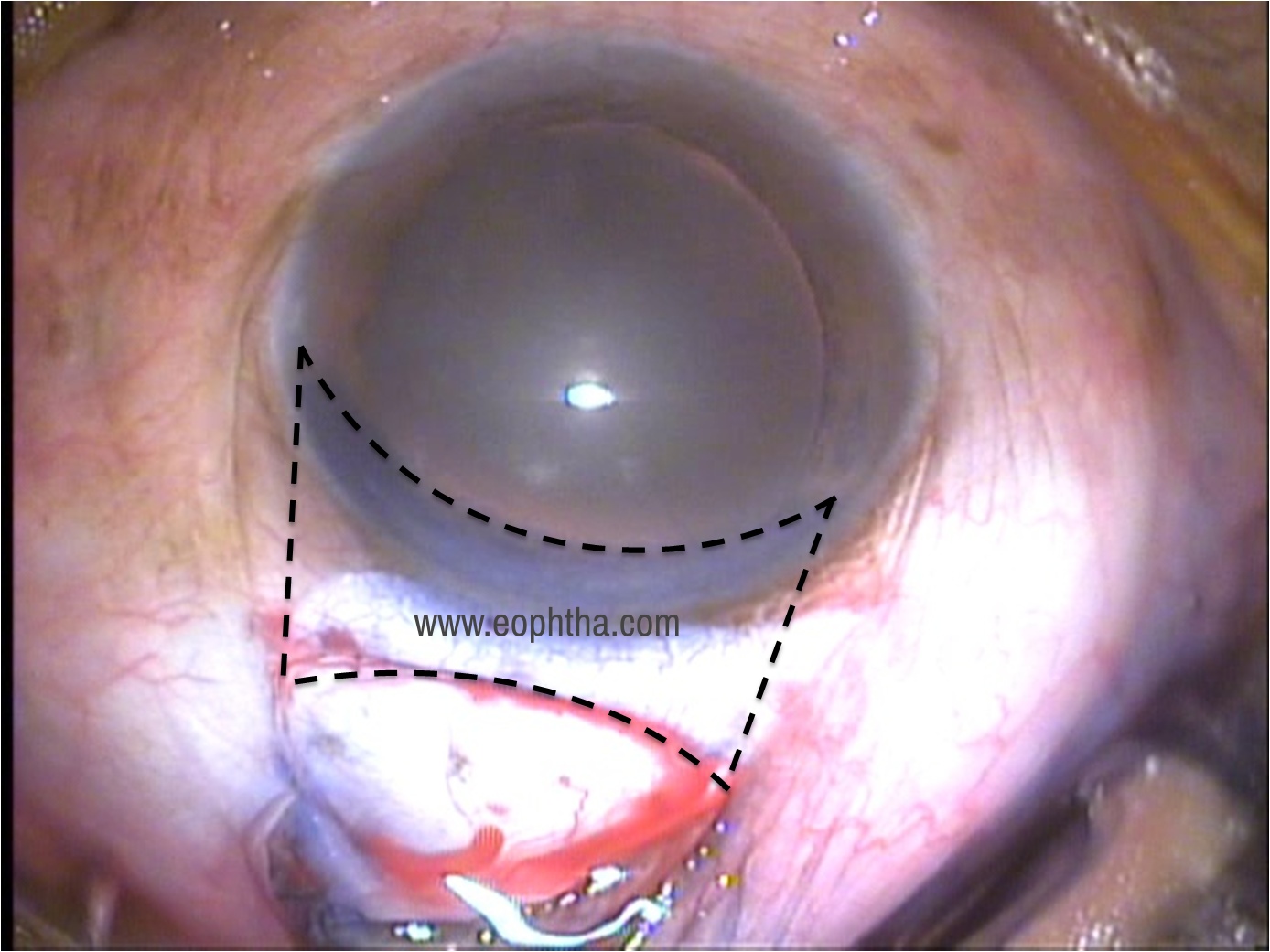
7. Adequate width of tunnel & Side pockets :Plan the width
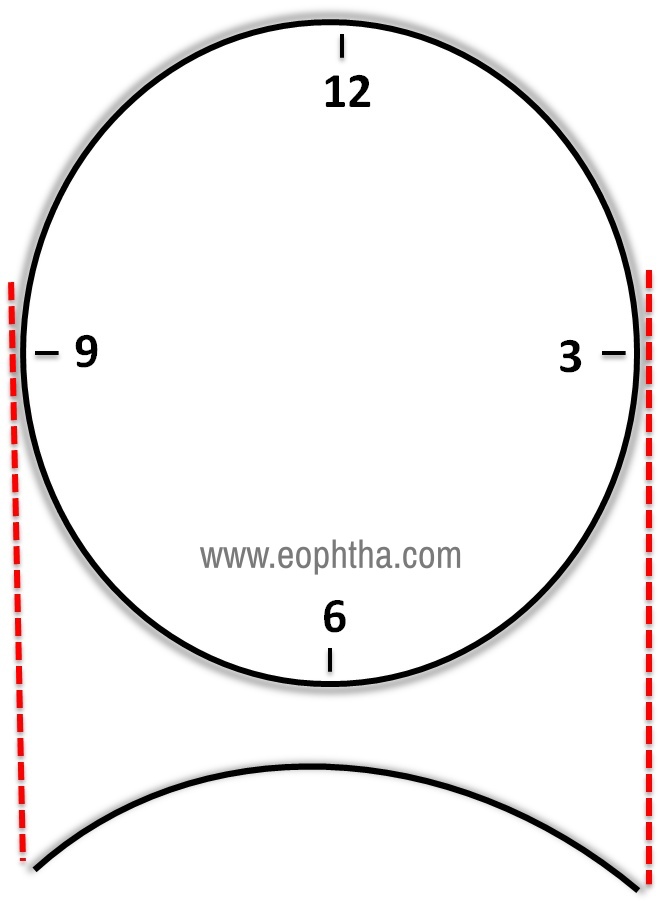
Width of tunnel plays an important role in nucleus delivery, especially in hard brown cataract. A narrow tunnel will not allow the nucleus to delivery; it will get stuck and can cause endothelium damage, descemet's detachment, etc.
