
INTRODUCTION:
There are several definitions for dry eye available in world literature. The one that I prefer is the following: Dry eye is a disease in which there is a qualitative and /or quantitative decline in the tears accompanied by disorders of the ocular surface.
The new definition proposed by the Dry Eye Workshop (DEWS) in 2006-07 states: Dry eye is a multifactorial disease of tear film & ocular surface resulting in symptoms of ocular discomfort, visual disturbance and tear film instability with potential damage to the ocular surface. This is associated with hyperosmolarity of the tear film and inflammation of ocular surface
It is important that dry eye is recognized as a disease entity and not merely regarded as a nuisance. This definition also makes clear that one can have dry eye even in the presence of epiphora, as the quality of the tears may be inadequate to provide lubrication, with normal quantity of tear production. Also, even if the quality and quantity of tears is initially adequate, if the ocular surface is altered, the tears will not spread evenly across the surface, leading to dry eye. This has been recognized by a panel of experts in 2006-07 meeting at Delphi and endorsed at the Dry Eye Workshop (DEWS) in the United States. They proposed a new terminology for Dry Eye, preferring to refer to it as “Dysfunctional Tear Syndrome” or DTS.
COMMON (NON-PATHOLOGICAL) CAUSES OF DRY EYE ENCOUNTERED IN DAILY PRACTICE.
For convenience of recollection, I label these as ABCDE where:
A= ageing disorders,
B= blinking disorders,
C= Contact lens related dry eye,
D=drug related dry eye and
E= environmental causes for dry eye.
Let us examine each one in detail.
A =AGEING
Aqueous tear production is 60% less at age of 65 years as compared to that of an 18-year-old. This does not mean that all elderly patients will develop dry eye. However, an elderly person who has no symptoms of dryness can easily become symptomatic in case of change of environment e.g. increase of pollution or excessive use of airconditioner or by being prescribed certain drugs such as beta blockers for hypertension as these are known to reduce tear production. An elderly patient who undergoes an uneventful cataract surgery may complain of a little irritation or soreness post-operatively. Often these symptoms are mistaken for inflammation or infection and he is prescribed increasing doses of steroids or local antibiotics. The active constituents in these eye drops, as well as the preservatives in them both, exacerbate a subclinical dry eye, which was the root cause of his symptoms. If the ophthalmologist is confident that the surgery has gone off uneventfully, it would be wiser to add ocular lubricants (especially preservative free ones) to the treatment schedule and actually reduce the frequency of local antibiotics and steroids. I re-iterate that there has to be a high level of suspicion of dry eye for any unexplained symptoms of soreness or grittiness in a senior citizen, especially one that has been recently operated.
B = BLINKING DISORDERS
Our tears are spread evenly over the entire ocular surface with each blink of the lids, rather like the windshield wiper effect. Besides, optimum blink rate is essential to prevent excessive evaporation of the tears. Tears evaporate from the ocular surface whenever the eyes are open – hence when the blink frequency reduces, there is increased evaporation, resulting in relative dryness. This is what happens for example, in people who spend several hours each day in front of the computer terminal. They tend to stare at the screen, with such concentration, that their blink rate falls by 50% or even more, according to several published studies. At the end of the day, their eyes feel tired, sore and they often don’t feel like doing any visual activity on coming home from work. They may even develop mild ocular congestion, for which they are mistakenly prescribed vasoconstrictor eye drops or even antibiotic-steroid combination drops. They are suffering from what is known as “Computer Vision Syndrome (CVS)”. All they need is to be made aware of their condition. They are asked to blink more often while at work. Surprisingly, even though blinking is an involuntary reflex, these intelligent patients are able to increase their blink rate to near normal simply by remembering to blink frequently. In the initial period, of course, they may need to be put on a short course of lubricant eye drops. It is important to educate them on using these lubricant drops rather than splashing tap water from the nearest washbasin into their eyes. Tap water may not be very clean – its frequent use may cause conjunctivitis. Besides, the lubricant drops mimic our natural tears much better than plain water and hence give greater comfort and are less harmful to the eyes in the long run.
Another type of blink disorder is often seen in young children. Parents often complain that their child has frequent blinking of eyes. After a complete eye examination and ruling out refractive errors, we often just reassure the parents that the child will grow out of this symptom. Most often we are right. However, if the habit persists, the child can develop a mild dry eye, as the tears do not have the time to spread evenly between blinks, thus causing uneven surface wetting. These patients too may benefit from a short course of ocular lubricants.

