
A 65-year-old male presented to the OPD with complaints of painless, gradually progressive dimunision of vision of the right eye over several months.
History of Present Illness:
The Patient was apparently normal 1 year ago since when he noticed dimunision of vision of the right eye by closing the left eye by chance. The vision progressively got worse. No h/o pain, watering, halos, glare or double vision.
Past Ocular History:
No H/o trauma or ocular surgery.
Past Medical History/ History of Medication:
No systemic illnesses. No H/O taking any steroids or long term medications
Family History:
Not significant. No family history of glaucoma.
Review of Systems/Systemic Examination:
Normal. Vitals were normal.
OCULAR EXAMINATION
Best Corrected Visual Acuity (Snellen)
- Right eye (OD): 6/60
- Left eye (OS): 6/9
Ocular Motility/Alignment:
Full, free, and painless in all gazes.
Intraocular Pressure (IOP)
- OD: 55mmHg (@ 2pm using Goldmann Applanation Tonometry)
- OS: 19mmHg (@ 2pm using Goldmann Applanation Tonometry)
Pupils:
Round, reacting to light in both eyes. Grade 1 RAPD noted in the right eye. Dilates poorly in right eye.
Confrontation visual fields: Full
Slit-lamp exam:
|
OD |
OS |
|
|
Lids/lashes |
Normal |
Normal |
|
Conjunctiva/Sclera |
Normal |
Normal |
|
Cornea |
Clear |
Clear |
|
Anterior chamber |
Normal depth, quiet |
Normal depth, quiet |
|
Iris |
Fine flaky white material can be seen on the pupillary border of the iris. Moth-eaten peripupillary transillumination defects of the iris could also be seen on retroillumination. |
Normal colour and pattern |
|
Lens |
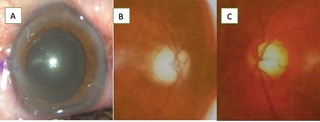
Grade 3 nuclear sclerosis. The white flaky disc is seen on anterior lens capsule after dilatation. (Fig A) |
Grade 1 nuclear sclerosis. |
|
Gonioscopy |
All quadrants open till scleral spur. Irregular blotchy pigmentation of the trabecular meshwork. Sampolesi line noted. |
All quadrants open till scleral spur(SS). |
Dilated Fundus examination
|
OD |
OS |
|
|
Vitreous |
Clear |
Clear |
|
Disc |
Average-sized disc. C:D 0.8, bipolar neuroretinal rim(NRR) excavation. (Fig 1B) |
Average-sized disc. C:D 0.65 bipolar sloping NRR. (Fig 1C) |
|
Macula |
FR+ |
FR+ |
|
Vessels |
Normal calibre. A:V ratio 2:4 |
Normal calibre. A:V ratio 2:4 |
|
Periphery |
Normal |
Normal |
Ancillary Investigations:
Humphrey Visual fields:
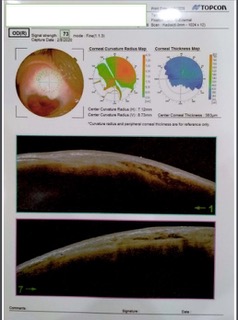
Visual fields using SITA Standard 24-2 and 10-2 were suggestive of advanced glaucomatous damage in the right eye(Fig 2 A&B) and normal fields in the left eye.(Fig 2C)

Optical coherence tomography:
OD: Superior and inferior retinal nerve fibre layer(RNFL) thinning, correlated with clinical disc findings(Fig 2D).
OS: Bipolar borderline RNFL thinning(Fig 2D)
Optic disc photography:
Disc photographs of the patient were also taken for documentation purposes. (Fig 1 B&C)
Pachymetry :
OD 564um, OS 567um
Diagnosis:
Based on the typical clinical picture, a diagnosis of Exfoliation Glaucoma was made in the right eye with Grade 3 nuclear sclerosis. Left eye has Grade 1 nuclear sclerosis.