So to eliminate this problem, one can draw an imaginary line from the 3 and 9 O’ clock, then this line can be an estimate of width of tunnel.
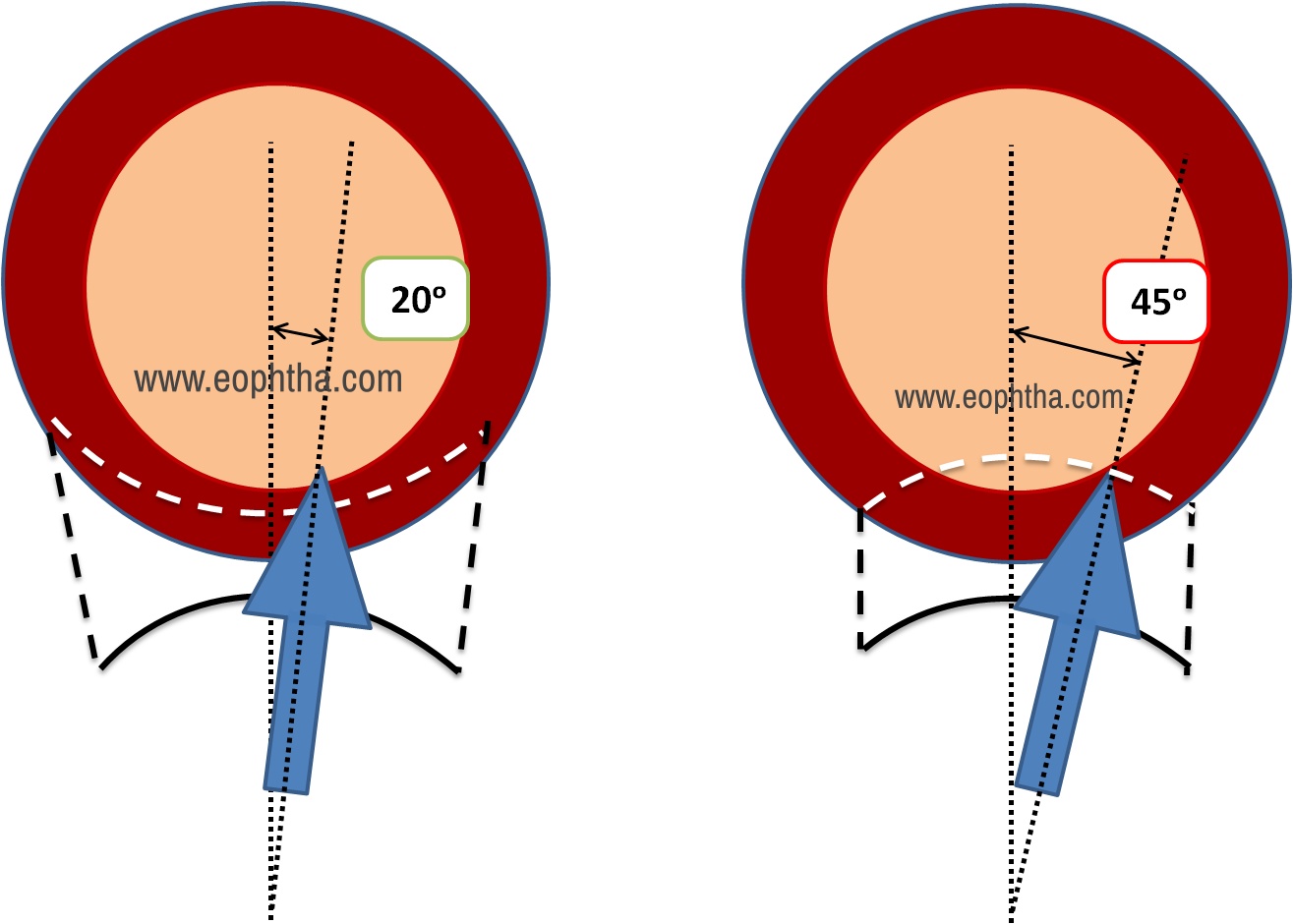
8. Keep It straight: No tilting please
While making tunnel one should avoid tilting the crescent knife otherwise it may lead to posterior scleral tear or irregular tunnel.