Fig. 1. Dry eye with mild photophobia
C = CONTACT LENS RELATED DRY EYE
Contact lenses – hard, soft or gas permeable increase the surface area from which tears evaporate. They also tend to disrupt the stability of the tear film, in ways not fully understood. This of course does not happen to all contact wearers – only a small minority of them will develop mild to moderate dry eye. However, a contact lens wearer going into a polluted environment or working for long hours continuously on the computer, or working in an air-conditioned area is more predisposed to develop dry eye. This is seen, for example, in airhostesses, working on long haul flights. The passenger cabins are designed to make the passengers feel comfortable, by lowering the temperature and the humidity levels considerably. Both these factors cause increased evaporation of tears, more so from the eyes of a contact lens wearer. Many of these young women therefore complain of irritation or soreness of eyes at the end of the flight. It is wise to ask them to use lubricant drops frequently on top of their lenses while in flight. Drops containing polyvinyl alcohol and/or polyvinyl pyrrolidone can safely be put in the eyes and do not damage the lenses.
Again here, being alert to the possibility of dry eye in a contact lens wearer will make it easier for the eye surgeon to resist the temptation of prescribing new contact lenses every time a contact lens wearer complains of discomfort with the existing pair. It will also prevent needless prescription of steroids and NSAID drops for imaginary findings of giant papillary conjunctivitis, when all that is required in most cases is ocular lubricants.
D = DRUGS CAUSING DRY EYE.
Several commonly used medications taken orally result in mild to moderate dry eye, chiefly by affecting the production of the aqueous component of tears. Among them are several antacids, antihistaminics, NSAIDs, some anti-hypertensives (calcium channel and beta-blockers), drugs used for depression and for treatment of Parkinsonism as well as some of the drugs used for HRT (hormone replacement therapy) for menopausal symptoms. Also several eye drops such as steroids and beta-blockers used for glaucoma are known to produce mild dry eye. However, many a time it is not the active constituent of the eye drop, but the preservative, which can prove toxic in the long run to the surface epithelium, exacerbating the symptoms of dry eye. Hence when prescribing any eye drops including ocular lubricants which are likely to be used for a prolonged period of time, it is wise to pay some attention to the preservative content of the drops. The 4 main preservatives used today are benzalkonium chloride, thimerosal, phenyl mercuric nitrate and chlorbutanol. Of them chlorbutanol is least toxic to the epithelium, while benzalkonium chloride is the most toxic. If one is keen to use drops containing benzalkonium, it may be a good idea to substitute with a different brand containing a different preservative for some time and switch back to the drop containing benzalkonium later. In this way, one can prevent continuous exposure to the deleterious effect of one preservative. In case the patient requires drops to be instilled more than 4 to 6 times a day for a prolonged period, for example a severely dry eye patient, it is better to prescribe drops with disappearing preservative or preservative free drops.

Fig. 2. Lacrimal plugs (Herrick)
E= ENVIRONMENTAL CAUSES OF DRY EYE
Most of us are well aware that dry, windy or dusty, hot climates are likely to exacerbate dry eye disease. Workers in chemical factories or those exposed to toxic fumes are also more prone to develop mild dry eye or worsen a pre-existing dry eye. What we often fail to realize is that all of us who work in air-conditioned rooms (including most ophthalmologists) are also likely to fall prey to this disease. All air-conditioners work at making the occupant s of the room comfortable by not only lowering the ambient room temperature, but by markedly lowering the room humidity. This causes decreased sweating and makes the body feel comfortable. However, what is comfortable for the body is not comfortable for the eye! Decreased room humidity causes increased evaporation not only of sweat (desirable) but also of tears (undesirable). When this is combined with other factors, for example, a myopic computer software programmer working 14 hours a day on his computer screen with his contact lenses on, you have a surefire recipe for dry eye! Simple attention to seeing to it that the air draft from the AC is not directed on your face, turning the AC temperature control to the maximal tolerable for comfort, taking breaks during work, when the eyes are kept closed will go a long way in preventing the hazard of dry eye. For those who can afford it, one can keep a humidifier in the room. This controls the room humidity to desired levels, preventing the room air from becoming too dry. This can be used with both AC as well as heaters.