Differential Diagnosis of unilateral glaucoma:
- Pigmentary glaucoma
- Uveitic glaucoma
- Capsular delamination/True exfoliation
- Acute angle-closure glaucoma
- Asymmetric primary open-angle glaucoma
- Traumatic glaucoma
- Neovascular glaucoma
- Primary amyloidosis
- Fuchs heterochromic uveitis
Clinical Course of the condition:
This patient presented with unilateral advanced exfoliation glaucoma with a visually significant cataract. She had gradually progressive diminution of vision due to progressive cataracts and glaucoma. Since IOP of 55mmHg was gradually attained, it was painless unlike an acute attack of high pressures. Due to significant cataracts and advanced glaucoma in the right eye, combined Phacoemulsification and Trabeculectomy with Mitomycin C under Local anesthesia was planned for the patient after discussing the pros and cons of the procedure and taking high-risk consent. The patient’s 1-month BCVA was 6/6 with an IOP of 12mmHg. IOL was well centered. Bleb was well-formed, low lying, and diffuse(Fig 3). The left eye was kept under monitoring since diurnal IOP and visual fields were normal. The patient was explained the need for regular follow-up owing to the possibility of future development of ocular hypertension/glaucoma in the left eye.
DISCUSSION
Definition:
Exfoliation syndrome (XFS), previously known as pseudoexfoliation syndrome, is an age-related disease characterized by the production and progressive accumulation of fibrillar extracellular material in ocular tissues throughout the anterior segment like the lens, ciliary body, zonules, iris, trabecular meshwork, corneal endothelium, conjunctiva, and orbital structures. It can cause secondary open-angle glaucoma, angle-closure glaucoma (Exfoliation glaucoma), or Ocular Hypertension.
Epidemiology:
- Leading cause of unilateral glaucoma in the elderly.
- Incidence: 2-200 per 100,000 with increased incidence with age.1
- Exfoliation glaucoma occurs more commonly in eyes with XFS than in those without it, about six times more2.
- Exfoliation syndrome is three times more common in females than males2.
- Clusters in some regions eg. Scandinavia
- Age: elderly
- The reported prevalences in different parts of the world have varied from 0% to 38% in different populations3-6.
- Studies done in South India report a higher prevalence of XFS in rural population ~3.8% of which 13% have XFG.7
Etiology:
- Defects in elastin metabolism have been proposed to be responsible for the synthesis of exfoliative material since association with specific mutations of the lysyl oxidase-like protein 1(LOXL1) gene, which is important in elastin metabolism, is strongly associated with XFS and exfoliation glaucoma(XFG).
- Environmental factors also play a role in those who are genetically susceptible.
Pathophysiology
- Exfoliative material can be identified with transmission electron microscopy which shows fibrillar elastotic material.
- Histochemically, it is made of glycoconjugates surrounding a protein core.
- The origin of exfoliative material is unclear; however, evidence suggests emergence from intraocular cells (trabecular and corneal endothelium, ciliary and lens epithelium and iris) and extraocular cells (fibrocytes, vascular and muscle)8. This is thought to be a result of oxidative stress.
- Glaucoma in pseudoexfoliation can exhibit as open-angle or angle-closure glaucoma.
- Blockage of the trabecular spaces by XFM promotes accumulation of pigment and cellular debris in the juxtacanalicular tissue, which causes obstruction of the aqueous channels and limits access to the Schlemm canal that leads to narrowing of the canal lumen, the collapse of its walls, disruption of its endothelium, and partial obliteration causing open-angle glaucoma.
- Mechanism of angle-closure glaucoma is zonular laxity allowing forward movement of the lens, causing decreased anterior chamber depth and pupillary or angle closure.
Clinical Features
- Patients presenting with XFS may be asymptomatic, or they may complain of decreased visual acuity secondary to cataracts or glaucomatous visual field changes.