Similarly, even when you do keratome entry, avoid too much tilting as it may lead to frown shaped internal entry instead of a smile shaped, it will cause trouble in AC formation at the end.
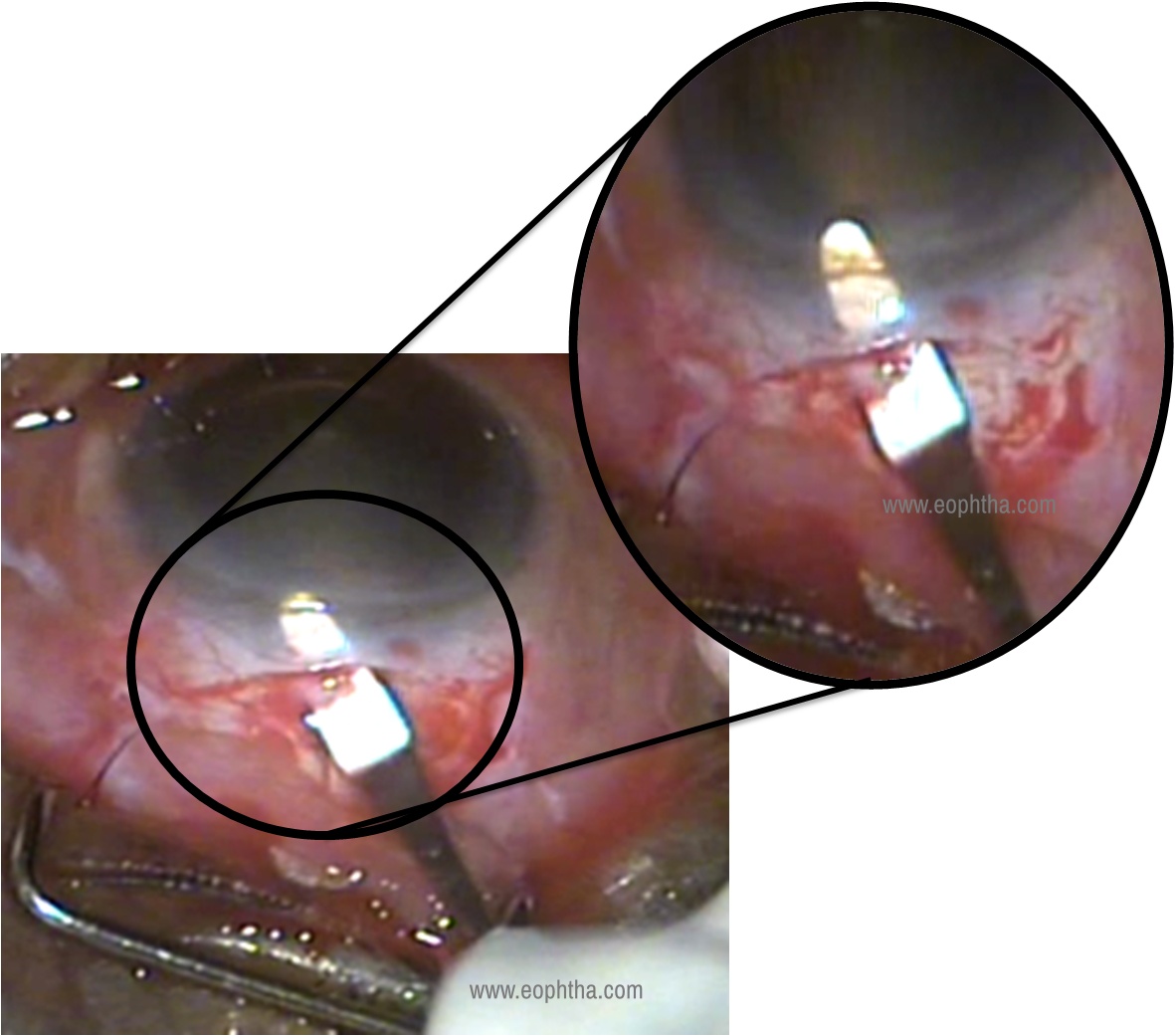
9. Keratome entry : Enter the right way
Identifying the end of the tunnel and making the keratome entry at the end is very crucial. In cases where tunnel construction was good but still you face complications like iris prolapse or difficulty in AC formation, then the problem lies in keratome entry. In that case, probably the keratome entry was done prematurely and not at the end of the tunnel.
