


Allergic conjunctivitis, which includes a spectrum of clinical entities is one of the most common conditions with which patients present to a general ophthalmologist. They include milder forms like seasonal and perennial allergic conjunctivitis as well as severe forms like vernal and atopic which can be sight-threatening.
In spite of common clinical and immunological features vernal keratoconjunctivitis differs from the rest in myriad ways. (1)This article brings forth five most pertinent points which will not only improve the understanding but also help identify and manage it.
1. Vernal keratoconjunctivitis can have three distinct forms
Vernal keratoconjunctivitis (VKC) is a bilateral, chronic, usually seasonal, recurrent allergic inflammation of the conjunctiva. It mainly affects boys living in tropical countries in their first or second decade of life, mostly seasonal but in tropical countries, it can be perennial too. In the temperate regions, in many parts of Africa, Latin America and Asia; VKC represents an important cause for hospital attendance, ranging from 3% to 6% of patients of all ages, rising to 33% and 90% in children and adolescents. (1)
There are 3 distinct forms of the disease: tarsal (giant cobblestone papillae in the tarsal conjunctiva ), limbal (gelatinous limbal infiltrates ) and mixed (has features of both tarsal and limbal forms ). Palpebral forms are more prevalent in Europe and America, whereas mixed and limbal forms are seen in Asia and Africa respectively. In the Indian subcontinent majority of patients have mixed form of the disease (72%) with almost 36% having it perennial.(2)
2. Vernal keratoconjunctivitis is type 1 along with a type 4 hypersensitivity reaction
VKC has always been considered as IgE-mediated type 1 hypersensitivity reaction. A family or personal history of systemic allergies like atopic dermatitis, asthma, rhinitis is a common feature. Recently however reports have confirmed a non-Ig E mediated mechanism also which is mainly T cell-mediated. Ig E mediated is the immediate /early phase reaction where already sensitized mast cells with Ig E coated on their surface on exposure to the antigen get sensitized and release preformed mediators which is followed by a late phase reaction by the release of newly formed mediators(cytokines/chemokines )from mast cells . The late phase reaction can occur between 6-24 hours after the early phase and is associated with leucocytic influx. However, the non-Ig E /T cell-mediated is like a persistent late-phase reaction where presenting an antigen (Ag) with the help of antigen-presenting cells (dendritic cells) binds to CD4 T cells and result in the production of Th2 cells and its cytokines. These cytokines also cause Ig class switching and result in localized production of Ig E which binds to mast cells and causes the release of mediators.(3,4)
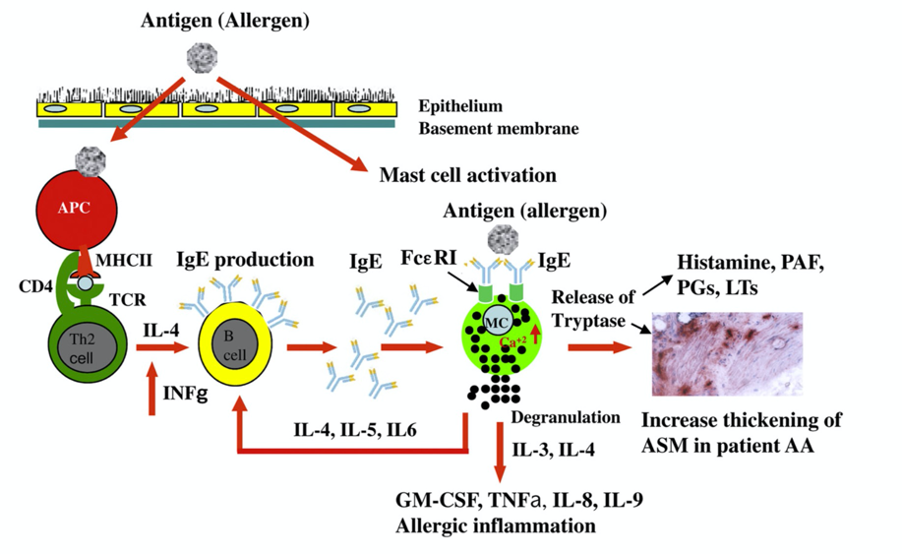
Fig 1: Induction and Effector Mechanisms in Type 1 Hypersensitivity (Courtesy: Kawa Amin .The role of mast cells in allergic inflammation Respiratory Medicine (2012);106, 9-14 )
3. We should look for and prevent corneal complications in Vernal Keratoconjunctivitis
Itching is the foremost symptom with which the patient presents along with watering, photophobia, mucoid ropy discharge, blepharospasm, and foreign body sensation.
On ocular examination, during an active stage, it can present as purely tarsal, limbal or mixed. Based on the pattern one can find papillary reaction on the tarsal plate with papillae ranging from 0.1mm to giant cobblestone papillae, more frequently in upper than lower or gelatinous limbal hypertrophy. Aggregates of epithelial cells and eosinophils at the limbus called the Horner Tranta’s dots and conjunctival hyperemia also indicate an active stage of the disease. Corneal involvement is mostly noted in the tropical belts and includes superficial punctate keratopathy, shield ulcers, and neovascularization.
In addition to the above, a pigmented perilimbal bulbar conjunctiva has been documented as one of the diagnostic signs, especially in the Asian population.