- Rarely occurs before 50yrs of age and the incidence increases steadily with age.
- XFS typically presents unilaterally. The fellow eye develops signs of exfoliation in more than 40% of cases9.
- Exfoliation syndrome is essentially a clinical diagnosis.
- Slit-lamp examination, including gonioscopy and pupillary dilation, represents the gold-standard procedures for the clinical diagnosis of XFS/XFG.
- Diagnosis can be made on the slit lamp examination with an 85% sensitivity and a 100% specificity10.
- Characteristic features are:
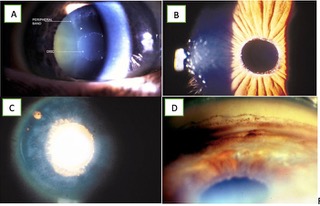
- Lens: The most commonly recognized feature is the 3-ring sign on the anterior lens capsule(Fig 4A), formed by a central disc, a peripheral ring, and a clear zone, in between. In some cases, it may be absent and only ground glass deposits on the anterior lens capsule may be seen(Fig 1A)
- Iris: Fine flaky white material can be seen on the pupillary border of the iris without dilation(Fig 4B). Physiological rubbing of iris against the lens scrapes the XFM from the surface of the lens and causes secondary pigmentary dispersion syndrome, with a loss of melanin from the iris pigment epithelium at the pupillary margin causing a sawtooth-like peripupillary iris atrophy(Fig 4C). It is best visualized using infrared transillumination.
- Pupil: Eyes with XFS often dilate poorly11. Eyes with XFS may also constrict less well to topical 4% pilocarpine12. Pigment dispersion in the anterior chamber is common after pupillary dilation and may be profuse causing marked IOP elevation13.
- Cornea: Scattered flakes of XFM may be observed on the endothelial surface of the cornea. A greater than normal frequency of cornea guttata in eyes with XFS has been suggested14.
- Zonules and Ciliary Body: Exfoliation material(XFM) may be detected earliest on the ciliary processes and zonules and this creates a tendency to spontaneous subluxation or dislocation of the crystalline lens in advanced cases.
- Anterior Chamber Angle: Gonioscopy shows a discontinuous pigmentation of the trabecular meshwork, pigment characteristically is deposited on the Schwalbe line or anterior to the Schwalbe line (the Sampaolesi line)(Fig 4D). A high incidence of narrow or occludableangles in eyes with pseudoexfoliation has been reported, sometimes with peripheral anterior synechiae.
- Optic nerve assessment: with +78D or +90D will show optic disc cupping with NRR thinning and corresponding RNFL defects. Glaucomatous changes in the optic disc are similar in pattern with POAG.
GLAUCOMA IN EXFOLIATION SYNDROME
- Glaucoma is a secondary event. Exfoliation syndrome itself does not cause optic nerve damage.
- Glaucoma in XFS has a more serious clinical course and worse prognosis than POAG.
- There is a significantly higher frequency and severity of optic nerve damage at the time of diagnosis, worse visual field damage, higher baseline IOP, greater diurnal fluctuation of IOP, poorer response to medications, more severe clinical course, more rapid progression, and more frequent necessity for surgical intervention9.
CATARACT IN EXFOLIATION SYNDROME
- Nuclear cataract is often more frequently found in eyes with XFS than in eyes without it15.
- Patients with XFS are much more prone to having complications at the time of cataract extraction9.
- Pupillary diameter and zonular fragility (and/or phacodonesis) have been suggested as the most important risk factors for capsular rupture, zonular dehiscence, vitreous loss and nucleus drop(5-10 times more common)16,17 and should serve as a warning sign to the surgeon.
- Posterior capsular opacification is more in eyes with XFS.18
- Late postoperative decentration of IOLs and capsular bags is significantly higher in eyes with XFS20.
- Capsule contraction syndrome is particularly common in eyes with XFS, particularly if the capsulorrhexis is small, and can lead to IOL displacement20.