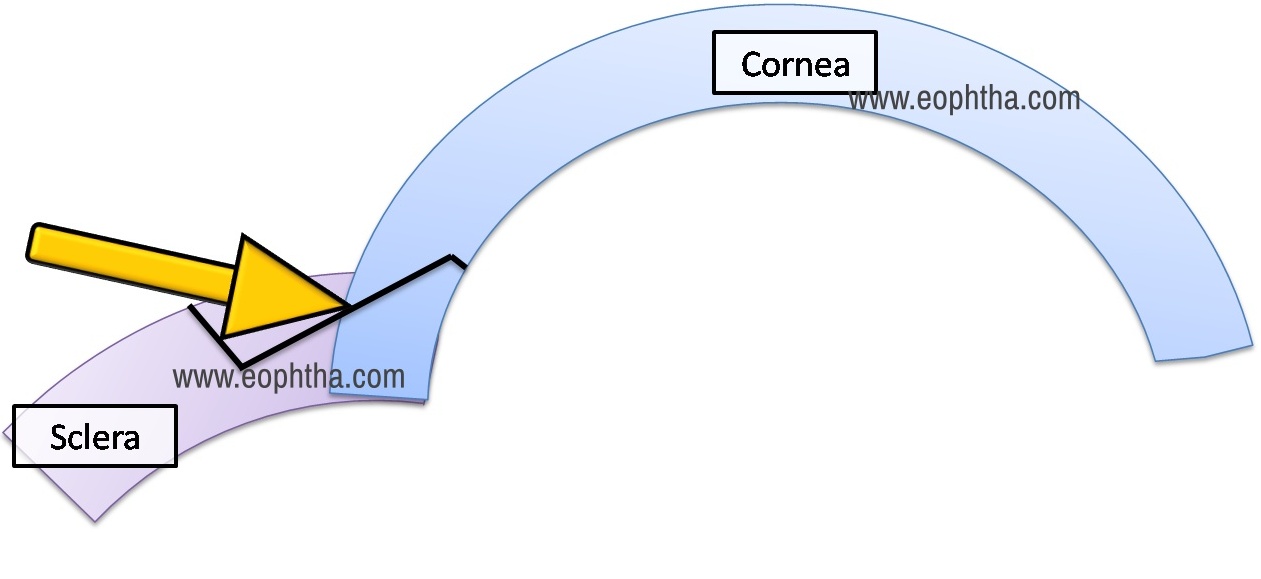
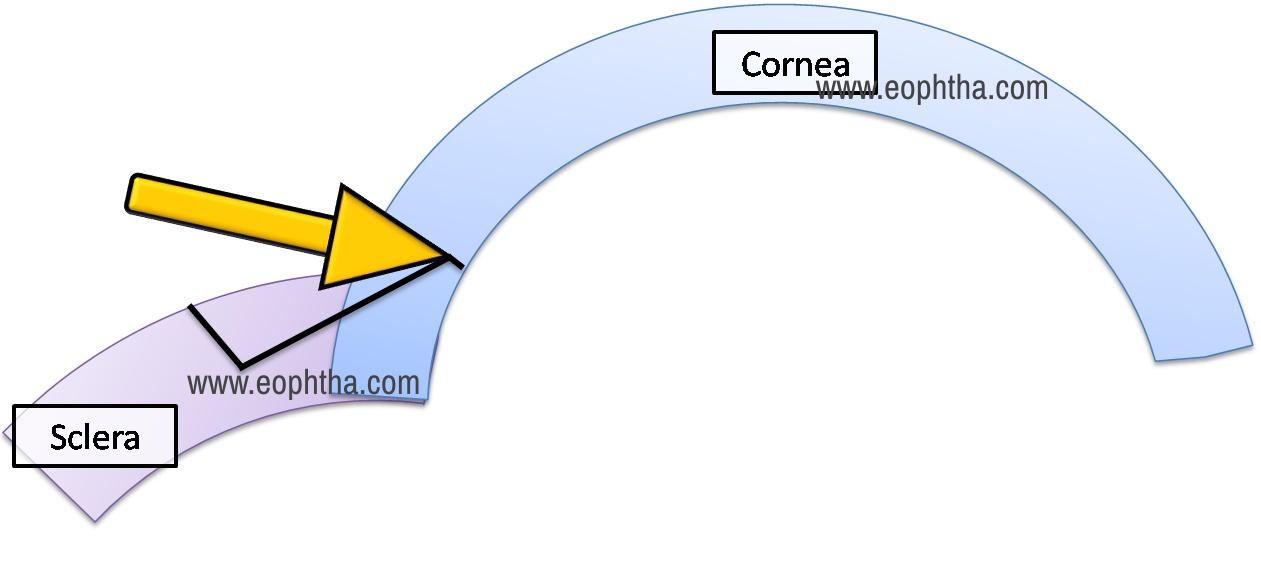
10. Cut while going in forward motion: Mind the move
Keratome moving directions while extending is also very important. One needs to extend the entry on moving inside, simultaneously moving the keratome in forward direction.
This is the only way to achieve smile shaped internal opening
COUNT THE PEARLS AND CARRY ON CONFIDENTLY.