In the chronic stage of the disease pseudogerontoxon, subconjunctival fibrosis, corneal scarring, keratoconus, and limbal stem cell deficiency have been reported. Complications like keratoconus (6-8%) and limbal stem cell deficiency (2-4%) are more in tropical areas with the severe perennial form of the disease. Based on the above signs and symptoms Bonini et al proposed a classification to help diagnose and manage patients more uniformly. (5)
|
VKC grading |
Symptoms |
Conjunctival Hyperemia |
Conjunctival congestion |
Papillary reaction |
Trantas Dots |
Corneal involvement |
|
Grade 0 ( Quiescent) |
Absent |
Absent/mild |
Absent |
Mild to moderate |
Absent |
Absent |
|
Grade 1 (mild intermittent) |
Mild to occasional |
Mild |
Absent/mild |
Mild to moderate |
Absent |
Absent |
|
Grade 2 A ( moderate intermittent) |
Mild to moderate intermittent |
Mild |
Mild |
Mild to severe |
Absent |
Absent |
|
Grade 2B (moderate persistent ) |
Mild to moderate persistent |
Mild to moderate |
Mild to moderate |
Mild to severe |
Absent |
Superficial punctate keratitis may be present |
|
Grade 3 (severe) |
Moderate to severe persistent |
Moderate to severe |
Moderate to severe |
Moderate to severe with injection and swelling |
Few are present |
Superficial punctate keratitis |
|
Grade 4 (very severe) |
severe and persistent |
Moderate to severe |
severe |
Moderate to severe with injection and swelling |
Numerous |
Corneal erosion or ulceration |
|
Grade 5 (evolution) |
Absent or mild occasional |
Absent/mild |
Absent |
Mild to moderate |
Absent |
Absent |
4. It is very important to differentiate Vernal Keratoconjunctivitis from other forms of allergic conjunctivitis.(4)
|
Seasonal allergic conjunctivitis |
Perrineal allergic conjunctivitis |
Vernal keratoconjunctivitis |
Atopic keratoconjunctivitis |
|
|
Immunopathogenesis |
IgE mediated |
IgE mediated |
IgE and Tcell mediated |
IgE and Tcell mediated |
|
Photophobia |
- |
- |
+ |
+ |
|
Itching |
+ |
+ |
++ |
++ |
|
Giant cobblestone papillae |
- |
- |
+ more on the upper tarsus |
+ on the lower tarsus |
|
Age |
Any age |
Any age |
5-15 years |
20-40 years |
|
Recurrence |
Seasonal during spring /summer |
Throughout the year |
Seasonal / perennial |
Perennial |
|
Cicatrical changes |
Absent |
Absent |
Almost nil |
Present |
|
Sight threatening |
No |
No |
Yes |
Yes |
5. Reduction in frequency of acute attack plays a key role in the management of Vernal Keratoconjunctivitis
Management of patients with vernal keratoconjunctivitis has 2 arms: disease and treatment-related. Aims of managing the disease-related arm include reducing the frequency of active episodes and preventing or curtail the occurrence of complications related to the disease like keratoconus, shield ulcer or limbal stem cell deficiency. Since steroids are an important and frequently advised treatment option, the complications related to its long term use need to be dealt with along with ways to reduce steroid dependency.
|
Grade of VKC |
Treatment plan |
|
Grade 0 (Quiescent ) |
No treatment |
|
Grade 1 (Mild intermittent ) |
Occasional Anti-allergic drops |
|
Grade 2 (Moderate) A ( Intermittent) B (Persistent ) |
Daily administration of dual-action antiallergic drops + pulsed topical steroids + Cyclosporine A eye drops |
|
Grade 3 (Severe) |
Daily administration of dual-action antiallergic drops + pulsed topical steroids + Cyclosporine A eye drops |
|
Grade 4 (Very Severe) |
Daily administration of dual action antiallergic drops + pulsed high dose topical steroids + Cyclosporine A eye drops |
|
Grade 5 ( Evolution) |
Occasional anti-allergic drops |
Educating the patient and the family regarding the chronicity of the disease, avoiding aggravating factors, prohibit inadvertent use of steroids are the primary aims of treatment. Bonini et al proposed a stepwise tailored approach in managing the disease based on their classification. Fig 2
Once the disease is under control, complications can be better managed. In children with VKC with keratoconus, early collagen cross-linking is recommended once the eye quietens down to prevent further diminution of vision. Since rigid contact lens might rub against the limbus and fitting of soft contact lens might be a concern in this group, PROSE lenses can be considered for visual rehabilitation as well as in patients with limbal stem cell deficiency. The use of steroid-sparing agents like cyclosporin and tacrolimus will help reduce steroid dependency and complications with their prolonged use.
To summarise, VKC is not a rare allergic disorder especially in tropical countries, and reducing the frequency of episodes will help reduce the functional and social morbidities sensitization is definitely a primary factor but T cell-mediated cytokines also have a significant role to play in its pathogenesis. Despite improved understanding of etiopathogenesis, steroids and mast cell stabilizers still form the mainstay of treatment along with immunomodulators but are often not enough in controlling severe cases and preventing complications.
References :
- De Smedt S, et al. Vernal keratoconjunctivitis: an update. Br J Ophthalmol 2013;97:9–14.
- Anthony VD,et al.Allergic disease in children and adolescents seeking eye care in India:Electronic medical records driven big data analytics report II. The Ocular Surface.doi.org/10.1016/j.jtos.2019.08.11
- Kawa Amin .The role of mast cells in allergic inflammation Respiratory Medicine (2012) ;106, 9-14
- Mark BA,et al . Ocular Allergic Disease: Mechanisms, Disease Sub-types, Treatment . The Ocular Surface ;2003( 1), 127-149.
- Stefano B, et al. Clinical grading of vernal keratoconjunctivitis. Current Opinion in Allergy and Clinical Immunology 2007, 7:436–441