ANCILLARY INVESTIGATIONS:
Following investigations aid in diagnosis, management, and monitoring of XFG.
- Goldmann Applanation Tonometry : Since XFG is characterized by wide fluctuations in diurnal IOP levels, single IOP measurement may be unreliable and it becomes important to monitor IOP levels at different times of the day21
- Visual Fields: are required to confirm the diagnosis of XFG. In exfoliative glaucoma, visual fields defect pattern is the same as in POAG.
- Pachymetry: for estimating central corneal thickness adjusted IOPs. Central corneal thickness is also greater in eyes with XFS, perhaps reflective of early corneal dysfunction22
- Glaucoma Imaging: Various imaging technologies like Optical coherence tomography (OCT) and confocal scanning laser ophthalmoscope (Heidelberg retina tomograph [HRT]) are also being used to document and monitor changes due to glaucomatous damage in the optic disc and the retinal nerve fibre layer. These imaging techniques are similar to those in POAG. Anterior Segment OCT can suggest the presence of any angle-closure or reduced depth of the anterior chamber.
- Serial optic disc photographs: can be done to document baseline findings and monitor progression.
The following investigations may be helpful for preoperative assessment prior to cataract surgery in patients with XFS:
- Ultrasound Biomicroscopy to diagnose any zonular laxity or lens subluxation.
- Specular microscopy can be done to ascertain reduced endothelial cell density or morphologic changes in the size and shape of the endothelial cells21.
TREATMENT
Management of XFG is guided by mechanism, stage of glaucoma, degree of IOP elevation, ocular and systemic factors and patient and care provider preferences.
Establish target IOP levels:
Patients with XFS are more likely to convert from ocular hypertension to glaucoma and have a greater baseline IOP at glaucoma diagnosis compared with POAG23. So, the target IOP range needs to be defined after diurnal/serial IOP measurements to establish baseline IOP and after determining stage of glaucoma with the help of visual fields.24
Medical management:
It is the first line of treatment. Although medical management of XFG is the same as POAG, XFG tends to respond less well to medical therapy than does POAG9.
|
Salient features in the medical management of Exfoliation Glaucoma. |
|
|
|
|
|
Lasers
- Laser trabeculoplasty can be tried if patient is unresponsive, non-compliant or intolerant to anti-glaucoma medications.
- Laser trabeculoplasty is particularly effective in XFL glaucoma owing to the relatively pigmented angles.
- The amount of IOP reduction is modest and long-term success drops to approximately 35–55% at 3–6 years 30,31.
- Eyes with XFS may have a greater post-laser inflammatory reaction than eyes without 32.
- Selective laser trabeculoplasty (SLT) has been shown to be equivalent to Argon laser trabeculoplasty in terms of lowering IOP 33.
- The advantage of SLT is that it is a repeatable procedure because it does not produce thermal damage to the trabecular meshwork.
- Laser iridotomy is the procedure of choice for angle-closure glaucoma.
- Angle-closure glaucoma caused by anterior lens movement or subluxation may benefit from argon laser peripheral iridoplasty to mechanically pull the iris away from the trabecular meshwork34.
- The role of endoscopic cyclophotocoagulation (ECP) in XFG is minimal as exfoliation material accumulates on the ciliary body and zonules, and high laser energy can result in rupture of ciliary processes with significant inadvertent haemorrhage35.
Surgery
- If IOP remains uncontrolled following medical and/or laser treatment, surgical management is warranted.
- Trabeculectomy has similar efficacy and safety outcomes in XFG as in POAG36.
- Glaucoma drainage device implantation is also an option, especially in eyes with previous conjunctival manipulation37,38.
Newer surgical options
- The adjunctive use of ExPRESS shunts have been widely talked about.
- Trabeculotomy as well as trabecular aspiration (TA) have been shown to be effective in the management of XFG.
