
Chief Complaint:
A 12-year-old boy presented with redness and a decrease in vision in the left eye within four hours of injury with a top.
History of Present Illness:
Redness and decrease in vision in the left eye. No other significant complaint.
Past Ocular History:
No H/O any previous injury.
Past Medical History/ History of Medication:
No significant ocular past history for which he has used medications.
Family History:
No significant family history.
Review of Systems/Systemic Examination
The child was conscious, well oriented in time and space, afebrile, pulse rate was 88/min, respiratory rate was 16/minute. Examination of other systems were normal.
Ocular Examination
Best Corrected Visual Acuity (Snellen)
- Right eye (OD): 6/6
- Left eye (OS): 6/36 with pinhole – 6/18p
Ocular Motility/Alignment
Extraocular motility was full and free in all gazes in both eyes.
Intraocular Pressure (IOP)- By Applanation tonometry
- Right eye: 14mm
- Left eye: 16mm
Pupils:
Right eye - round and briskly reacting to light.
Left eye - Pharmacologically dilated but consensual present.
Slit-lamp exam:
- Lids/lashes:
Normal in both eyes.
- Conjunctiva/sclera:
Right eye - normal.
Left eye - showed circum corneal congestion, no evidence of tear in the conjunctiva or sclera.
- Cornea:
Clear in both eyes
- Anterior chamber:
Right eye - Normal and quiet
Left eye - normal in depth, cells2+, flare 2+, small blood clot inferiorly.
- Iris:
RE- normal in colour and pattern
LE- normal in colour, pharmacologically dilated, no evidence of sphincter tears.
- Lens:
Clear in both eyes. No evidence of subluxation or dislocation following trauma in the left eye.
Dilated Fundus examination
- Vitreous:
Clear in both eyes.
- Disc:
Size, shape, colour and margins normal in both eyes.
- Macula:
Right eye normal.
Left eye normal.
- Vessels:
Normal in both eyes.
- Retinal examination and Periphery:
Right eye – Normal
Left eye – Greyish-white opacification of the entire retina with an absence of the usual red reflex.
Ancillary Investigations:
Fundus photo and fundus photo montage
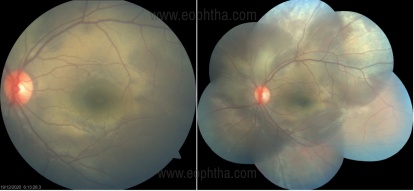
Within four hours of injury shows greyish-white opacification of the entire retina with loss of red reflex suggestive of commotion retinae.
Optical coherence tomogram (OCT)
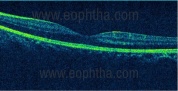
Cirrus HD OCT of the macula within four hours of injury
Clinical Course of the condition:
The patient was started on topical steroids and cycloplegics for traumatic iritis and hyphema. The patient reviewed 1 week later. The best-corrected visual acuity was 6/6 N6 in both eyes, iritis and hyphema had cleared in the left eye, intraocular pressure was 12mm and 14mm respectively in both eyes. Fundus examination showed resolution of commotio retinae and OCT showed return of the optical space and intact outer retinal layers.
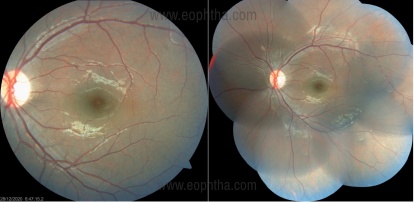
Fundus photo and fundus photo montage after 1 week showing resolution of commotion retinae.
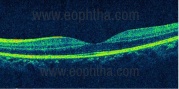
OCT showing intact outer retinal layers at 1-week post-injury.
Differential Diagnosis:
- Retinal detachment
- Choroidal rupture
- Retinal ischemia
- Traumatic macular hole
- Purtscher’s retinopathy
- Chorioretinitis sclopetaria
Diagnosis:
Commotio retinae secondary to blunt trauma
Discussion
Etiology/Epidemiology
It is usually following blunt injury or blast injury. The term was coined by Berlin describing it as opacification of the retina following blunt trauma. The damage is thought to be mechanical in nature due to the concussive force that is transmitted to the retina and choroid, particularly to the most sensitive and delicate photoreceptor outer segments. This can be by both and indirect mechanisms. It is estimated to be around 30% of all eye traumas presenting to the hospital. It mainly affects young males [1],[2],[3].
Pathophysiology
The concussive force following blunt trauma is transmitted to the retina and choroid, particularly affecting the delicate and sensitive photoreceptor outer segments. This has been shown in experimental models and invivo studies. The area of opacification or retinal whitening is thought to be secondary to increased scattering of light by the disrupted photoreceptor outer segments. Berlin proposed the concept of extracellular edema corresponding to the areas of retinal whitening [1],[5],[6],[7]. There is no clear cut evidence of a blood-retinal breakdown in commotion retinae [8].
The damaged photoreceptor cells degenerate within the first few days after injury. Restoration of photoreceptors can begin at 1 week and go on until few months. The damaged photoreceptor cells are cleared by the phagocytic cells from retinal pigment epithelium and the proliferating retinal pigment epithelial cells occupy the spaces left behind after phagocytosis [5],[6],[7].