Fig.3. Severe lid inflammation (meibomitis) with dry eye
Symptoms of DTS
Watering (Epiphora). This is present in 20% of patients of dry eye. This watering is due to reflex tears produced because the ocular surface is irritated due to dry eye. Unfortunately, these reflex tears have poor lubricating qualities.
Feeling of dryness, sandy sensation, grittiness, and foreign body sensation. In those with CVS, these symptoms are often worse at the end of the day, especially in those spending long hours on the computer. The symptoms often disappear on Sundays and public holidays.
Photophobia and disorders of blink mechanism.
Frequent attacks of mild redness, occasional discharge, fluctuating vision with occasional blurring.
Signs of DTS
Decreased lower tear meniscus: Look at the height of the lower tear film meniscus above the lower lid on the slit lamp. Take 100 normal asymptomatic elderly patients on slit lamp and do this examination. You will then get a good idea of ‘normal’ height. If you then come across a symptomatic patient, check for the height of the meniscus, with a suspicious mind. Do not go by textbook definition of 1mm or 0.5mm. It depends on your slit lamp and the magnification you are using!
Debris in tear film: Look for evidence of mucous, strands, in the tears. Normal tears do not have visible debris – if any are present, it is highly likely that the patient has DTS.
Mucous Fishing Syndrome: Many patients develop a habit of constantly pulling out stringy mucous from the corners of their eyes or rubbing their eyes at the corners, due to the constant presence of mucous especially near the medial canthus. If a patient does this in front of you, or you observe a collection of mucous near the medial canthus, suspect DTS.
Squamous Blepharitis: There are tiny flakes at the lash margins or in later stages, crusting and matting of the eyelashes. This may or may not be accompanied by scalp dandruff.
Meibomitis: The opening s of the meibomian glands may be inflamed. There may also be increased vascularisation in the area. Attempts to squeeze out an oil droplet may result in a ‘toothpaste’ effect or if the opening is blocked, there may be no oil droplet release. Both Squamous blepharitis and Meibomitis are more common in Indian eyes than in Caucasian eyes. These 2 conditions also tend to recur; hence they must be looked out for in every patient visit.

Fig. 4. Early OCP with symblepharon

Fig.5. Filamentary Keratitis
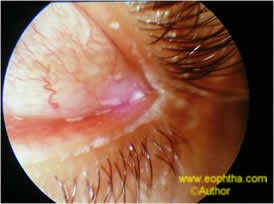
Fig: 6. Mucous and debri in tear film

Fig:7. Mucous strands, cause “mucous fishing” syndrome
Current Management Principles for DTS patients
1. Tear conservation: This aims to preserve the patient’s own tears as much as possible. This can be done by:
a) wearing swimmer’s goggles. This decreases evaporation from the eyes by 14%. However, almost all your patients will refuse to wear these on cosmetic grounds.
b) Use of Punctum and canalicular plugs. These block the egress of the patient’s own tears from the eye as well as allow lubricant eye drops to stay in the eye longer. They can be inserted in the office of the eye surgeon or in the Operation theatre in a simple 5-minute procedure, without any injection anaesthesia. However, these must be inserted only in moderate dry eye, once the inflammatory component of dry eye is controlled with use of topical cyclosporine drops for at least 2 months. Otherwise, the plugs will only cause the patient’s own ‘hot’ tears, rich in inflammatory cytokines to remain in the eye for longer, thus perpetuating the vicious cycle of sub clinical inflammation.
c) Life-style changes. These have been alluded to in the discussion on computer vision syndrome i.e. asking the patient to blink more often and to close his eyes for a few seconds at regular intervals of 20-30 minutes when on the computer terminal. This also means asking patient’s not to work in polluted environments or reduce exposure to dust and chemicals – easier said than done! Those always in air-conditioned environments, should be asked to turn the draft away from their faces, keep the room at optimum temperature and if required, install a small room humidifier in the room to increase the room humidity, to reduce tear evaporation.