- TA aims to improve trabecular outflow by removing pigment and exfoliative material. Trabecular aspiration combined with phacoemulsification is more effective than cataract surgery alone in reducing postoperative IOP and the necessity for antiglaucoma medication but not as effective as phaco-trabeculectomy39.
- The use of Trabectome, iStent, viscocanalostomy, but prospective studies with longer follow-up are needed before one can recommend widespread use of these and possibly other microinvasive glaucoma surgical approaches 40.
- However, given the higher mean IOP in PXFG compared to other types of glaucoma and the larger diurnal fluctuations, nonpenetrating surgeries, which are less efficient in IOP reduction, are not recommended for these patients.
CATARACT SURGERY IN EXFOLIATIVE SYNDROME
It is recommended not to delay cataract surgery. Today phacoemulsification is the most frequent procedure performed in cases of pseudoexfoliative cataract and has a lower recurrence of complications41Key recommendations to prevent complications during cataract extraction are summarised.
Pearls for Safer Cataract Surgery 42 |
|
Capsulorhexis ► Large enough to enable the nucleus to prolapse into the anterior chamber as needed in order to reduce strain on zonules. Hydrodissection ► Occasionally tap on centre of nucleus to decompress fluid pressure on weak posterior capsule. Phacoemulsification ► Prevent anterior chamber collapse and protect corneal endothelium using cohesive as well as dispersive ophthalmic viscosurgical devices (OVD). Cortical removal ► Use tangential vectors to carefully separate cortical material from capsular bag, particularly if a capsule tension ring (CTR) has been inserted. Small pupil ► Consider cohesive OVD, mechanical and pharmacological dilation (instillation of 10% phenylephrine and 0.5% tropicamide causes greater mydriasis than 2% ibopamine and a more significant dilation can be obtained through the combined use of both drugs (mean pupil diameter of 7.19 mm)) [G. L. Scuderi, F. Regine, A. Perdicchi, A. Turtoro, and M. T. Contestabile, “Efficacy of 2% ibopamine on the dilation of patients with pseudoexfoliation syndrome,”European Journal of Ophthalmology, vol. 20, no. 1, pp. 120–123, 2010. Zonular weakness► Consider CTR or capsule tension segments. If diffuse weakness, could consider intracapsular or pars plana removal. PCIOL► Posterior chamber intraocular lens is generally well tolerated. Postop ► Potential for fibrinoid reaction postoperatively due to weak blood–aqueous barrier. Postop management should include aggressive anti-inflammatory treatment with steroids and NSAIDs. |
Management of coexisting cataract and glaucoma
- In patients necessitating surgical control of IOP and visually significant cataract, a combined cataract and trabeculectomy procedure may be a good option. The decision should be weighed with caution owing to high risk of complications. Phacotrabeculectomy has similar success rates in XFG as in POAG patients.43
- The degree of IOP reduction achieved with combined surgery may be less than that of trabeculectomy with MMC alone, likely secondary to increased inflammation from concurrent cataract surgery however It is well established that cataract surgery performed following successful trabeculectomy may have an adverse impact on IOP control, leads to a higher rate of failure secondary to the introduction of inflammatory mediators into the bleb.
- The postoperative management, either after cataract, or, even more, glaucoma surgery, should involve the use of aggressive anti-inflammatory treatment with steroids and nonsteroidal medications, due to weak brain–blood barrier in PXF. 18
Follow up protocol:
- XFS patients have approximately a 40% chance of developing ocular hypertension or glaucoma within 10 years, a risk approximately a tenfold higher than that found in the general population44 hence they should have annual checkups for early detection of glaucoma.
- Exfoliative glaucoma patients should also be more frequently followed up than POAG patients, depending on the stage of the disease at presentation, as progression can occur more rapidly.
SUMMARY
PSEUDOEXFOLIATION GLAUCOMA |
|
Etiology:
|
Signs:
|
Symptoms:
|
Differentials:
|
Investigations:
|
Treatment:
|