Clinical Features
The patient presents with blurred vision, vision loss, field defect, or metamorphopsia. Examination shows opacification of the retina with the absence of the usual red reflex. Extramacular commoto retinae occur at the inferotemporal or temporal retina. A pseudo-cherry red spot may be seen if commotio retinae involve the fovea [4],[5]. OCT and OCT angiography findings are as described below. However, other signs of blunt trauma from the anterior to posterior segment should not be overlooked.
Investigation
OCT is very important in assessing the visual outcome. The damage occurs at the level of the photoreceptor outer segment and retinal pigment epithelial junction. In the acute stage, OCT shows hyperreflectivity of the ellipsoid zone with the disappearance of the thin hypo reflective space with loss of external limiting membrane in some areas. OCT in commotion retinae can be graded from hyperreflectivity of the ellipsoid zone to complete disruption of the photoreceptor layers. The disruption of the ellipsoid zone led to pigmentary and retinal atrophic changes causing poor visual outcome [2],[9],[10],[11].
OCT angiography shows decreased vessel density of the superficial, deep capillary, and radial peripapillary capillary plexus initially and returns to normalcy by 6 months [12],[13].
Treatment and Prognosis
There is no proposed treatment for commotion retinae. The outcome for this entity is promising without any treatment. However, there have been reports demonstrating the use of high-dose intravenous steroids to reduce retinal swelling. The recovery can be full to partial depending on the involvement of the macula. Macular involvement can cause mild visual impairment to severe visual loss or associated scotomatous areas. The theory of caspase activation leading to photoreceptor apoptosis has been established in the literature. Hence, intravitreal anti- caspase injections might prove effective in severe cases of commotion retinae [14],[15]. In cases of severe commotion retinae. OCT has been used to prognosticate the visual outcome. The greater the photoreceptor damage in OCT, the greater the visual loss in these patients [9].
Commotio Retinae |
|
|
Etiology
|
Signs
|
|
Symptoms
|
Differential diagnosis
|
|
Investigations Fundus photo, OCT macula |
Treatment
|
References
- Berlin R. Zur sogenannten commotio retinae, so called commotio reinae, Klin Monatsbl Augenheilkd. 1873;(11):42-78.
- Sony P, Venkatesh P, Gadaginamath S, Garg SP. Optical coherence tomography findings in commotio retina. Clin Experiment Ophthalmol 2006; 34:621–3.
- Leshno A, Alhalel A, Fogel-Levin M, Zloto O, Moisseiev J, Vidne-Hay O. Pediatric retinal damage due to soccer-ball-related injury: results from the last decade. Eur J Ophthalmol. 2019. doi:10.1177/1120672119882332.
- Blanch RJ, Good PA, Shah P, Bishop JRB, Logan A, Scott RAH. Visual outcomes after blunt ocular trauma. Ophthalmology. 2013. doi: 10.1016/j.ophtha.2013.01.009.
- Mansour AM, Green WR, Hogge C. Histopathology of commotio retinae. Retina. 1992. doi:10.1097/00006982-199212010-00006.
- Liem ATA, Keunen JEE, Norren D Van. Reversible cone photoreceptor injury in commotio retinae of the macula. Retina. 1995. doi:10.1097/00006982-199515010-00011.
- Sipperley JO, Quigley HA, Gass JDM. Traumatic retinopathy in primates: the explanation of commotio retinae. Arch Ophthalmol. 1978. doi:10.1001/archopht.1978.03910060563021.
- Hart, J.C. and R. Blight,Commotio retinae.Arch Ophthalmol, 1979.97(9): p. 1738.
- Ahn SJ, Woo SJ, Kim KE, Jo DH, Ahn J, Park KH. Optical coherence tomography morphologic grading of macular commotio retinae and its association with anatomic and visual outcomes. Am J Ophthalmol 2013;156 994_1001.e1.
- Oh J, Jung J-H, Moon SW, Song SJ, Yu HG, Cho HY. Commotio retinae with spectral-domain optical coherence tomography. Retina 2011;31(10):2044–9.
- Souza-Santos F, Lavinsky D, Moraes NS, Castro AR, Cardillo JA, Farah ME. Spectral-domain optical coherence tomography in patients with commotio retinae. Retina 2012; 32:711–8.
- Mansour AM, Shields CL. Microvascular Capillary Plexus Findings of Commotio Retinae on Optical Coherence Tomography Angiography. Case Rep Ophthalmol. 2018 Nov 27;9(3):473-478. doi: 10.1159/000494916.
- Montorio D, D'Andrea L, Cennamo G. Retinal Vascular Features in Ocular Blunt Trauma by Optical Coherence Tomography Angiography. J Clin Med. 2020 Oct 16;9(10):3329. doi: 10.3390/jcm9103329.
- Blanch RJ, Ahmed Z, Thompson AR, et al. Caspase-9 mediates photoreceptor death after blunt ocular trauma. Investig Ophthalmol Vis Sci. 2014. doi:10.1167/iovs.13-13708.
- Thomas CN, Thompson AM, McCance E, et al. Caspase-2 mediates site-specific retinal ganglion cell death after blunt ocular injury. Investig Ophthalmol Vis Sci. 2018. doi:10.1167/iovs.18-24045.