Fig:8. S-J Syndrome with keratinisation
2. Tear Supplementation.There are a plethora of lubricant eye drops and ointments available in the market today, a far cry from a decade ago, when only methylcellulose drops were available. The main ingredients in these are polyvinyl alcohol (PVA), polyvinylpyrrolidone (PVP), sodium hyaluronate and cousins of methylcellulose such as hydroxypropylmethyl cellulose (HPMC), carboxymethylcellulose (CMC). Some of these are preservative free; some are with ‘friendly’ preservatives that are broken down into non-toxic components on exposure to light or the enzymes of the eye, on instillation. The latter are useful in moderate to severe DTS, when the patient needs to instill drops more frequently.

Fig: 9. Squamous blepharitis –severe
3. Osmo Protection.The ocular surface in a patient with DTS is subjected to osmo-stress. The lack of water makes the surface hyper osmotic. This causes the surface to suck out water from the underlying Conjunctival and Corneal epithelium causing their apoptosis or premature cell death. A new class of tear supplements contains small molecules such as L-carnitine, glycerol etc, known as “compatible solutes”. These slip through tiny openings in the epithelial cell wall called ‘aquaporins’ and enter the cell cytoplasm. Once there, they hold onto the intra cellular water, preventing it from leaving the cell, thus prolonging the life of the cell. Since these compatible solutes prevent osmotic damage to the cells in spite of a hostile environment, they are known as osmo-protectants’. Most of these eye drops in addition contain carboxymethylcellulose and a disappearing preservative
4. Increasing Tear Production.Since the last few years, topical Cyclosporine drops are available in preservative free single dose containers. These increase the production of tears by the lacrimal glands in patients with mild to moderate dry eye. They act on the neuro-hormonal mechanism down regulating the inflammatory component and apoptosis of epithelial cells and up regulating the apoptosis of inflammatory white blood cells The flip side is they are a bit expensive and need to be continued twice a day for a minimum of a year to 2 years.
Oral Pilocarpine tablets are also available in India and are said to increase the production of tears. Unfortunately they also increase the production of saliva, sweat and urine, causing bodily discomfort in some patients.
5.Surgical TreatmentDry eye patients are more prone to ocular infections, which must be promptly and aggressively treated to prevent complications. If the dry eye is due to systemic conditions such as pemphigoid or Stevens-Johnson syndrome, there may be formation of symblephara, which may need excision and amniotic membrane grafting. If both eyes are blind due to severe dryness, with opaque, vascularised corneas, corneal grafting is contra-indicated. In such seemingly hopeless cases, artificial corneas or Keratoprosthesis such as the Pintucci Keratoprosthesis (of which the author has done over75 cases since 1997) or the MOOKP can help to restore vision

Fig 10: 5 years post Pintucci Keratoprosthesis in a S-J patient with vision 6/18
CONCLUSION:
By being more aware of the common (ABCDE) causes of dry eye in the normal population, simple tips and increasing patient awareness can go a long way in ameliorating the problem without the need for ocular lubricants in many cases. In those that need treatment, lubricant medication is available over the counter and is harmless in most cases. All patients with external ocular symptoms such as sandy feeling, itching, grittiness, foreign body sensation, occasional redness, feeling of tiredness, soreness, even watering (in 20% of dry eye patients) should be suspected to have dry eye and treated as such. It must be emphasized that family physicians should resist the temptation of treating every red eye as conjunctivitis or inflammation, with antibiotics or steroids. Often these worsen pre-existing dry eye.